Providing opioid use disorder medications in jails: Results from a randomized study in 67 communities
Initiating medication treatment for opioid use disorder in criminal justice settings and linking to medication services upon release can reduce overdose. However, less than half of jails in the US offer such medication treatment. This study investigated the impact of a large-scale intervention designed to support communities in implementing evidence-based practices, such as expanding medication treatment and linkage.
The Communities that Heal intervention was designed to reduce overdose deaths by supporting communities in implementing evidence-based practices of their choice, including, but not limited to, medication treatment for opioid use disorder in criminal justice settings. This intervention was evaluated by the HEALing (Helping to End Addiction Long-term) Communities Study, which randomized communities to either receive the intervention or to be waitlisted as part of the control group. Communities that were randomized to the intervention group received the intervention from January 2020 to June 2022.
This study focused on whether communities randomized to the intervention group had more jails that expanded the provision of medications for opioid use disorder than communities in the control group. They were also interested in whether the intervention communities had more jails that linked people to medication treatment upon being released from jail. Such research can shed light on whether interventions designed to support communities in implementing evidence-based practices for reducing overdose deaths, such as the Communities that Heal intervention, expands access to medication treatment for opioid use disorder in criminal justice settings and increases linkage to medication services following release.
HOW WAS THIS STUDY CONDUCTED?
This study examined whether communities assigned to the intervention group, as part of the Communities that Heal study, had more jails that provided medications for opioid use disorder in jails and linked people to medication treatment upon release more than the communities’ jails assigned to the control group. These outcomes were assessed with a survey administered in jails within the 67 communities that were part of the study.
This survey was administered at 3 time points. For the first time point, data was collected as part of the Justice Community Opioid Innovation Network (JCOIN) and the HEALing Communities Study, which administered the survey to jail administrators in 2018 and 2019. Survey questions assessed the availability, accessibility, and use of interventions to treat opioid use disorder in jails during the prior 12 months. For the second and third time points, data was collected as part of the HEALing Communities Study. Data for the second survey was collected between 7/1/2020 and 6/30/2021, while data for the third survey was collected between 7/1/2021 and 6/30/2022. However, this study only used data from the first and third time points in their analyses.
The 2 primary outcomes of interest included the impact of the intervention on whether communities had jails: (1) that started people with opioid use disorder on medication treatment during their incarceration and/or immediately prior to their release, and (2) linked people to medication for opioid use disorder treatment upon their release. The researchers categorized jails as providing medications for opioid use disorder if jail administrators answered yes to 1 of the 2 following questions: “Is (buprenorphine, methadone, or naltrexone) used for induction and treatment during incarceration?” or “Is (buprenorphine, methadone, or naltrexone) used for pre-release induction?” The researchers also categorized jails as linking people to medication treatment upon release if the jail administrators reported that their jail provides 1 or more re-entry or continuity of care services, such as scheduling appointments with medication providers in the community or helping with completing intake paperwork for medication treatment. The researchers were also interested in the type of medication for opioid use disorders that the jails offered as a secondary outcome (buprenorphine, methadone, or naltrexone).
Analyses included descriptive statistics to summarize the frequencies, percentages, and means of jail characteristics and primary outcomes. Then models tested the impact of the intervention on each outcome at the third time point (i.e., the evaluation period, which was between 7/1/2021 and 6/30/2022). Only communities that responded to the first and third surveys were included in the analyses.
The 67 communities that participated in the HEALing Communities Study included 16 research sites across Kentucky, Massachusetts, and New York, each, and 19 research sites in Ohio. Of these, 57% of the communities were urban and 43% were rural.
There were 8.2 million adults estimated to populate the 67 communities. Of these, 31% were between the ages of 18-34, 31% were between 35-54, and 39% were 55 years old or older. The majority identified as non-Hispanic White (73%). For the remaining races/ethnicities, 16% identified as non-Hispanic Black, 4% identified as non-Hispanic Other, and 7% identified as Hispanic. People in the communities were approximately half men (48%) and half women (52%). The 67 communities in the study were randomized to either the intervention group (34 communities) or to the control condition that were waitlisted to receive the intervention (33 communities).
