Improvements in recovery capital associated with improvement after incarceration
The period following incarceration is a challenging one for individuals with substance use disorder, in part due to limited access to helpful recovery resources (recovery capital) upon release. This study examined recovery capital over time for individuals participating in an addiction medicine clinic after incarceration and whether recovery capital improvements were associated with changes in criminal activity, methamphetamine use, and alcohol use.
Harms from substances are common among people who are incarcerated, with research suggesting that 85% of people in the carceral system either meet criteria for a substance use disorder or were charged with a drug-related crime. The period following reentry post-incarceration is a vulnerable time for individuals with opioid or methamphetamine use disorder. Compared to the general population, the period following reentry post-incarceration for inmates with a substance use disorder history is associated with higher likelihood of return to use and crime recidivism. Further, overdose is more likely to occur after periods of abstinence (particularly for opioid use disorder) due to reduced neurophysiological tolerance. For individuals with opioid use disorder specifically, agonist medications like buprenorphine and methadone have been shown to reduce overdose risk. In addition to the benefits of medication, more research examining psychological and social improvements associated with reduced recidivism and return to substance use would directly benefit formerly incarcerated individuals.
Research shows individuals with greater recovery capital – the acquisition and/or use of available resources that can be accessed to support the initiation and maintenance of recovery from substance use disorder – report improved recovery outcomes over time. Incarceration is a process that often systematically removes access to resources and experiences that would enhance recovery capital (e.g., employment), an effect that can linger post-incarceration through stigma and rights restrictions for the formerly incarcerated in the United States. Efforts to bolster recovery capital among those re-entering post-incarceration may reduce the likelihood of recidivism and return to substance use.
This study examined whether increased recovery capital among individuals receiving active case management and financial support within an addiction medicine clinic after incarceration was associated with changes in criminal activity, methamphetamine use, and alcohol use.
HOW WAS THIS STUDY CONDUCTED?
The study took place in Iowa City, Iowa. The researchers used a single-group, prospective observational design. The researchers collected data from 136 people with opioid or methamphetamine use disorder released from the carceral system within the past year, 115 of which completed a 6-month follow up, comprising the analyzed sample. The researchers found no differences when comparing baseline values of recovery capital, crimes committed, days of substance use, or whether they were on medication between those who completed the study and those who did not. Inclusion criteria were patients 18 years or older, diagnosed with an opioid use disorder or stimulant use disorder, who possessed spoken English proficiency adequate to participate in case management, and who were planning to continue care for at least 6 months. All participants were involved in case management within an addiction medicine clinic prioritizing engagement and patient-centered treatment. Through the addiction medicine clinic, all participants had access to funds (typically totaling less than $5000 per participant available through the clinic) that could be used for resources and activities that typically have recovery capital value, such as medications for opioid use disorder (e.g., buprenorphine), dental care, transportation to clinic appointments, gym memberships, and educational needs. Participants completed one survey upon establishing care within the addiction medicine clinic, and an identical, second survey six months later. Participants were engaged within the clinic to various degrees throughout the study period.
Study surveys measured recovery capital (using the Assessment of Recovery Capital), days of alcohol use, days of methamphetamine use, and the number of crimes committed in the past 30 days. The study did not include a measure of past 30-day opioid use, and therefore this was not included in the current analyses. Due to large portions of the sample reporting no crimes committed or alcohol or methamphetamine use, the researchers examined categorical (yes/no) rather than continuous outcomes. The researchers tested whether recovery capital, substance use, and crimes committed changed over the course of the 6 months of involvement with the addiction medicine clinic, and whether greater improvements in recovery capital were associated with reductions in substance use and crimes committed. Analyses evaluating whether change in recovery capital predicted substance use or crimes committed included age, sex, cohort site, baseline recovery capital, and baseline substance use, or crimes committed respectively to each model. Controlling for the baseline recovery capital across all models, and substance use, and crimes committed in each respective model, allowed for the researchers to test whether changes in recovery capital were uniquely associated with changes in each substance use and crime outcome.
The sample was 69.9% male sex assigned at birth, 91.2% white, and 88% had at least a high school diploma or equivalent. Half (50%) of the sample was diagnosed with a stimulant use disorder (>90% methamphetamine), and 77.9% were diagnosed with an opioid use disorder. 32.4% of participants reported no medication for addiction treatment; 56.6% reported a prescription for buprenorphine, 9.6% reported a prescription for methadone, and 1.5% reported a prescription for naltrexone. At baseline, participants reported 1.1 (SD = 3.6) days of alcohol use, 2.4 (SD = 6.1) days of methamphetamine use, and 7.9 (SD = 13.8) crimes committed on average in the past 30 days.
