Less is more? Additions to a brief intervention for youth alcohol use and aggression
Alcohol use and aggression in young people can lead to severe consequences, including emergency room visits. This study recruited young people presenting in emergency departments and tested whether additional treatments can improve on an established brief intervention for alcohol use and aggression.
Underage alcohol use is linked to disruptions in typical neurological development, a higher risk of developing alcohol use disorder later in life, and acute harms such as injuries, sexual assault, overdose, motor vehicle accidents, and death. Alcohol is also considered to be the most harmful substance to other people (e.g., assaults, domestic violence). In parallel, youth aggression also contributes significantly to public health concerns. For youth ages 15-19, homicide was the second leading cause of death in 2021. Thus, interventions for youth that lead to reduced alcohol use and aggression may have a meaningful individual and societal impacts.
A range of interventions have been shown to help reduce alcohol use among youth though many do not willingly attend treatment. Furthermore, typical programs taking several sessions can be costly and may not be feasible for many young people. Brief interventions—often delivered in a single session—are promising strategies that save resources, scale easily, and may improve outcomes. Incorporating technology and adaptive design elements may further enhance the effectiveness of these brief approaches without substantially increasing costs. For example, strategically allocating resources to individuals with the greatest need (i.e., adapting), assessed at multiple timepoints, may improve efficiency and support broader scalability. This study explored if adaptative boosters following a brief intervention for young people reporting to the emergency department had a differential effect on alcohol use and aggression.
HOW WAS THIS STUDY CONDUCTED?
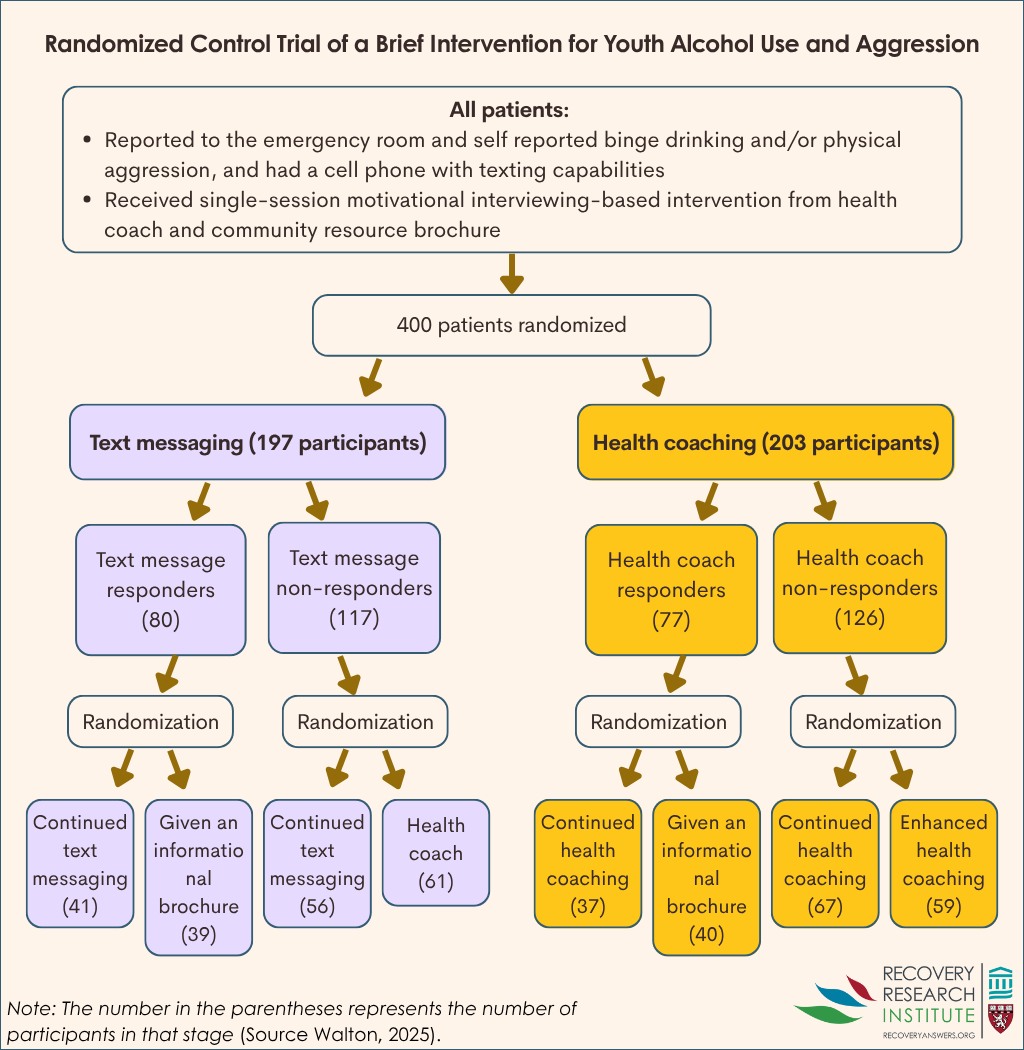
This study was a sequential multiple assignment randomized trial among 400 youth (aged 14-20) that reported to the emergency department for any reason except sexual assault, child maltreatment, or suicide attempt/ideation. Youth who self-reported binge drinking (via the AUDIT-C assessment), physical aggression, and a cell phone with texting capabilities were eligible for the study. Following the initial baseline survey and enrollment, youth received a brief intervention followed by an 8-week sequential multiple assignment randomized trial (see graphic below for details). Then outcomes were measured at 4- and 8-months post brief intervention.