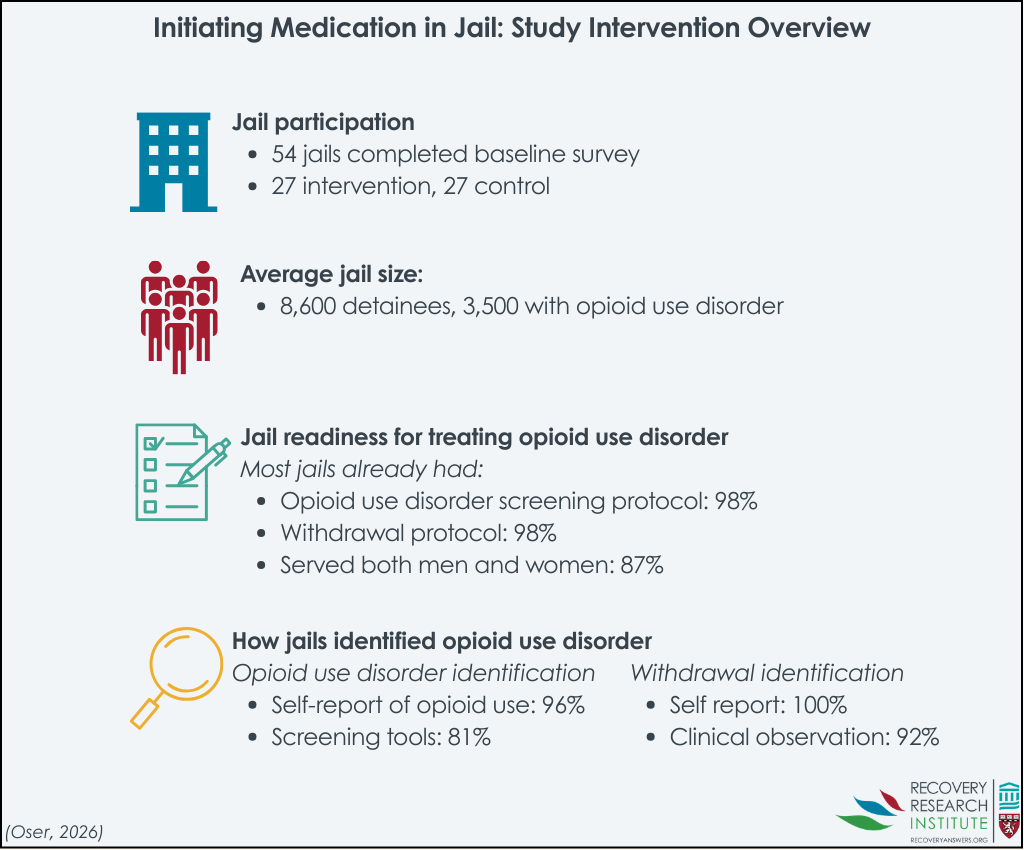
Of the 67 communities, administrators from 54 jails returned the baseline survey, with 27 from the intervention group and 27 from the control group (see graphic below for a summary of the study procedures). It is unclear from the study how many jails were offered the baseline survey but did not take it because the response rate was not reported in the study. It is possible that jails which did not respond were less likely to provide, or link to, opioid use disorder medication at baseline and may not have been open to changes in their medication policies. If that was the case, and these types of jails were more likely to be in the intervention versus control group, study effects may be overestimated. If these types of nonresponders were more likely to be in the control group, study effects may be underestimated. Jails that did return the survey included 15 sites from Kentucky, 11 from Massachusetts, 12 from New York, and 16 from Ohio. Among these, the jails had an average of approximately 8,600 detainees, of which approximately 3,540 had an opioid use disorder. The majority of these jails served both males and females (87%), had a screening protocol in place to identify people who may have opioid use disorder (89%), and had a standardized protocol in place to identify people experiencing opioid withdrawal (98%).
The most commonly reported methods for identifying people with an opioid use disorder were the self-reported number of days using opioids (96%) and use of a screening tool for substance use disorders (81%; primarily an agency-created screening tool with 77% of jails reporting use of this type of screening tool). The most commonly reported tool for identifying people experiencing opioid withdrawal were self-report (100%) and clinical observation (92%).
WHAT DID THIS STUDY FIND?
At baseline, slightly more control communities’ jails started people on medication for opioid use disorder and linked them to medication treatment upon release
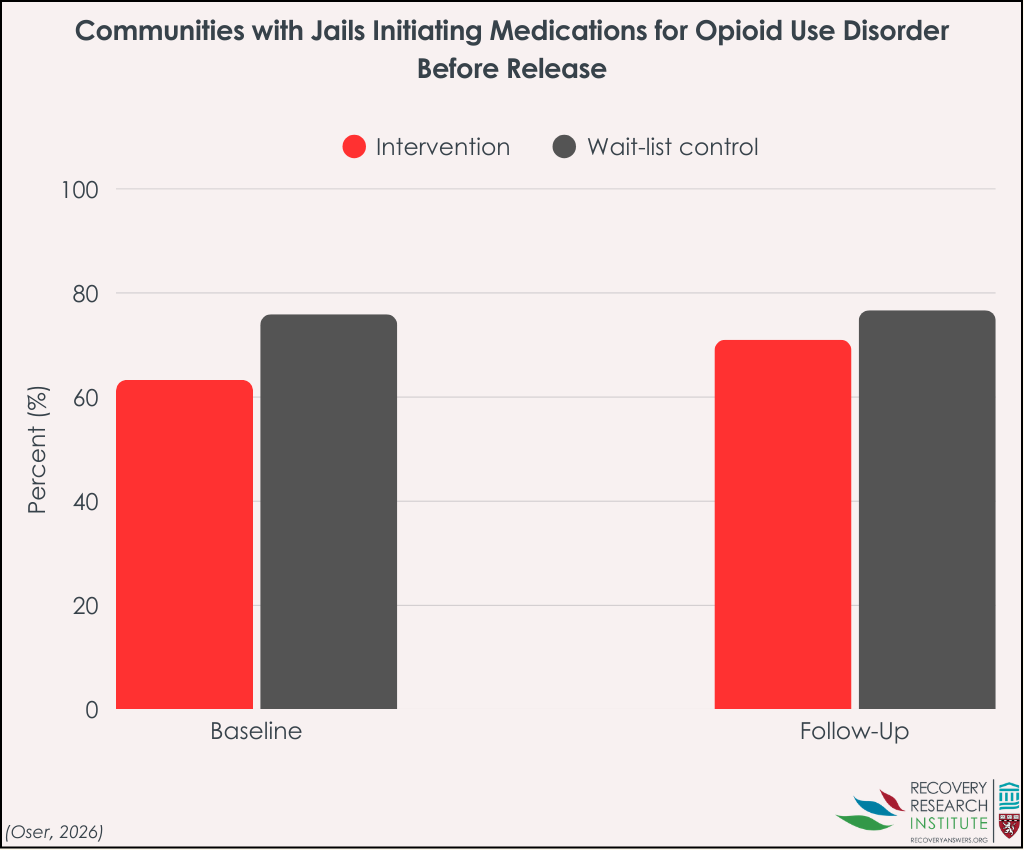
At the baseline survey, there were slight differences in the percentages of communities with jails that started people with opioid use disorder on medication treatment and linked them to medication treatment upon release. More communities in the waitlisted control group had jails that started people on medication treatment during incarceration or immediately prior to release (76%) compared to communities in the intervention group (63%).