WHAT DID THIS STUDY FIND?
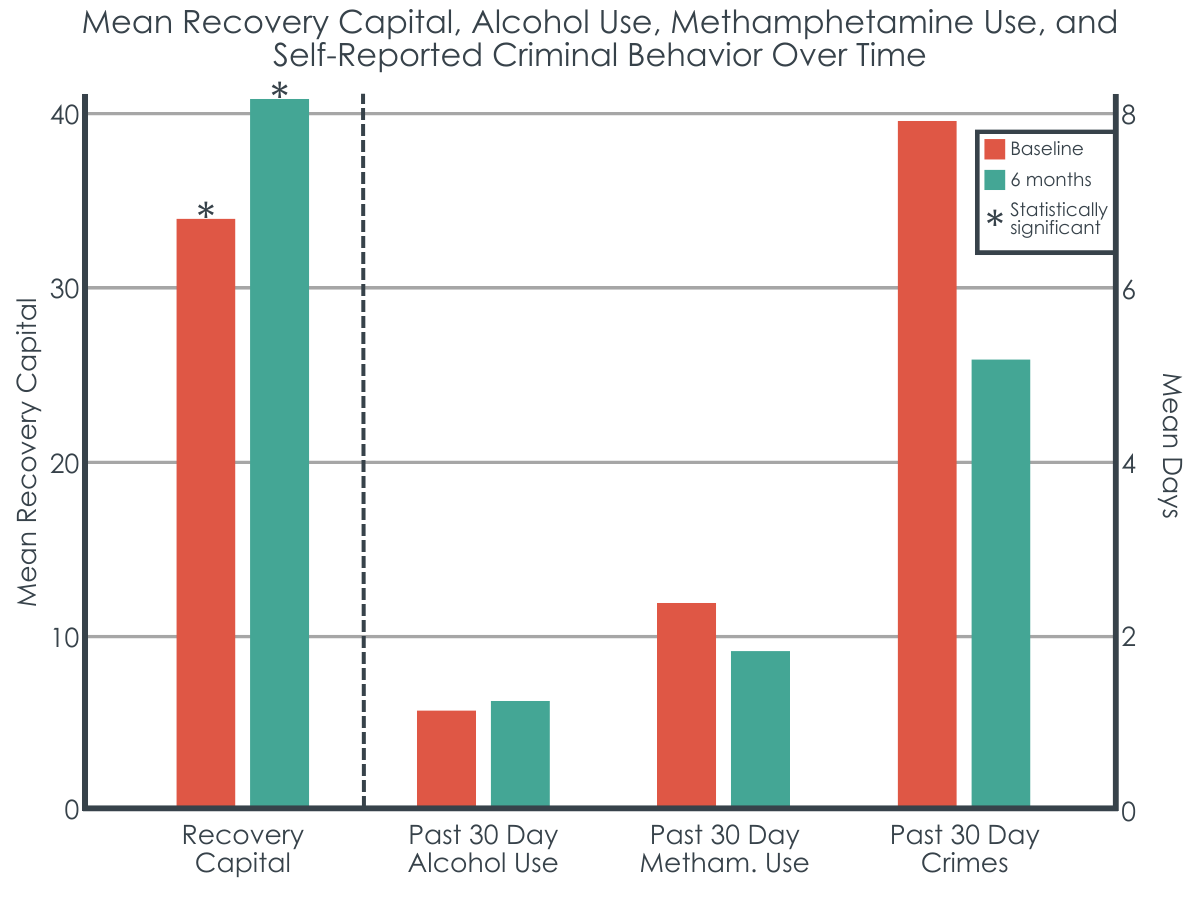
Recovery capital increased over 6 months and was the only statistically significant difference.