In this study, the sequential design featured two 4-week stages with weekly surveys and two primary booster conditions. The main aim of this study was to explore if changing the booster condition after 4-weeks impacted the intervention outcomes, which could suggest the efficiency of adapting resource allocation (e.g., more and less) at multiple timepoints to improve outcomes for youth.
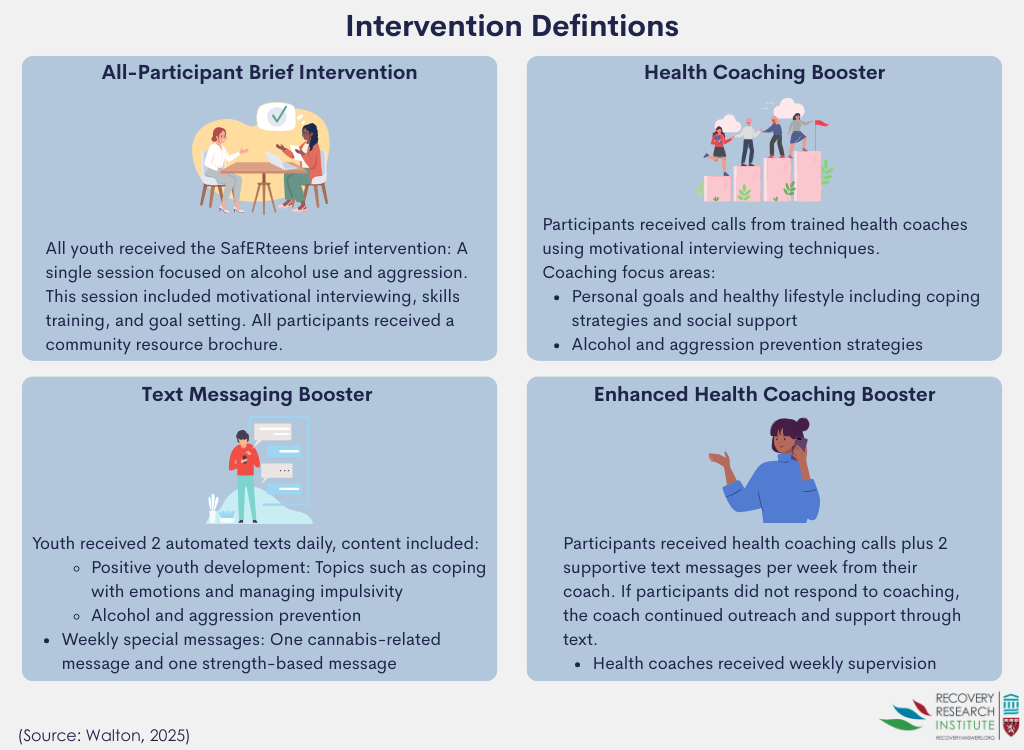
All youth received the SafERteens single session brief intervention for alcohol use and aggression, which combines motivational interviewing and skills training. The brief intervention (averaging 32 minutes in this study) includes goal setting, tailored feedback, decisional balance exercise, role plays, and referrals. See graphic below for intervention details.
After the brief intervention, the participants received boosters: text messaging, telehealth calls from a health coach, both texts and telehealth calls, or a resource brochure. For the text messaging booster, youth received automated texts twice per day. The automated texts were pulled from a library of about 1200 possible texts that were created with feedback from youth advisors. Morning texts (10am-3pm) featured positive youth development messages related to coping with negative feelings, impulsivity, excitement, social support, hope, and leisure activities. Afternoon texts (4-9pm) featured reasons and tools to avoid or reduce alcohol use and aggression. One day per week included a cannabis-related message, and one day included a strength or positive quality that the youth participant had identified themselves in the prior weekly survey. The health coaching condition included calls from a trained health coach and featured motivational interviewing focused on personal goals and healthy lifestyles with strategies to avoid alcohol and aggression incorporated when possible.
The graphic below outlines how participants flowed through this multi-stage study. At the first stage, youth were randomly assigned to either receive the text messaging or health coach call. After the first 4-weeks, youth were identified as intervention responders or non-responders. Response status was determined by self-reports on the week 3 and 4 surveys. “Responders” were those who reported no binge drinking or aggression, and “non-responders” were those who reported binge drinking, aggression, both, or did not complete the survey.