Specifically, more communities in the waitlisted control group had jails that started people on buprenorphine, methadone, and naltrexone during incarceration or immediately prior to release, with percentages of 24%, 7%, and 76%, respectively. This is compared to 10%, 0%, and 63% of intervention communities having jails who initiated these medications, respectively.
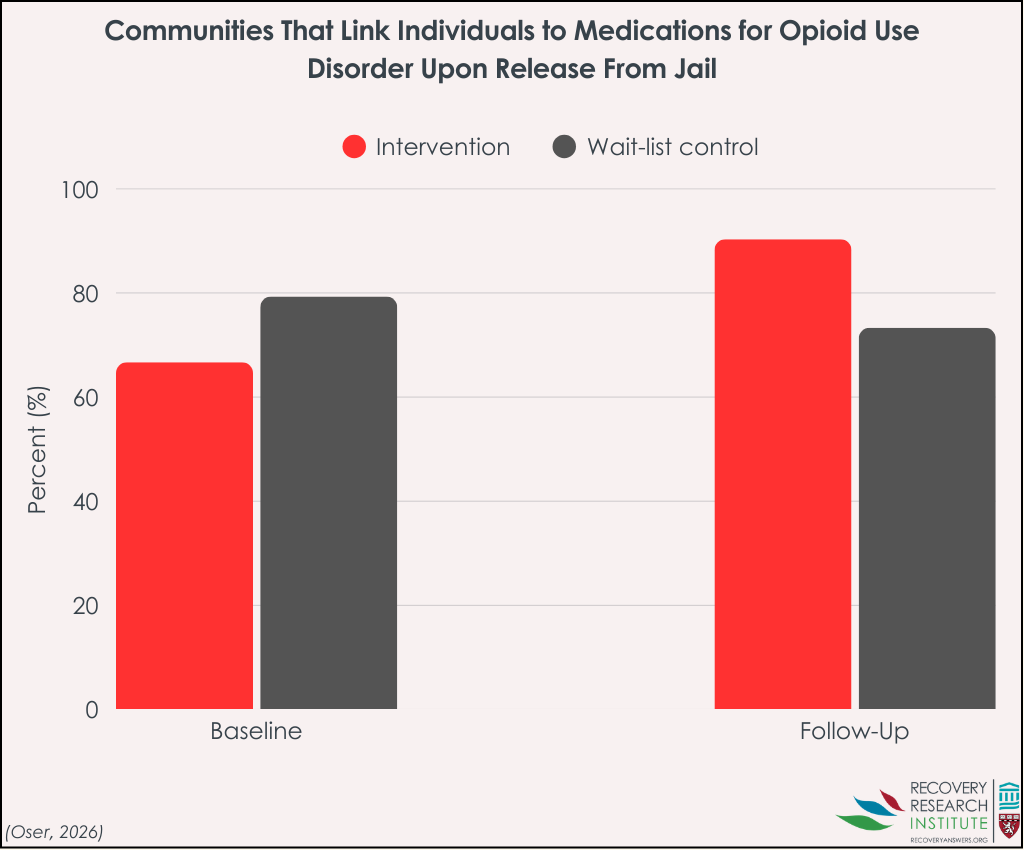
Likewise, more communities in the waitlisted control group had jails that linked people to medication treatment upon release (79%) compared to communities in the intervention group (67%). The most commonly reported linkage services provided by the jails were scheduling appointments with providers in the community (61%), facilitating the exchange of information with a medication provider in the community (60%), and helping to complete intake paperwork (59%).
There was no impact of the intervention on outcomes
At the third time point (during the evaluation period), fewer communities in the intervention group had jails that started people on medication for opioid use disorder during their incarceration or immediately prior to their release (71%) than communities in the control group (77%; see graph below). Specifically, 48% of communities in the intervention group initiated buprenorphine, 32% initiated methadone, and 58% initiated naltrexone. In the control group, 63% initiated buprenorphine, 37% initiated methadone, and 63% initiated naltrexone. However, there was no impact of the intervention on whether communities had jails that started people on medication treatment. Across medication types, there was also no impact of the intervention on whether communities had jails that initiated buprenorphine and naltrexone, but this analysis could not be run for methadone because 2 of the 4 research sites did not initiate anyone on methadone (i.e., had zero prevalence).
More communities in the intervention group had jails that linked people with opioid use disorder to medication treatment following their release (90%) than communities in the control group (73%; see graph below). However, this just missed statistical significance (p = .058).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the impact of an intervention designed to support communities in implementing evidence-based practices to reduce opioid overdoses. Specifically, the researchers investigated whether the intervention had an impact on communities with jails: (1) that started people with opioid use disorder on medication treatment during their incarceration and immediately prior to their release and (2) linked people to medication for opioid use disorder treatment upon their release.
Results showed that, at baseline, the majority of communities’ jails in both the control and intervention groups provided medication treatment for opioid use disorder and linkage to medication treatment upon release, with slightly more communities’ jails from the control group. The number of jails in intervention communities that provided linkage to medication treatment upon release may have increased more than control communities during the evaluation period, but this just missed statistical significance.
The inability of the researchers to detect an effect of the intervention may be partially due to the intervention not being specifically designed to increase medication treatment and linkage in criminal justice settings. Rather, the intervention was designed to support community coalition leaders in implementing evidence-based practices of their choice, of which medication treatment and linkage in jails was one option. Another possible explanation is that the evaluation period occurred amidst rapidly changing policies and contexts that may have made it more difficult to attribute any increases in medication provision and linkage to the intervention itself. For example, Massachusetts mandated the availability of all 3 medications for opioid use disorder in state prisons and 7 county correctional facilities in the same year that implementation of the intervention began.