Recovery capital increased over the course of the 6 months from an average of 34.1 (SD = 11.1) to 40.3 (SD = 9.4); however, there were no differences in the number of days of alcohol or methamphetamine use or the number of crimes committed from baseline to 6 months. The researchers found that improvements in recovery capital were associated with reduced likelihood of reporting any substance use or crimes committed in the past 30 days. More specifically, a 1 standard deviation increase in recovery capital (e.g., from 34.1 to 45.2) was associated with a 68%, 82%, and 66% reduction in the likelihood that a participant would report past 30-day criminal activity, alcohol use, or methamphetamine use, respectively. Thus, the actual magnitude change in recovery capital was about one half of that (i.e., an absolute change score equal to approximately one half a standard deviation).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For those reentering the community post-incarceration, early improvements in recovery capital are associated with reduced likelihood of alcohol use, methamphetamine use, and criminal activity.
The period following reentry post-incarceration is a vulnerable time for individuals with opioid and methamphetamine use disorder and is associated with higher likelihood of return to use and recidivism. Incarceration often systematically removes access to recovery capital, bolstering the importance of building recovery capital upon community reentry among formerly incarcerated people. In the current study, researchers found that recovery capital increased on average among formerly incarcerated people engaged in an addiction medicine clinic, and that increased recovery capital was associated with 60-75% reduced likelihood of alcohol and methamphetamine use and criminal activity. Reductions in methamphetamine use are particularly significant considering that there are currently no FDA approved medications for methamphetamine.
This study and others support the importance of building recovery capital in early recovery. The current study design cannot isolate the cause of the increase in recovery capital; in other words, the researchers did not measure engagement in the addiction medicine clinic against a comparison group, and the degree to which recovery capital increased due to participation in the addiction medicine clinic and access to its resources (e.g., services covered financially up to $5000 in value) or for other reasons remains unknown. However, several elements of the case management in the addiction medicine clinic are consistent with robust and evidence-based strategies for reducing substance use disorder common in other treatments approaches, including the strategies used increased access to drug-specific treatment, medical treatment, and alternative, enjoyable activities that compete with substance use. This program also offered transportation, which addresses accessibility for certain aspects of recovery capital, and may be a critical component partially accounting for the success of the program. Future research should determine which of these strategies are the most necessary to increase which aspects of recovery capital.
The researchers did not randomize participants to engagement in the addiction medicine clinic or another control intervention, so while recovery capital did increase, it Is not possible to determine whether engagement with the addiction medicine clinic was the cause of these improvements in recovery capital. Future research should explore particular strategies implemented through addiction medicine clinics or other services to determine which approaches are associated with the greatest boast in recovery capital.
Recovery capital is a multidimensional construct theoretically consisting of four domains: social, physical, human, and cultural capital. In the current study, recovery capital was considered more broadly, and these separate domains were not examined specifically, and so we do not necessarily know whether changes some domains occurred more than others, or whether such changes in some domains were associated with varying reductions in substance use days and criminal activity.
Although the current study explored associations among people diagnosed with an opioid use disorder, a measure of past 30-day illicit opioid use was not included in the study.
Analyses included only study completers and did not include those that did not complete the 6-month assessment. The findings may only apply to those with the greatest levels of motivation for change.
BOTTOM LINE
The period following reentry post-incarceration is a vulnerable time for individuals with opioid use disorder and methamphetamine use disorder associated with higher likelihood of return to drug use and crime recidivism. Incarceration is a process that often systematically constrains access to recovery capital upon re-entry, an effect that can linger post-incarceration through stigma and rights restrictions (e.g., on employment opportunities) for the formerly incarcerated in the United States. Increasing recovery capital may result in decreased likelihood of recidivism and substance use post-incarceration, though more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population.
For individuals and families seeking recovery: Nurturing and growing recovery capital in early recovery can be difficult, particularly when returning to the community from incarceration. While more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population, a strong repertoire of recovery capital may help reduce substance use during this critical time and increase the chances of staying out of prison in the future. These strategies may include linkages to recovery support services such as recovery community centers, mutual-help organizations like alcoholics anonymous, or identifying and working with a peer recovery coach. More generally, spending more time with people who are supportive of your recovery and engaging in enjoyable and meaningful activities, such as exercise, reading, developing a hobby, or becoming involved in a volunteer organization, are also promising strategies for building recovery capital.
For treatment professionals and treatment systems: The findings suggest that targeting recovery capital among those reentering the community post-incarceration may pay dividends in reducing the likelihood of substance use and recidivism. While more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population, strategies such as those used in the addiction medicine clinic from the current study, such as increasing substance treatment access (e.g., paying for transportation to treatment), medical treatment, and access to meaningful activities (e.g., gym memberships) may be useful for enhancing recovery capital in this population.