At the second stage, responders were randomized to receive either the same condition (i.e., booster) or a minimized condition (health coach to texts or texts to resource brochure). Non-responders were re-randomized to receive either the same or an intensive condition (e.g., text messaging stepped up to health coach; health coach stepped up to health coach plus text messages). This 2-stage process results in 8 possible groups.
The first analysis compared texts versus heath coaching after the first 4-week stage on 4- and 8-month outcomes. The next group of analyses assessed responders and non-responders separately on 8-month outcomes accounting for the 4-month outcomes, age, and sex. The last group of analyses looked at overall changes from baseline to 8-month follow-up. The two primary outcomes were past 30-day alcohol use and past 30-day aggression, which could be toward friends, neighbors, relatives, acquaintances, dating partners, or strangers. Aggression was then made into a yes/no variable because it was so rarely reported. Secondary alcohol outcomes included alcohol misuse (yes/no), alcohol consequences, and violence-related consequences. Additional outcomes explored other drug-related measures including drug use severity and drug-related consequences.
There were 400 youth aged 14-20 years (average 18) enrolled in the study. Most of the youthwere female (78%), with 51% identifying as Black or African American, 40% White, and less than 10% as another race. Just over half (55%) received public assistance, and 99% were never married. At baseline, the average total number of drinks in the past 30 days was 29, and 52% met AUDIT-C cutoffs for harmful drinking (e.g., score of 3+ in adolescent females). Youth reported 7 alcohol-related consequences, on average. The average days of aggression was less than 1, and the average number of aggression-related consequences was 3. Most youth reported cannabis use (81%), although youth also reported “other illicit drug use” (23%), prescription opioid misuse (15%), prescription sedative misuse (17%), and prescription stimulant misuse (10%).
WHAT DID THIS STUDY FIND?
Booster strategies were equally effective
Outcomes were assessed related to both the first and second stage of randomization. There were no differences in the impact of the text messaging versus the health coaching on reducing alcohol consumption or aggression at the first stage. There were also no differences in alcohol misuse, alcohol-related consequences, aggression-related consequences, other drug use, or other drug-related consequences. Furthermore, the second stage booster strategies for responders and non-responders did not change the effects. For example, for those receiving text messages, adding health coaching did no better than continued text messages. Similarly, there were no differences across all outcomes.
Youth improved over time after receiving the intervention, however
Across all conditions, youth were 4 times as likely to report alcohol abstinence at 4 and 8 months compared to baseline. Among those that did report alcohol use, there was no improvement between baseline alcohol use frequency and the 4- or 8-month follow ups. Youth were nearly 10 times and 15 times more likely to have no alcohol-related consequences at the 4- and 8-month follow up, respectively.
Aggression was less likely at the 8-month follow up, but not the 4-month, compared to baseline. Specifically, participants were about half as likely to report aggression 8 months after the brief intervention. Other drug use apart from alcohol, other drug-related consequences, and aggression-related consequences were also less likely at the 4- and 8-month follow ups compared to baseline.
While these improvements are noteworthy, all individuals in the study received the brief intervention and there was no real non-treatment condition (although the type and intensity of texting and health coaching did vary across time). Consequently, we can’t know with certainty whether such improvements would have happened anyway without this intervention.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study did not find that adding either daily text messages or adding calls from a health coach improved outcomes when added to a brief intervention delivered in the emergency department. Furthermore, among those who did not have a positive response, outcomes were similar for more (e.g., texting to health coach calls) and less intense (e.g., texting to resource brochure) boosters. Overall, boosters did not differentially change the impact of the intervention on alcohol, aggression, or other drug outcomes. This could be good news: automated text messages were as effective as a live health coach phone call. That said, the study did not include a comparison group that received no booster, so it remains unclear whether boosters themselves led to improved outcomes.
More research is needed to disentangle the effects of the brief intervention and booster sessions, so that this empirically-supported approach to address youth alcohol use and aggression can be scaled in as cost-efficient manner as possible. It may be that certain youth may prefer or respond better to different types of approaches, but this was not examined in this study.
Of note there may have been a selection bias in the included study sample as most youth ED visits for alcohol/drug related aggression are male and almost four out of five study participants here were female. Though it is unclear why females were overrepresented, this unusual aspect of the study suggests results may have been different with more males represented and included in the study.
The majority of youth were female, and there were very few cases of aggression. These further limit the generalizability for the brief intervention and boosters’ impact on alcohol use and aggression across genders.
Public events (Flint Water Crisis, COVID-19, and recreational cannabis legalization) may have meaningfully impacted the behaviors that led to inclusions in the study (e.g., alcohol use) as well as changes over time. The variety of public health events that occurred during recruitment also limit the ability to generalize to youth in other locations or over time.
The study did not include a control that did not receive the brief intervention or a group that did not receive any boosters. The absence of control groups prevents us from knowing if the brief intervention impacted changes in outcomes or if receiving any booster altered outcomes.