Despite the lack of an intervention effect, the finding that, at the beginning of the study, many of the communities in both the intervention and control groups were already offering medication treatment for opioid use disorder in jails and linkage to medication services upon release is promising and reflects the changing views and perspectives of medication treatment.
Also, even with the harder-to-implement agonist medications methadone and buprenorphine, substantial increases were reported across both intervention and control communities. Still, several barriers remain to achieve maximum implementation of medication treatment for opioid use disorder in criminal justice settings (e.g., costs, stigma, need for dosing protocols and training, diversion concerns). The (statistically non-significant but) sizeable increase in the number of intervention communities offering linkage to medication following release from jail, however, suggests that community coalitions may be critical in addressing these barriers and increasing medication treatment and linkage.
The study was conducted in 4 states in the United States. Results may therefore not be reflective of all states in the US or generalize to other countries.
Data collected from the survey was self-reported and therefore could be subject to desirability bias – i.e., participants may have over-reported service provision at later time points because they think that is what the researchers want.
Because the data was self-reported, it is also reliant on jail administrators’ knowledge of medication and linkage provision, which may or may not be accurate.
The small sample size of the study (i.e., jails from 67 communities) may have limited the researchers’ ability to detect smaller effects from intervention, which may in part explain why they did not find an effect of the intervention.
One of the states in the study, Massachusetts, had jails from communities that were part of both the control and intervention groups. Similarly, communities in other states that were assigned to the control and intervention groups were next to each other. Given the central role of state laws and policies on jail-based healthcare services, both of these could have reduced any differences between the intervention and control communities.
BOTTOM LINE
The majority of jails in communities that were part of the HEALing Communities Study reported that they offered at least 1 type of medication to treat opioid use disorder during incarceration and that they offered linkage to medication treatment upon release at the beginning of the study. While there was no impact of the intervention on offering medications to individuals during incarceration, the number of jails from communities receiving the intervention that offered linkage to medication treatment increased during the evaluation period.
For individuals and families seeking recovery: The study’s findings suggest that access to medication treatment for opioid use disorder during incarceration and linkage to medication services upon release is becoming more common, reflecting a growing recognition that such treatments save lives. While availability may vary by location, continuity of medication during and after incarceration can reduce overdose risk during a particularly vulnerable transition period. For individuals and families, this highlights the importance of asking about medication options and linkage to care when navigating release planning and re-entry into the community.
For treatment professionals and treatment systems: Although the intervention did not produce statistically significant increases in offering medication during incarceration, the widespread baseline availability of medication treatment in jails with increases across both intervention and control communities points to meaningful progress and is encouraging. The modest increase in linkage upon release observed in intervention communities suggests that community coalitions may play an important role in addressing persistent barriers such as stigma, logistical challenges, and continuity of care, and can make a difference. Treatment systems may benefit from strengthening partnerships between jails, community providers, and re-entry services to ensure timely and sustained access to medication following release.
For scientists: Given the study’s limited geographic scope, reliance on self-reported data, and relatively small sample size, future research that uses larger samples, objective measures of service provision, and longer follow-up periods can help clarify the impact of community-based interventions on the provision of medication treatment for opioid use disorder in criminal justice settings. Studies designed to isolate criminal justice-specific strategies, account for policy changes occurring concurrently with interventions, and examine how coalitions overcome logistical and structural barriers can deepen understanding of what drives successful medication initiation and linkage. Such work can help distinguish intervention effects from broader policy and system-level shifts.
For policy makers: The study’s findings indicate that many jurisdictions are already moving toward offering medication treatment in jails and linkage upon release, reflecting changing norms and policy environments. While the evaluated intervention did not independently drive widespread change, the results point to the potential value of policies that support cross-sector coordination, resource allocation, and technical assistance for implementation. Policymakers who build on existing momentum by supporting policies that address structural barriers, such as funding, training, and continuity of care, can further expand medication treatment for opioid use disorder in criminal justice settings and linkage to medication services upon release.
The Communities that Heal intervention was designed to reduce overdose deaths by supporting communities in implementing evidence-based practices of their choice, including, but not limited to, medication treatment for opioid use disorder in criminal justice settings. This intervention was evaluated by the HEALing (Helping to End Addiction Long-term) Communities Study, which randomized communities to either receive the intervention or to be waitlisted as part of the control group. Communities that were randomized to the intervention group received the intervention from January 2020 to June 2022.
This study focused on whether communities randomized to the intervention group had more jails that expanded the provision of medications for opioid use disorder than communities in the control group. They were also interested in whether the intervention communities had more jails that linked people to medication treatment upon being released from jail. Such research can shed light on whether interventions designed to support communities in implementing evidence-based practices for reducing overdose deaths, such as the Communities that Heal intervention, expands access to medication treatment for opioid use disorder in criminal justice settings and increases linkage to medication services following release.
HOW WAS THIS STUDY CONDUCTED?
This study examined whether communities assigned to the intervention group, as part of the Communities that Heal study, had more jails that provided medications for opioid use disorder in jails and linked people to medication treatment upon release more than the communities’ jails assigned to the control group. These outcomes were assessed with a survey administered in jails within the 67 communities that were part of the study.
This survey was administered at 3 time points. For the first time point, data was collected as part of the Justice Community Opioid Innovation Network (JCOIN) and the HEALing Communities Study, which administered the survey to jail administrators in 2018 and 2019. Survey questions assessed the availability, accessibility, and use of interventions to treat opioid use disorder in jails during the prior 12 months. For the second and third time points, data was collected as part of the HEALing Communities Study. Data for the second survey was collected between 7/1/2020 and 6/30/2021, while data for the third survey was collected between 7/1/2021 and 6/30/2022. However, this study only used data from the first and third time points in their analyses.