For scientists: Findings from the current study continue to build upon a robust literature illustrating the protective nature of recovery capital among people in early recovery by extending such findings longitudinally to a formerly incarcerated population. Future research may clarify which domains of recovery support are the most important in this population. Further, the current study did not use randomization or include a comparison group, and it is unclear whether case management in the addiction management clinic in the current study was responsible for the increases in recovery capital. Future research may determine which strategies are most likely to help mobilize recovery capital among individuals in early recovery. Finally, given that analyses included only completers, the findings may only apply to those with greatest levels of engagement.
For policy makers: One primary goal of incarceration is rehabilitation. This goal may be more likely to be achieved if people reentering the community post-incarceration are provided with opportunities to build recovery capital. This may be accomplished through case management in the context of addiction medicine clinics. More funding to assess recovery capital accrual in the immediate period post-incarceration would help establish the most promising and cost-effective ways to achieve such goals in this population. Working with treatment professionals and scientists to establish policies and regulations may also help maximize rehabilitation and success in building recovery in the period following incarceration.
Harms from substances are common among people who are incarcerated, with research suggesting that 85% of people in the carceral system either meet criteria for a substance use disorder or were charged with a drug-related crime. The period following reentry post-incarceration is a vulnerable time for individuals with opioid or methamphetamine use disorder. Compared to the general population, the period following reentry post-incarceration for inmates with a substance use disorder history is associated with higher likelihood of return to use and crime recidivism. Further, overdose is more likely to occur after periods of abstinence (particularly for opioid use disorder) due to reduced neurophysiological tolerance. For individuals with opioid use disorder specifically, agonist medications like buprenorphine and methadone have been shown to reduce overdose risk. In addition to the benefits of medication, more research examining psychological and social improvements associated with reduced recidivism and return to substance use would directly benefit formerly incarcerated individuals.
Research shows individuals with greater recovery capital – the acquisition and/or use of available resources that can be accessed to support the initiation and maintenance of recovery from substance use disorder – report improved recovery outcomes over time. Incarceration is a process that often systematically removes access to resources and experiences that would enhance recovery capital (e.g., employment), an effect that can linger post-incarceration through stigma and rights restrictions for the formerly incarcerated in the United States. Efforts to bolster recovery capital among those re-entering post-incarceration may reduce the likelihood of recidivism and return to substance use.
This study examined whether increased recovery capital among individuals receiving active case management and financial support within an addiction medicine clinic after incarceration was associated with changes in criminal activity, methamphetamine use, and alcohol use.
HOW WAS THIS STUDY CONDUCTED?
The study took place in Iowa City, Iowa. The researchers used a single-group, prospective observational design. The researchers collected data from 136 people with opioid or methamphetamine use disorder released from the carceral system within the past year, 115 of which completed a 6-month follow up, comprising the analyzed sample. The researchers found no differences when comparing baseline values of recovery capital, crimes committed, days of substance use, or whether they were on medication between those who completed the study and those who did not. Inclusion criteria were patients 18 years or older, diagnosed with an opioid use disorder or stimulant use disorder, who possessed spoken English proficiency adequate to participate in case management, and who were planning to continue care for at least 6 months. All participants were involved in case management within an addiction medicine clinic prioritizing engagement and patient-centered treatment. Through the addiction medicine clinic, all participants had access to funds (typically totaling less than $5000 per participant available through the clinic) that could be used for resources and activities that typically have recovery capital value, such as medications for opioid use disorder (e.g., buprenorphine), dental care, transportation to clinic appointments, gym memberships, and educational needs. Participants completed one survey upon establishing care within the addiction medicine clinic, and an identical, second survey six months later. Participants were engaged within the clinic to various degrees throughout the study period.
Study surveys measured recovery capital (using the Assessment of Recovery Capital), days of alcohol use, days of methamphetamine use, and the number of crimes committed in the past 30 days. The study did not include a measure of past 30-day opioid use, and therefore this was not included in the current analyses. Due to large portions of the sample reporting no crimes committed or alcohol or methamphetamine use, the researchers examined categorical (yes/no) rather than continuous outcomes. The researchers tested whether recovery capital, substance use, and crimes committed changed over the course of the 6 months of involvement with the addiction medicine clinic, and whether greater improvements in recovery capital were associated with reductions in substance use and crimes committed. Analyses evaluating whether change in recovery capital predicted substance use or crimes committed included age, sex, cohort site, baseline recovery capital, and baseline substance use, or crimes committed respectively to each model. Controlling for the baseline recovery capital across all models, and substance use, and crimes committed in each respective model, allowed for the researchers to test whether changes in recovery capital were uniquely associated with changes in each substance use and crime outcome.