BOTTOM LINE
Alcohol and aggression interventions for youth can be costly and time-consuming. Brief, single-session interventions paired with adaptive boosters—tailored based on recent behavior—have the potential to enhance effectiveness and efficiency, thereby improving scalability. In the current study, the adaptive boosters – automated text messaging and a health coach phone call – did equally as well. Given the ongoing need for effective and scalable approaches, continued rigorous research is essential to guide the development of future interventions and booster strategies for co-occurring youth alcohol use and aggression.
For individuals and families seeking recovery: This study did not find that one intervention booster strategy was better or worse than others in impacting alcohol or aggression outcomes. However, the nearly all-female sample of youth showed improvements in alcohol and aggression. It may be that receiving any intervention booster after the brief intervention positively impacted results for young women. If you or a loved one are engaging in an intervention, participating in actives meant to boost the intervention (e.g., texting or calls from a health coach) are unlikely to hurt and may be beneficial.
For treatment professionals and treatment systems: While this study did not find that one booster strategy outperformed another, the nearly all-female sample of youth did report lower odds, on average, of alcohol consumption, aggression, and drug use and all their related consequences. This may suggest that receiving any booster has a positive effect for most young women. Accordingly, treatment systems and clinicians that aim to maximize resources may benefit from exploring brief interventions with follow up boosters. It is likely to help and unlikely to hurt in developing follow-ups post interventions, especially when those interventions are based in the emergency department as those in this study were.
For scientists: The current study was based in Flint, Michigan among youth reporting to emergency departments and reporting binge drinking and aggression. The study employed a brief intervention followed by an adaptive booster strategy that featured two stages of randomization to see if adapting the boosters to align with previous intervention response improved outcomes. This study did not find differences across first or second stage randomization. It may be that receiving any booster benefits youth; however, the study did not include a control group that did not receive any boosters, and the sample was nearly all young women whereas most binge drinking aggression occurs among young men. Future studies would benefit from a design that incorporated a control group to tease out the effects of receiving any booster. Furthermore, it is unknown whether the effects found for youth from baseline to 4- and 8-month follow up were a result of the brief intervention or something else (e.g., regression to the mean), though a prior study did show that the brief computerized intervention, especially when facilitated by a therapist, was better than simply receiving an brochure including community resources.
For policy makers: This study did not find differences across the intervention booster strategies. However, the mostly female sample of youth – all of whom received the brief intervention – had lower odds of alcohol consumption, aggression, and drug use along with their respective consequences, which may reflect the need for regular intervention boosters and follow ups to sustain the individual and societal level benefits from an alcohol and aggression intervention. Funding to research the best ways to address youth alcohol use and aggression may have exponential benefit that is also cost-effective.
Underage alcohol use is linked to disruptions in typical neurological development, a higher risk of developing alcohol use disorder later in life, and acute harms such as injuries, sexual assault, overdose, motor vehicle accidents, and death. Alcohol is also considered to be the most harmful substance to other people (e.g., assaults, domestic violence). In parallel, youth aggression also contributes significantly to public health concerns. For youth ages 15-19, homicide was the second leading cause of death in 2021. Thus, interventions for youth that lead to reduced alcohol use and aggression may have a meaningful individual and societal impacts.
A range of interventions have been shown to help reduce alcohol use among youth though many do not willingly attend treatment. Furthermore, typical programs taking several sessions can be costly and may not be feasible for many young people. Brief interventions—often delivered in a single session—are promising strategies that save resources, scale easily, and may improve outcomes. Incorporating technology and adaptive design elements may further enhance the effectiveness of these brief approaches without substantially increasing costs. For example, strategically allocating resources to individuals with the greatest need (i.e., adapting), assessed at multiple timepoints, may improve efficiency and support broader scalability. This study explored if adaptative boosters following a brief intervention for young people reporting to the emergency department had a differential effect on alcohol use and aggression.
HOW WAS THIS STUDY CONDUCTED?
This study was a sequential multiple assignment randomized trial among 400 youth (aged 14-20) that reported to the emergency department for any reason except sexual assault, child maltreatment, or suicide attempt/ideation. Youth who self-reported binge drinking (via the AUDIT-C assessment), physical aggression, and a cell phone with texting capabilities were eligible for the study. Following the initial baseline survey and enrollment, youth received a brief intervention followed by an 8-week sequential multiple assignment randomized trial (see graphic below for details). Then outcomes were measured at 4- and 8-months post brief intervention.
In this study, the sequential design featured two 4-week stages with weekly surveys and two primary booster conditions. The main aim of this study was to explore if changing the booster condition after 4-weeks impacted the intervention outcomes, which could suggest the efficiency of adapting resource allocation (e.g., more and less) at multiple timepoints to improve outcomes for youth.
All youth received the SafERteens single session brief intervention for alcohol use and aggression, which combines motivational interviewing and skills training. The brief intervention (averaging 32 minutes in this study) includes goal setting, tailored feedback, decisional balance exercise, role plays, and referrals. See graphic below for intervention details.