The 2 primary outcomes of interest included the impact of the intervention on whether communities had jails: (1) that started people with opioid use disorder on medication treatment during their incarceration and/or immediately prior to their release, and (2) linked people to medication for opioid use disorder treatment upon their release. The researchers categorized jails as providing medications for opioid use disorder if jail administrators answered yes to 1 of the 2 following questions: “Is (buprenorphine, methadone, or naltrexone) used for induction and treatment during incarceration?” or “Is (buprenorphine, methadone, or naltrexone) used for pre-release induction?” The researchers also categorized jails as linking people to medication treatment upon release if the jail administrators reported that their jail provides 1 or more re-entry or continuity of care services, such as scheduling appointments with medication providers in the community or helping with completing intake paperwork for medication treatment. The researchers were also interested in the type of medication for opioid use disorders that the jails offered as a secondary outcome (buprenorphine, methadone, or naltrexone).
Analyses included descriptive statistics to summarize the frequencies, percentages, and means of jail characteristics and primary outcomes. Then models tested the impact of the intervention on each outcome at the third time point (i.e., the evaluation period, which was between 7/1/2021 and 6/30/2022). Only communities that responded to the first and third surveys were included in the analyses.
The 67 communities that participated in the HEALing Communities Study included 16 research sites across Kentucky, Massachusetts, and New York, each, and 19 research sites in Ohio. Of these, 57% of the communities were urban and 43% were rural.
There were 8.2 million adults estimated to populate the 67 communities. Of these, 31% were between the ages of 18-34, 31% were between 35-54, and 39% were 55 years old or older. The majority identified as non-Hispanic White (73%). For the remaining races/ethnicities, 16% identified as non-Hispanic Black, 4% identified as non-Hispanic Other, and 7% identified as Hispanic. People in the communities were approximately half men (48%) and half women (52%). The 67 communities in the study were randomized to either the intervention group (34 communities) or to the control condition that were waitlisted to receive the intervention (33 communities).
Of the 67 communities, administrators from 54 jails returned the baseline survey, with 27 from the intervention group and 27 from the control group (see graphic below for a summary of the study procedures). It is unclear from the study how many jails were offered the baseline survey but did not take it because the response rate was not reported in the study. It is possible that jails which did not respond were less likely to provide, or link to, opioid use disorder medication at baseline and may not have been open to changes in their medication policies. If that was the case, and these types of jails were more likely to be in the intervention versus control group, study effects may be overestimated. If these types of nonresponders were more likely to be in the control group, study effects may be underestimated. Jails that did return the survey included 15 sites from Kentucky, 11 from Massachusetts, 12 from New York, and 16 from Ohio. Among these, the jails had an average of approximately 8,600 detainees, of which approximately 3,540 had an opioid use disorder. The majority of these jails served both males and females (87%), had a screening protocol in place to identify people who may have opioid use disorder (89%), and had a standardized protocol in place to identify people experiencing opioid withdrawal (98%).
The most commonly reported methods for identifying people with an opioid use disorder were the self-reported number of days using opioids (96%) and use of a screening tool for substance use disorders (81%; primarily an agency-created screening tool with 77% of jails reporting use of this type of screening tool). The most commonly reported tool for identifying people experiencing opioid withdrawal were self-report (100%) and clinical observation (92%).
WHAT DID THIS STUDY FIND?
At baseline, slightly more control communities’ jails started people on medication for opioid use disorder and linked them to medication treatment upon release
At the baseline survey, there were slight differences in the percentages of communities with jails that started people with opioid use disorder on medication treatment and linked them to medication treatment upon release. More communities in the waitlisted control group had jails that started people on medication treatment during incarceration or immediately prior to release (76%) compared to communities in the intervention group (63%).
Specifically, more communities in the waitlisted control group had jails that started people on buprenorphine, methadone, and naltrexone during incarceration or immediately prior to release, with percentages of 24%, 7%, and 76%, respectively. This is compared to 10%, 0%, and 63% of intervention communities having jails who initiated these medications, respectively.
Likewise, more communities in the waitlisted control group had jails that linked people to medication treatment upon release (79%) compared to communities in the intervention group (67%). The most commonly reported linkage services provided by the jails were scheduling appointments with providers in the community (61%), facilitating the exchange of information with a medication provider in the community (60%), and helping to complete intake paperwork (59%).
There was no impact of the intervention on outcomes
At the third time point (during the evaluation period), fewer communities in the intervention group had jails that started people on medication for opioid use disorder during their incarceration or immediately prior to their release (71%) than communities in the control group (77%; see graph below). Specifically, 48% of communities in the intervention group initiated buprenorphine, 32% initiated methadone, and 58% initiated naltrexone. In the control group, 63% initiated buprenorphine, 37% initiated methadone, and 63% initiated naltrexone. However, there was no impact of the intervention on whether communities had jails that started people on medication treatment. Across medication types, there was also no impact of the intervention on whether communities had jails that initiated buprenorphine and naltrexone, but this analysis could not be run for methadone because 2 of the 4 research sites did not initiate anyone on methadone (i.e., had zero prevalence).
More communities in the intervention group had jails that linked people with opioid use disorder to medication treatment following their release (90%) than communities in the control group (73%; see graph below). However, this just missed statistical significance (p = .058).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the impact of an intervention designed to support communities in implementing evidence-based practices to reduce opioid overdoses. Specifically, the researchers investigated whether the intervention had an impact on communities with jails: (1) that started people with opioid use disorder on medication treatment during their incarceration and immediately prior to their release and (2) linked people to medication for opioid use disorder treatment upon their release.