The sample was 69.9% male sex assigned at birth, 91.2% white, and 88% had at least a high school diploma or equivalent. Half (50%) of the sample was diagnosed with a stimulant use disorder (>90% methamphetamine), and 77.9% were diagnosed with an opioid use disorder. 32.4% of participants reported no medication for addiction treatment; 56.6% reported a prescription for buprenorphine, 9.6% reported a prescription for methadone, and 1.5% reported a prescription for naltrexone. At baseline, participants reported 1.1 (SD = 3.6) days of alcohol use, 2.4 (SD = 6.1) days of methamphetamine use, and 7.9 (SD = 13.8) crimes committed on average in the past 30 days.
WHAT DID THIS STUDY FIND?
Recovery capital increased over 6 months and was the only statistically significant difference.
Recovery capital increased over the course of the 6 months from an average of 34.1 (SD = 11.1) to 40.3 (SD = 9.4); however, there were no differences in the number of days of alcohol or methamphetamine use or the number of crimes committed from baseline to 6 months. The researchers found that improvements in recovery capital were associated with reduced likelihood of reporting any substance use or crimes committed in the past 30 days. More specifically, a 1 standard deviation increase in recovery capital (e.g., from 34.1 to 45.2) was associated with a 68%, 82%, and 66% reduction in the likelihood that a participant would report past 30-day criminal activity, alcohol use, or methamphetamine use, respectively. Thus, the actual magnitude change in recovery capital was about one half of that (i.e., an absolute change score equal to approximately one half a standard deviation).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For those reentering the community post-incarceration, early improvements in recovery capital are associated with reduced likelihood of alcohol use, methamphetamine use, and criminal activity.
The period following reentry post-incarceration is a vulnerable time for individuals with opioid and methamphetamine use disorder and is associated with higher likelihood of return to use and recidivism. Incarceration often systematically removes access to recovery capital, bolstering the importance of building recovery capital upon community reentry among formerly incarcerated people. In the current study, researchers found that recovery capital increased on average among formerly incarcerated people engaged in an addiction medicine clinic, and that increased recovery capital was associated with 60-75% reduced likelihood of alcohol and methamphetamine use and criminal activity. Reductions in methamphetamine use are particularly significant considering that there are currently no FDA approved medications for methamphetamine.
This study and others support the importance of building recovery capital in early recovery. The current study design cannot isolate the cause of the increase in recovery capital; in other words, the researchers did not measure engagement in the addiction medicine clinic against a comparison group, and the degree to which recovery capital increased due to participation in the addiction medicine clinic and access to its resources (e.g., services covered financially up to $5000 in value) or for other reasons remains unknown. However, several elements of the case management in the addiction medicine clinic are consistent with robust and evidence-based strategies for reducing substance use disorder common in other treatments approaches, including the strategies used increased access to drug-specific treatment, medical treatment, and alternative, enjoyable activities that compete with substance use. This program also offered transportation, which addresses accessibility for certain aspects of recovery capital, and may be a critical component partially accounting for the success of the program. Future research should determine which of these strategies are the most necessary to increase which aspects of recovery capital.
The researchers did not randomize participants to engagement in the addiction medicine clinic or another control intervention, so while recovery capital did increase, it Is not possible to determine whether engagement with the addiction medicine clinic was the cause of these improvements in recovery capital. Future research should explore particular strategies implemented through addiction medicine clinics or other services to determine which approaches are associated with the greatest boast in recovery capital.
Recovery capital is a multidimensional construct theoretically consisting of four domains: social, physical, human, and cultural capital. In the current study, recovery capital was considered more broadly, and these separate domains were not examined specifically, and so we do not necessarily know whether changes some domains occurred more than others, or whether such changes in some domains were associated with varying reductions in substance use days and criminal activity.
Although the current study explored associations among people diagnosed with an opioid use disorder, a measure of past 30-day illicit opioid use was not included in the study.