After the brief intervention, the participants received boosters: text messaging, telehealth calls from a health coach, both texts and telehealth calls, or a resource brochure. For the text messaging booster, youth received automated texts twice per day. The automated texts were pulled from a library of about 1200 possible texts that were created with feedback from youth advisors. Morning texts (10am-3pm) featured positive youth development messages related to coping with negative feelings, impulsivity, excitement, social support, hope, and leisure activities. Afternoon texts (4-9pm) featured reasons and tools to avoid or reduce alcohol use and aggression. One day per week included a cannabis-related message, and one day included a strength or positive quality that the youth participant had identified themselves in the prior weekly survey. The health coaching condition included calls from a trained health coach and featured motivational interviewing focused on personal goals and healthy lifestyles with strategies to avoid alcohol and aggression incorporated when possible.
The graphic below outlines how participants flowed through this multi-stage study. At the first stage, youth were randomly assigned to either receive the text messaging or health coach call. After the first 4-weeks, youth were identified as intervention responders or non-responders. Response status was determined by self-reports on the week 3 and 4 surveys. “Responders” were those who reported no binge drinking or aggression, and “non-responders” were those who reported binge drinking, aggression, both, or did not complete the survey.
At the second stage, responders were randomized to receive either the same condition (i.e., booster) or a minimized condition (health coach to texts or texts to resource brochure). Non-responders were re-randomized to receive either the same or an intensive condition (e.g., text messaging stepped up to health coach; health coach stepped up to health coach plus text messages). This 2-stage process results in 8 possible groups.
The first analysis compared texts versus heath coaching after the first 4-week stage on 4- and 8-month outcomes. The next group of analyses assessed responders and non-responders separately on 8-month outcomes accounting for the 4-month outcomes, age, and sex. The last group of analyses looked at overall changes from baseline to 8-month follow-up. The two primary outcomes were past 30-day alcohol use and past 30-day aggression, which could be toward friends, neighbors, relatives, acquaintances, dating partners, or strangers. Aggression was then made into a yes/no variable because it was so rarely reported. Secondary alcohol outcomes included alcohol misuse (yes/no), alcohol consequences, and violence-related consequences. Additional outcomes explored other drug-related measures including drug use severity and drug-related consequences.
There were 400 youth aged 14-20 years (average 18) enrolled in the study. Most of the youthwere female (78%), with 51% identifying as Black or African American, 40% White, and less than 10% as another race. Just over half (55%) received public assistance, and 99% were never married. At baseline, the average total number of drinks in the past 30 days was 29, and 52% met AUDIT-C cutoffs for harmful drinking (e.g., score of 3+ in adolescent females). Youth reported 7 alcohol-related consequences, on average. The average days of aggression was less than 1, and the average number of aggression-related consequences was 3. Most youth reported cannabis use (81%), although youth also reported “other illicit drug use” (23%), prescription opioid misuse (15%), prescription sedative misuse (17%), and prescription stimulant misuse (10%).
WHAT DID THIS STUDY FIND?
Booster strategies were equally effective
Outcomes were assessed related to both the first and second stage of randomization. There were no differences in the impact of the text messaging versus the health coaching on reducing alcohol consumption or aggression at the first stage. There were also no differences in alcohol misuse, alcohol-related consequences, aggression-related consequences, other drug use, or other drug-related consequences. Furthermore, the second stage booster strategies for responders and non-responders did not change the effects. For example, for those receiving text messages, adding health coaching did no better than continued text messages. Similarly, there were no differences across all outcomes.
Youth improved over time after receiving the intervention, however
Across all conditions, youth were 4 times as likely to report alcohol abstinence at 4 and 8 months compared to baseline. Among those that did report alcohol use, there was no improvement between baseline alcohol use frequency and the 4- or 8-month follow ups. Youth were nearly 10 times and 15 times more likely to have no alcohol-related consequences at the 4- and 8-month follow up, respectively.
Aggression was less likely at the 8-month follow up, but not the 4-month, compared to baseline. Specifically, participants were about half as likely to report aggression 8 months after the brief intervention. Other drug use apart from alcohol, other drug-related consequences, and aggression-related consequences were also less likely at the 4- and 8-month follow ups compared to baseline.
While these improvements are noteworthy, all individuals in the study received the brief intervention and there was no real non-treatment condition (although the type and intensity of texting and health coaching did vary across time). Consequently, we can’t know with certainty whether such improvements would have happened anyway without this intervention.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study did not find that adding either daily text messages or adding calls from a health coach improved outcomes when added to a brief intervention delivered in the emergency department. Furthermore, among those who did not have a positive response, outcomes were similar for more (e.g., texting to health coach calls) and less intense (e.g., texting to resource brochure) boosters. Overall, boosters did not differentially change the impact of the intervention on alcohol, aggression, or other drug outcomes. This could be good news: automated text messages were as effective as a live health coach phone call. That said, the study did not include a comparison group that received no booster, so it remains unclear whether boosters themselves led to improved outcomes.