Results showed that, at baseline, the majority of communities’ jails in both the control and intervention groups provided medication treatment for opioid use disorder and linkage to medication treatment upon release, with slightly more communities’ jails from the control group. The number of jails in intervention communities that provided linkage to medication treatment upon release may have increased more than control communities during the evaluation period, but this just missed statistical significance.
The inability of the researchers to detect an effect of the intervention may be partially due to the intervention not being specifically designed to increase medication treatment and linkage in criminal justice settings. Rather, the intervention was designed to support community coalition leaders in implementing evidence-based practices of their choice, of which medication treatment and linkage in jails was one option. Another possible explanation is that the evaluation period occurred amidst rapidly changing policies and contexts that may have made it more difficult to attribute any increases in medication provision and linkage to the intervention itself. For example, Massachusetts mandated the availability of all 3 medications for opioid use disorder in state prisons and 7 county correctional facilities in the same year that implementation of the intervention began.
Despite the lack of an intervention effect, the finding that, at the beginning of the study, many of the communities in both the intervention and control groups were already offering medication treatment for opioid use disorder in jails and linkage to medication services upon release is promising and reflects the changing views and perspectives of medication treatment.
Also, even with the harder-to-implement agonist medications methadone and buprenorphine, substantial increases were reported across both intervention and control communities. Still, several barriers remain to achieve maximum implementation of medication treatment for opioid use disorder in criminal justice settings (e.g., costs, stigma, need for dosing protocols and training, diversion concerns). The (statistically non-significant but) sizeable increase in the number of intervention communities offering linkage to medication following release from jail, however, suggests that community coalitions may be critical in addressing these barriers and increasing medication treatment and linkage.
The study was conducted in 4 states in the United States. Results may therefore not be reflective of all states in the US or generalize to other countries.
Data collected from the survey was self-reported and therefore could be subject to desirability bias – i.e., participants may have over-reported service provision at later time points because they think that is what the researchers want.
Because the data was self-reported, it is also reliant on jail administrators’ knowledge of medication and linkage provision, which may or may not be accurate.
The small sample size of the study (i.e., jails from 67 communities) may have limited the researchers’ ability to detect smaller effects from intervention, which may in part explain why they did not find an effect of the intervention.
One of the states in the study, Massachusetts, had jails from communities that were part of both the control and intervention groups. Similarly, communities in other states that were assigned to the control and intervention groups were next to each other. Given the central role of state laws and policies on jail-based healthcare services, both of these could have reduced any differences between the intervention and control communities.
BOTTOM LINE
The majority of jails in communities that were part of the HEALing Communities Study reported that they offered at least 1 type of medication to treat opioid use disorder during incarceration and that they offered linkage to medication treatment upon release at the beginning of the study. While there was no impact of the intervention on offering medications to individuals during incarceration, the number of jails from communities receiving the intervention that offered linkage to medication treatment increased during the evaluation period.
For individuals and families seeking recovery: The study’s findings suggest that access to medication treatment for opioid use disorder during incarceration and linkage to medication services upon release is becoming more common, reflecting a growing recognition that such treatments save lives. While availability may vary by location, continuity of medication during and after incarceration can reduce overdose risk during a particularly vulnerable transition period. For individuals and families, this highlights the importance of asking about medication options and linkage to care when navigating release planning and re-entry into the community.
For treatment professionals and treatment systems: Although the intervention did not produce statistically significant increases in offering medication during incarceration, the widespread baseline availability of medication treatment in jails with increases across both intervention and control communities points to meaningful progress and is encouraging. The modest increase in linkage upon release observed in intervention communities suggests that community coalitions may play an important role in addressing persistent barriers such as stigma, logistical challenges, and continuity of care, and can make a difference. Treatment systems may benefit from strengthening partnerships between jails, community providers, and re-entry services to ensure timely and sustained access to medication following release.
For scientists: Given the study’s limited geographic scope, reliance on self-reported data, and relatively small sample size, future research that uses larger samples, objective measures of service provision, and longer follow-up periods can help clarify the impact of community-based interventions on the provision of medication treatment for opioid use disorder in criminal justice settings. Studies designed to isolate criminal justice-specific strategies, account for policy changes occurring concurrently with interventions, and examine how coalitions overcome logistical and structural barriers can deepen understanding of what drives successful medication initiation and linkage. Such work can help distinguish intervention effects from broader policy and system-level shifts.
For policy makers: The study’s findings indicate that many jurisdictions are already moving toward offering medication treatment in jails and linkage upon release, reflecting changing norms and policy environments. While the evaluated intervention did not independently drive widespread change, the results point to the potential value of policies that support cross-sector coordination, resource allocation, and technical assistance for implementation. Policymakers who build on existing momentum by supporting policies that address structural barriers, such as funding, training, and continuity of care, can further expand medication treatment for opioid use disorder in criminal justice settings and linkage to medication services upon release.
The Communities that Heal intervention was designed to reduce overdose deaths by supporting communities in implementing evidence-based practices of their choice, including, but not limited to, medication treatment for opioid use disorder in criminal justice settings. This intervention was evaluated by the HEALing (Helping to End Addiction Long-term) Communities Study, which randomized communities to either receive the intervention or to be waitlisted as part of the control group. Communities that were randomized to the intervention group received the intervention from January 2020 to June 2022.
This study focused on whether communities randomized to the intervention group had more jails that expanded the provision of medications for opioid use disorder than communities in the control group. They were also interested in whether the intervention communities had more jails that linked people to medication treatment upon being released from jail. Such research can shed light on whether interventions designed to support communities in implementing evidence-based practices for reducing overdose deaths, such as the Communities that Heal intervention, expands access to medication treatment for opioid use disorder in criminal justice settings and increases linkage to medication services following release.