Analyses included only study completers and did not include those that did not complete the 6-month assessment. The findings may only apply to those with the greatest levels of motivation for change.
BOTTOM LINE
The period following reentry post-incarceration is a vulnerable time for individuals with opioid use disorder and methamphetamine use disorder associated with higher likelihood of return to drug use and crime recidivism. Incarceration is a process that often systematically constrains access to recovery capital upon re-entry, an effect that can linger post-incarceration through stigma and rights restrictions (e.g., on employment opportunities) for the formerly incarcerated in the United States. Increasing recovery capital may result in decreased likelihood of recidivism and substance use post-incarceration, though more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population.
For individuals and families seeking recovery: Nurturing and growing recovery capital in early recovery can be difficult, particularly when returning to the community from incarceration. While more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population, a strong repertoire of recovery capital may help reduce substance use during this critical time and increase the chances of staying out of prison in the future. These strategies may include linkages to recovery support services such as recovery community centers, mutual-help organizations like alcoholics anonymous, or identifying and working with a peer recovery coach. More generally, spending more time with people who are supportive of your recovery and engaging in enjoyable and meaningful activities, such as exercise, reading, developing a hobby, or becoming involved in a volunteer organization, are also promising strategies for building recovery capital.
For treatment professionals and treatment systems: The findings suggest that targeting recovery capital among those reentering the community post-incarceration may pay dividends in reducing the likelihood of substance use and recidivism. While more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population, strategies such as those used in the addiction medicine clinic from the current study, such as increasing substance treatment access (e.g., paying for transportation to treatment), medical treatment, and access to meaningful activities (e.g., gym memberships) may be useful for enhancing recovery capital in this population.
For scientists: Findings from the current study continue to build upon a robust literature illustrating the protective nature of recovery capital among people in early recovery by extending such findings longitudinally to a formerly incarcerated population. Future research may clarify which domains of recovery support are the most important in this population. Further, the current study did not use randomization or include a comparison group, and it is unclear whether case management in the addiction management clinic in the current study was responsible for the increases in recovery capital. Future research may determine which strategies are most likely to help mobilize recovery capital among individuals in early recovery. Finally, given that analyses included only completers, the findings may only apply to those with greatest levels of engagement.
For policy makers: One primary goal of incarceration is rehabilitation. This goal may be more likely to be achieved if people reentering the community post-incarceration are provided with opportunities to build recovery capital. This may be accomplished through case management in the context of addiction medicine clinics. More funding to assess recovery capital accrual in the immediate period post-incarceration would help establish the most promising and cost-effective ways to achieve such goals in this population. Working with treatment professionals and scientists to establish policies and regulations may also help maximize rehabilitation and success in building recovery in the period following incarceration.
Harms from substances are common among people who are incarcerated, with research suggesting that 85% of people in the carceral system either meet criteria for a substance use disorder or were charged with a drug-related crime. The period following reentry post-incarceration is a vulnerable time for individuals with opioid or methamphetamine use disorder. Compared to the general population, the period following reentry post-incarceration for inmates with a substance use disorder history is associated with higher likelihood of return to use and crime recidivism. Further, overdose is more likely to occur after periods of abstinence (particularly for opioid use disorder) due to reduced neurophysiological tolerance. For individuals with opioid use disorder specifically, agonist medications like buprenorphine and methadone have been shown to reduce overdose risk. In addition to the benefits of medication, more research examining psychological and social improvements associated with reduced recidivism and return to substance use would directly benefit formerly incarcerated individuals.
Research shows individuals with greater recovery capital – the acquisition and/or use of available resources that can be accessed to support the initiation and maintenance of recovery from substance use disorder – report improved recovery outcomes over time. Incarceration is a process that often systematically removes access to resources and experiences that would enhance recovery capital (e.g., employment), an effect that can linger post-incarceration through stigma and rights restrictions for the formerly incarcerated in the United States. Efforts to bolster recovery capital among those re-entering post-incarceration may reduce the likelihood of recidivism and return to substance use.
This study examined whether increased recovery capital among individuals receiving active case management and financial support within an addiction medicine clinic after incarceration was associated with changes in criminal activity, methamphetamine use, and alcohol use.
HOW WAS THIS STUDY CONDUCTED?