More research is needed to disentangle the effects of the brief intervention and booster sessions, so that this empirically-supported approach to address youth alcohol use and aggression can be scaled in as cost-efficient manner as possible. It may be that certain youth may prefer or respond better to different types of approaches, but this was not examined in this study.
Of note there may have been a selection bias in the included study sample as most youth ED visits for alcohol/drug related aggression are male and almost four out of five study participants here were female. Though it is unclear why females were overrepresented, this unusual aspect of the study suggests results may have been different with more males represented and included in the study.
The majority of youth were female, and there were very few cases of aggression. These further limit the generalizability for the brief intervention and boosters’ impact on alcohol use and aggression across genders.
Public events (Flint Water Crisis, COVID-19, and recreational cannabis legalization) may have meaningfully impacted the behaviors that led to inclusions in the study (e.g., alcohol use) as well as changes over time. The variety of public health events that occurred during recruitment also limit the ability to generalize to youth in other locations or over time.
The study did not include a control that did not receive the brief intervention or a group that did not receive any boosters. The absence of control groups prevents us from knowing if the brief intervention impacted changes in outcomes or if receiving any booster altered outcomes.
BOTTOM LINE
Alcohol and aggression interventions for youth can be costly and time-consuming. Brief, single-session interventions paired with adaptive boosters—tailored based on recent behavior—have the potential to enhance effectiveness and efficiency, thereby improving scalability. In the current study, the adaptive boosters – automated text messaging and a health coach phone call – did equally as well. Given the ongoing need for effective and scalable approaches, continued rigorous research is essential to guide the development of future interventions and booster strategies for co-occurring youth alcohol use and aggression.
For individuals and families seeking recovery: This study did not find that one intervention booster strategy was better or worse than others in impacting alcohol or aggression outcomes. However, the nearly all-female sample of youth showed improvements in alcohol and aggression. It may be that receiving any intervention booster after the brief intervention positively impacted results for young women. If you or a loved one are engaging in an intervention, participating in actives meant to boost the intervention (e.g., texting or calls from a health coach) are unlikely to hurt and may be beneficial.
For treatment professionals and treatment systems: While this study did not find that one booster strategy outperformed another, the nearly all-female sample of youth did report lower odds, on average, of alcohol consumption, aggression, and drug use and all their related consequences. This may suggest that receiving any booster has a positive effect for most young women. Accordingly, treatment systems and clinicians that aim to maximize resources may benefit from exploring brief interventions with follow up boosters. It is likely to help and unlikely to hurt in developing follow-ups post interventions, especially when those interventions are based in the emergency department as those in this study were.
For scientists: The current study was based in Flint, Michigan among youth reporting to emergency departments and reporting binge drinking and aggression. The study employed a brief intervention followed by an adaptive booster strategy that featured two stages of randomization to see if adapting the boosters to align with previous intervention response improved outcomes. This study did not find differences across first or second stage randomization. It may be that receiving any booster benefits youth; however, the study did not include a control group that did not receive any boosters, and the sample was nearly all young women whereas most binge drinking aggression occurs among young men. Future studies would benefit from a design that incorporated a control group to tease out the effects of receiving any booster. Furthermore, it is unknown whether the effects found for youth from baseline to 4- and 8-month follow up were a result of the brief intervention or something else (e.g., regression to the mean), though a prior study did show that the brief computerized intervention, especially when facilitated by a therapist, was better than simply receiving an brochure including community resources.
For policy makers: This study did not find differences across the intervention booster strategies. However, the mostly female sample of youth – all of whom received the brief intervention – had lower odds of alcohol consumption, aggression, and drug use along with their respective consequences, which may reflect the need for regular intervention boosters and follow ups to sustain the individual and societal level benefits from an alcohol and aggression intervention. Funding to research the best ways to address youth alcohol use and aggression may have exponential benefit that is also cost-effective.
Underage alcohol use is linked to disruptions in typical neurological development, a higher risk of developing alcohol use disorder later in life, and acute harms such as injuries, sexual assault, overdose, motor vehicle accidents, and death. Alcohol is also considered to be the most harmful substance to other people (e.g., assaults, domestic violence). In parallel, youth aggression also contributes significantly to public health concerns. For youth ages 15-19, homicide was the second leading cause of death in 2021. Thus, interventions for youth that lead to reduced alcohol use and aggression may have a meaningful individual and societal impacts.
A range of interventions have been shown to help reduce alcohol use among youth though many do not willingly attend treatment. Furthermore, typical programs taking several sessions can be costly and may not be feasible for many young people. Brief interventions—often delivered in a single session—are promising strategies that save resources, scale easily, and may improve outcomes. Incorporating technology and adaptive design elements may further enhance the effectiveness of these brief approaches without substantially increasing costs. For example, strategically allocating resources to individuals with the greatest need (i.e., adapting), assessed at multiple timepoints, may improve efficiency and support broader scalability. This study explored if adaptative boosters following a brief intervention for young people reporting to the emergency department had a differential effect on alcohol use and aggression.
HOW WAS THIS STUDY CONDUCTED?