HOW WAS THIS STUDY CONDUCTED?
This study examined whether communities assigned to the intervention group, as part of the Communities that Heal study, had more jails that provided medications for opioid use disorder in jails and linked people to medication treatment upon release more than the communities’ jails assigned to the control group. These outcomes were assessed with a survey administered in jails within the 67 communities that were part of the study.
This survey was administered at 3 time points. For the first time point, data was collected as part of the Justice Community Opioid Innovation Network (JCOIN) and the HEALing Communities Study, which administered the survey to jail administrators in 2018 and 2019. Survey questions assessed the availability, accessibility, and use of interventions to treat opioid use disorder in jails during the prior 12 months. For the second and third time points, data was collected as part of the HEALing Communities Study. Data for the second survey was collected between 7/1/2020 and 6/30/2021, while data for the third survey was collected between 7/1/2021 and 6/30/2022. However, this study only used data from the first and third time points in their analyses.
The 2 primary outcomes of interest included the impact of the intervention on whether communities had jails: (1) that started people with opioid use disorder on medication treatment during their incarceration and/or immediately prior to their release, and (2) linked people to medication for opioid use disorder treatment upon their release. The researchers categorized jails as providing medications for opioid use disorder if jail administrators answered yes to 1 of the 2 following questions: “Is (buprenorphine, methadone, or naltrexone) used for induction and treatment during incarceration?” or “Is (buprenorphine, methadone, or naltrexone) used for pre-release induction?” The researchers also categorized jails as linking people to medication treatment upon release if the jail administrators reported that their jail provides 1 or more re-entry or continuity of care services, such as scheduling appointments with medication providers in the community or helping with completing intake paperwork for medication treatment. The researchers were also interested in the type of medication for opioid use disorders that the jails offered as a secondary outcome (buprenorphine, methadone, or naltrexone).
Analyses included descriptive statistics to summarize the frequencies, percentages, and means of jail characteristics and primary outcomes. Then models tested the impact of the intervention on each outcome at the third time point (i.e., the evaluation period, which was between 7/1/2021 and 6/30/2022). Only communities that responded to the first and third surveys were included in the analyses.
The 67 communities that participated in the HEALing Communities Study included 16 research sites across Kentucky, Massachusetts, and New York, each, and 19 research sites in Ohio. Of these, 57% of the communities were urban and 43% were rural.
There were 8.2 million adults estimated to populate the 67 communities. Of these, 31% were between the ages of 18-34, 31% were between 35-54, and 39% were 55 years old or older. The majority identified as non-Hispanic White (73%). For the remaining races/ethnicities, 16% identified as non-Hispanic Black, 4% identified as non-Hispanic Other, and 7% identified as Hispanic. People in the communities were approximately half men (48%) and half women (52%). The 67 communities in the study were randomized to either the intervention group (34 communities) or to the control condition that were waitlisted to receive the intervention (33 communities).
Of the 67 communities, administrators from 54 jails returned the baseline survey, with 27 from the intervention group and 27 from the control group (see graphic below for a summary of the study procedures). It is unclear from the study how many jails were offered the baseline survey but did not take it because the response rate was not reported in the study. It is possible that jails which did not respond were less likely to provide, or link to, opioid use disorder medication at baseline and may not have been open to changes in their medication policies. If that was the case, and these types of jails were more likely to be in the intervention versus control group, study effects may be overestimated. If these types of nonresponders were more likely to be in the control group, study effects may be underestimated. Jails that did return the survey included 15 sites from Kentucky, 11 from Massachusetts, 12 from New York, and 16 from Ohio. Among these, the jails had an average of approximately 8,600 detainees, of which approximately 3,540 had an opioid use disorder. The majority of these jails served both males and females (87%), had a screening protocol in place to identify people who may have opioid use disorder (89%), and had a standardized protocol in place to identify people experiencing opioid withdrawal (98%).
The most commonly reported methods for identifying people with an opioid use disorder were the self-reported number of days using opioids (96%) and use of a screening tool for substance use disorders (81%; primarily an agency-created screening tool with 77% of jails reporting use of this type of screening tool). The most commonly reported tool for identifying people experiencing opioid withdrawal were self-report (100%) and clinical observation (92%).
WHAT DID THIS STUDY FIND?
At baseline, slightly more control communities’ jails started people on medication for opioid use disorder and linked them to medication treatment upon release
At the baseline survey, there were slight differences in the percentages of communities with jails that started people with opioid use disorder on medication treatment and linked them to medication treatment upon release. More communities in the waitlisted control group had jails that started people on medication treatment during incarceration or immediately prior to release (76%) compared to communities in the intervention group (63%).
Specifically, more communities in the waitlisted control group had jails that started people on buprenorphine, methadone, and naltrexone during incarceration or immediately prior to release, with percentages of 24%, 7%, and 76%, respectively. This is compared to 10%, 0%, and 63% of intervention communities having jails who initiated these medications, respectively.
Likewise, more communities in the waitlisted control group had jails that linked people to medication treatment upon release (79%) compared to communities in the intervention group (67%). The most commonly reported linkage services provided by the jails were scheduling appointments with providers in the community (61%), facilitating the exchange of information with a medication provider in the community (60%), and helping to complete intake paperwork (59%).
There was no impact of the intervention on outcomes
At the third time point (during the evaluation period), fewer communities in the intervention group had jails that started people on medication for opioid use disorder during their incarceration or immediately prior to their release (71%) than communities in the control group (77%; see graph below). Specifically, 48% of communities in the intervention group initiated buprenorphine, 32% initiated methadone, and 58% initiated naltrexone. In the control group, 63% initiated buprenorphine, 37% initiated methadone, and 63% initiated naltrexone. However, there was no impact of the intervention on whether communities had jails that started people on medication treatment. Across medication types, there was also no impact of the intervention on whether communities had jails that initiated buprenorphine and naltrexone, but this analysis could not be run for methadone because 2 of the 4 research sites did not initiate anyone on methadone (i.e., had zero prevalence).