This study was a sequential multiple assignment randomized trial among 400 youth (aged 14-20) that reported to the emergency department for any reason except sexual assault, child maltreatment, or suicide attempt/ideation. Youth who self-reported binge drinking (via the AUDIT-C assessment), physical aggression, and a cell phone with texting capabilities were eligible for the study. Following the initial baseline survey and enrollment, youth received a brief intervention followed by an 8-week sequential multiple assignment randomized trial (see graphic below for details). Then outcomes were measured at 4- and 8-months post brief intervention.
In this study, the sequential design featured two 4-week stages with weekly surveys and two primary booster conditions. The main aim of this study was to explore if changing the booster condition after 4-weeks impacted the intervention outcomes, which could suggest the efficiency of adapting resource allocation (e.g., more and less) at multiple timepoints to improve outcomes for youth.
All youth received the SafERteens single session brief intervention for alcohol use and aggression, which combines motivational interviewing and skills training. The brief intervention (averaging 32 minutes in this study) includes goal setting, tailored feedback, decisional balance exercise, role plays, and referrals. See graphic below for intervention details.
After the brief intervention, the participants received boosters: text messaging, telehealth calls from a health coach, both texts and telehealth calls, or a resource brochure. For the text messaging booster, youth received automated texts twice per day. The automated texts were pulled from a library of about 1200 possible texts that were created with feedback from youth advisors. Morning texts (10am-3pm) featured positive youth development messages related to coping with negative feelings, impulsivity, excitement, social support, hope, and leisure activities. Afternoon texts (4-9pm) featured reasons and tools to avoid or reduce alcohol use and aggression. One day per week included a cannabis-related message, and one day included a strength or positive quality that the youth participant had identified themselves in the prior weekly survey. The health coaching condition included calls from a trained health coach and featured motivational interviewing focused on personal goals and healthy lifestyles with strategies to avoid alcohol and aggression incorporated when possible.
The graphic below outlines how participants flowed through this multi-stage study. At the first stage, youth were randomly assigned to either receive the text messaging or health coach call. After the first 4-weeks, youth were identified as intervention responders or non-responders. Response status was determined by self-reports on the week 3 and 4 surveys. “Responders” were those who reported no binge drinking or aggression, and “non-responders” were those who reported binge drinking, aggression, both, or did not complete the survey.
At the second stage, responders were randomized to receive either the same condition (i.e., booster) or a minimized condition (health coach to texts or texts to resource brochure). Non-responders were re-randomized to receive either the same or an intensive condition (e.g., text messaging stepped up to health coach; health coach stepped up to health coach plus text messages). This 2-stage process results in 8 possible groups.
The first analysis compared texts versus heath coaching after the first 4-week stage on 4- and 8-month outcomes. The next group of analyses assessed responders and non-responders separately on 8-month outcomes accounting for the 4-month outcomes, age, and sex. The last group of analyses looked at overall changes from baseline to 8-month follow-up. The two primary outcomes were past 30-day alcohol use and past 30-day aggression, which could be toward friends, neighbors, relatives, acquaintances, dating partners, or strangers. Aggression was then made into a yes/no variable because it was so rarely reported. Secondary alcohol outcomes included alcohol misuse (yes/no), alcohol consequences, and violence-related consequences. Additional outcomes explored other drug-related measures including drug use severity and drug-related consequences.
There were 400 youth aged 14-20 years (average 18) enrolled in the study. Most of the youthwere female (78%), with 51% identifying as Black or African American, 40% White, and less than 10% as another race. Just over half (55%) received public assistance, and 99% were never married. At baseline, the average total number of drinks in the past 30 days was 29, and 52% met AUDIT-C cutoffs for harmful drinking (e.g., score of 3+ in adolescent females). Youth reported 7 alcohol-related consequences, on average. The average days of aggression was less than 1, and the average number of aggression-related consequences was 3. Most youth reported cannabis use (81%), although youth also reported “other illicit drug use” (23%), prescription opioid misuse (15%), prescription sedative misuse (17%), and prescription stimulant misuse (10%).
WHAT DID THIS STUDY FIND?
Booster strategies were equally effective
Outcomes were assessed related to both the first and second stage of randomization. There were no differences in the impact of the text messaging versus the health coaching on reducing alcohol consumption or aggression at the first stage. There were also no differences in alcohol misuse, alcohol-related consequences, aggression-related consequences, other drug use, or other drug-related consequences. Furthermore, the second stage booster strategies for responders and non-responders did not change the effects. For example, for those receiving text messages, adding health coaching did no better than continued text messages. Similarly, there were no differences across all outcomes.
Youth improved over time after receiving the intervention, however
Across all conditions, youth were 4 times as likely to report alcohol abstinence at 4 and 8 months compared to baseline. Among those that did report alcohol use, there was no improvement between baseline alcohol use frequency and the 4- or 8-month follow ups. Youth were nearly 10 times and 15 times more likely to have no alcohol-related consequences at the 4- and 8-month follow up, respectively.
Aggression was less likely at the 8-month follow up, but not the 4-month, compared to baseline. Specifically, participants were about half as likely to report aggression 8 months after the brief intervention. Other drug use apart from alcohol, other drug-related consequences, and aggression-related consequences were also less likely at the 4- and 8-month follow ups compared to baseline.
While these improvements are noteworthy, all individuals in the study received the brief intervention and there was no real non-treatment condition (although the type and intensity of texting and health coaching did vary across time). Consequently, we can’t know with certainty whether such improvements would have happened anyway without this intervention.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study did not find that adding either daily text messages or adding calls from a health coach improved outcomes when added to a brief intervention delivered in the emergency department. Furthermore, among those who did not have a positive response, outcomes were similar for more (e.g., texting to health coach calls) and less intense (e.g., texting to resource brochure) boosters. Overall, boosters did not differentially change the impact of the intervention on alcohol, aggression, or other drug outcomes. This could be good news: automated text messages were as effective as a live health coach phone call. That said, the study did not include a comparison group that received no booster, so it remains unclear whether boosters themselves led to improved outcomes.
More research is needed to disentangle the effects of the brief intervention and booster sessions, so that this empirically-supported approach to address youth alcohol use and aggression can be scaled in as cost-efficient manner as possible. It may be that certain youth may prefer or respond better to different types of approaches, but this was not examined in this study.
Of note there may have been a selection bias in the included study sample as most youth ED visits for alcohol/drug related aggression are male and almost four out of five study participants here were female. Though it is unclear why females were overrepresented, this unusual aspect of the study suggests results may have been different with more males represented and included in the study.
The majority of youth were female, and there were very few cases of aggression. These further limit the generalizability for the brief intervention and boosters’ impact on alcohol use and aggression across genders.
Public events (Flint Water Crisis, COVID-19, and recreational cannabis legalization) may have meaningfully impacted the behaviors that led to inclusions in the study (e.g., alcohol use) as well as changes over time. The variety of public health events that occurred during recruitment also limit the ability to generalize to youth in other locations or over time.
The study did not include a control that did not receive the brief intervention or a group that did not receive any boosters. The absence of control groups prevents us from knowing if the brief intervention impacted changes in outcomes or if receiving any booster altered outcomes.
BOTTOM LINE
Alcohol and aggression interventions for youth can be costly and time-consuming. Brief, single-session interventions paired with adaptive boosters—tailored based on recent behavior—have the potential to enhance effectiveness and efficiency, thereby improving scalability. In the current study, the adaptive boosters – automated text messaging and a health coach phone call – did equally as well. Given the ongoing need for effective and scalable approaches, continued rigorous research is essential to guide the development of future interventions and booster strategies for co-occurring youth alcohol use and aggression.
For individuals and families seeking recovery: This study did not find that one intervention booster strategy was better or worse than others in impacting alcohol or aggression outcomes. However, the nearly all-female sample of youth showed improvements in alcohol and aggression. It may be that receiving any intervention booster after the brief intervention positively impacted results for young women. If you or a loved one are engaging in an intervention, participating in actives meant to boost the intervention (e.g., texting or calls from a health coach) are unlikely to hurt and may be beneficial.
For treatment professionals and treatment systems: While this study did not find that one booster strategy outperformed another, the nearly all-female sample of youth did report lower odds, on average, of alcohol consumption, aggression, and drug use and all their related consequences. This may suggest that receiving any booster has a positive effect for most young women. Accordingly, treatment systems and clinicians that aim to maximize resources may benefit from exploring brief interventions with follow up boosters. It is likely to help and unlikely to hurt in developing follow-ups post interventions, especially when those interventions are based in the emergency department as those in this study were.
For scientists: The current study was based in Flint, Michigan among youth reporting to emergency departments and reporting binge drinking and aggression. The study employed a brief intervention followed by an adaptive booster strategy that featured two stages of randomization to see if adapting the boosters to align with previous intervention response improved outcomes. This study did not find differences across first or second stage randomization. It may be that receiving any booster benefits youth; however, the study did not include a control group that did not receive any boosters, and the sample was nearly all young women whereas most binge drinking aggression occurs among young men. Future studies would benefit from a design that incorporated a control group to tease out the effects of receiving any booster. Furthermore, it is unknown whether the effects found for youth from baseline to 4- and 8-month follow up were a result of the brief intervention or something else (e.g., regression to the mean), though a prior study did show that the brief computerized intervention, especially when facilitated by a therapist, was better than simply receiving an brochure including community resources.
For policy makers: This study did not find differences across the intervention booster strategies. However, the mostly female sample of youth – all of whom received the brief intervention – had lower odds of alcohol consumption, aggression, and drug use along with their respective consequences, which may reflect the need for regular intervention boosters and follow ups to sustain the individual and societal level benefits from an alcohol and aggression intervention. Funding to research the best ways to address youth alcohol use and aggression may have exponential benefit that is also cost-effective.