More communities in the intervention group had jails that linked people with opioid use disorder to medication treatment following their release (90%) than communities in the control group (73%; see graph below). However, this just missed statistical significance (p = .058).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the impact of an intervention designed to support communities in implementing evidence-based practices to reduce opioid overdoses. Specifically, the researchers investigated whether the intervention had an impact on communities with jails: (1) that started people with opioid use disorder on medication treatment during their incarceration and immediately prior to their release and (2) linked people to medication for opioid use disorder treatment upon their release.
Results showed that, at baseline, the majority of communities’ jails in both the control and intervention groups provided medication treatment for opioid use disorder and linkage to medication treatment upon release, with slightly more communities’ jails from the control group. The number of jails in intervention communities that provided linkage to medication treatment upon release may have increased more than control communities during the evaluation period, but this just missed statistical significance.
The inability of the researchers to detect an effect of the intervention may be partially due to the intervention not being specifically designed to increase medication treatment and linkage in criminal justice settings. Rather, the intervention was designed to support community coalition leaders in implementing evidence-based practices of their choice, of which medication treatment and linkage in jails was one option. Another possible explanation is that the evaluation period occurred amidst rapidly changing policies and contexts that may have made it more difficult to attribute any increases in medication provision and linkage to the intervention itself. For example, Massachusetts mandated the availability of all 3 medications for opioid use disorder in state prisons and 7 county correctional facilities in the same year that implementation of the intervention began.
Despite the lack of an intervention effect, the finding that, at the beginning of the study, many of the communities in both the intervention and control groups were already offering medication treatment for opioid use disorder in jails and linkage to medication services upon release is promising and reflects the changing views and perspectives of medication treatment.
Also, even with the harder-to-implement agonist medications methadone and buprenorphine, substantial increases were reported across both intervention and control communities. Still, several barriers remain to achieve maximum implementation of medication treatment for opioid use disorder in criminal justice settings (e.g., costs, stigma, need for dosing protocols and training, diversion concerns). The (statistically non-significant but) sizeable increase in the number of intervention communities offering linkage to medication following release from jail, however, suggests that community coalitions may be critical in addressing these barriers and increasing medication treatment and linkage.
The study was conducted in 4 states in the United States. Results may therefore not be reflective of all states in the US or generalize to other countries.
Data collected from the survey was self-reported and therefore could be subject to desirability bias – i.e., participants may have over-reported service provision at later time points because they think that is what the researchers want.
Because the data was self-reported, it is also reliant on jail administrators’ knowledge of medication and linkage provision, which may or may not be accurate.
The small sample size of the study (i.e., jails from 67 communities) may have limited the researchers’ ability to detect smaller effects from intervention, which may in part explain why they did not find an effect of the intervention.
One of the states in the study, Massachusetts, had jails from communities that were part of both the control and intervention groups. Similarly, communities in other states that were assigned to the control and intervention groups were next to each other. Given the central role of state laws and policies on jail-based healthcare services, both of these could have reduced any differences between the intervention and control communities.
BOTTOM LINE
The majority of jails in communities that were part of the HEALing Communities Study reported that they offered at least 1 type of medication to treat opioid use disorder during incarceration and that they offered linkage to medication treatment upon release at the beginning of the study. While there was no impact of the intervention on offering medications to individuals during incarceration, the number of jails from communities receiving the intervention that offered linkage to medication treatment increased during the evaluation period.
For individuals and families seeking recovery: The study’s findings suggest that access to medication treatment for opioid use disorder during incarceration and linkage to medication services upon release is becoming more common, reflecting a growing recognition that such treatments save lives. While availability may vary by location, continuity of medication during and after incarceration can reduce overdose risk during a particularly vulnerable transition period. For individuals and families, this highlights the importance of asking about medication options and linkage to care when navigating release planning and re-entry into the community.
For treatment professionals and treatment systems: Although the intervention did not produce statistically significant increases in offering medication during incarceration, the widespread baseline availability of medication treatment in jails with increases across both intervention and control communities points to meaningful progress and is encouraging. The modest increase in linkage upon release observed in intervention communities suggests that community coalitions may play an important role in addressing persistent barriers such as stigma, logistical challenges, and continuity of care, and can make a difference. Treatment systems may benefit from strengthening partnerships between jails, community providers, and re-entry services to ensure timely and sustained access to medication following release.
For scientists: Given the study’s limited geographic scope, reliance on self-reported data, and relatively small sample size, future research that uses larger samples, objective measures of service provision, and longer follow-up periods can help clarify the impact of community-based interventions on the provision of medication treatment for opioid use disorder in criminal justice settings. Studies designed to isolate criminal justice-specific strategies, account for policy changes occurring concurrently with interventions, and examine how coalitions overcome logistical and structural barriers can deepen understanding of what drives successful medication initiation and linkage. Such work can help distinguish intervention effects from broader policy and system-level shifts.
For policy makers: The study’s findings indicate that many jurisdictions are already moving toward offering medication treatment in jails and linkage upon release, reflecting changing norms and policy environments. While the evaluated intervention did not independently drive widespread change, the results point to the potential value of policies that support cross-sector coordination, resource allocation, and technical assistance for implementation. Policymakers who build on existing momentum by supporting policies that address structural barriers, such as funding, training, and continuity of care, can further expand medication treatment for opioid use disorder in criminal justice settings and linkage to medication services upon release.