The study took place in Iowa City, Iowa. The researchers used a single-group, prospective observational design. The researchers collected data from 136 people with opioid or methamphetamine use disorder released from the carceral system within the past year, 115 of which completed a 6-month follow up, comprising the analyzed sample. The researchers found no differences when comparing baseline values of recovery capital, crimes committed, days of substance use, or whether they were on medication between those who completed the study and those who did not. Inclusion criteria were patients 18 years or older, diagnosed with an opioid use disorder or stimulant use disorder, who possessed spoken English proficiency adequate to participate in case management, and who were planning to continue care for at least 6 months. All participants were involved in case management within an addiction medicine clinic prioritizing engagement and patient-centered treatment. Through the addiction medicine clinic, all participants had access to funds (typically totaling less than $5000 per participant available through the clinic) that could be used for resources and activities that typically have recovery capital value, such as medications for opioid use disorder (e.g., buprenorphine), dental care, transportation to clinic appointments, gym memberships, and educational needs. Participants completed one survey upon establishing care within the addiction medicine clinic, and an identical, second survey six months later. Participants were engaged within the clinic to various degrees throughout the study period.
Study surveys measured recovery capital (using the Assessment of Recovery Capital), days of alcohol use, days of methamphetamine use, and the number of crimes committed in the past 30 days. The study did not include a measure of past 30-day opioid use, and therefore this was not included in the current analyses. Due to large portions of the sample reporting no crimes committed or alcohol or methamphetamine use, the researchers examined categorical (yes/no) rather than continuous outcomes. The researchers tested whether recovery capital, substance use, and crimes committed changed over the course of the 6 months of involvement with the addiction medicine clinic, and whether greater improvements in recovery capital were associated with reductions in substance use and crimes committed. Analyses evaluating whether change in recovery capital predicted substance use or crimes committed included age, sex, cohort site, baseline recovery capital, and baseline substance use, or crimes committed respectively to each model. Controlling for the baseline recovery capital across all models, and substance use, and crimes committed in each respective model, allowed for the researchers to test whether changes in recovery capital were uniquely associated with changes in each substance use and crime outcome.
The sample was 69.9% male sex assigned at birth, 91.2% white, and 88% had at least a high school diploma or equivalent. Half (50%) of the sample was diagnosed with a stimulant use disorder (>90% methamphetamine), and 77.9% were diagnosed with an opioid use disorder. 32.4% of participants reported no medication for addiction treatment; 56.6% reported a prescription for buprenorphine, 9.6% reported a prescription for methadone, and 1.5% reported a prescription for naltrexone. At baseline, participants reported 1.1 (SD = 3.6) days of alcohol use, 2.4 (SD = 6.1) days of methamphetamine use, and 7.9 (SD = 13.8) crimes committed on average in the past 30 days.
WHAT DID THIS STUDY FIND?
Recovery capital increased over 6 months and was the only statistically significant difference.
Recovery capital increased over the course of the 6 months from an average of 34.1 (SD = 11.1) to 40.3 (SD = 9.4); however, there were no differences in the number of days of alcohol or methamphetamine use or the number of crimes committed from baseline to 6 months. The researchers found that improvements in recovery capital were associated with reduced likelihood of reporting any substance use or crimes committed in the past 30 days. More specifically, a 1 standard deviation increase in recovery capital (e.g., from 34.1 to 45.2) was associated with a 68%, 82%, and 66% reduction in the likelihood that a participant would report past 30-day criminal activity, alcohol use, or methamphetamine use, respectively. Thus, the actual magnitude change in recovery capital was about one half of that (i.e., an absolute change score equal to approximately one half a standard deviation).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For those reentering the community post-incarceration, early improvements in recovery capital are associated with reduced likelihood of alcohol use, methamphetamine use, and criminal activity.
The period following reentry post-incarceration is a vulnerable time for individuals with opioid and methamphetamine use disorder and is associated with higher likelihood of return to use and recidivism. Incarceration often systematically removes access to recovery capital, bolstering the importance of building recovery capital upon community reentry among formerly incarcerated people. In the current study, researchers found that recovery capital increased on average among formerly incarcerated people engaged in an addiction medicine clinic, and that increased recovery capital was associated with 60-75% reduced likelihood of alcohol and methamphetamine use and criminal activity. Reductions in methamphetamine use are particularly significant considering that there are currently no FDA approved medications for methamphetamine.
This study and others support the importance of building recovery capital in early recovery. The current study design cannot isolate the cause of the increase in recovery capital; in other words, the researchers did not measure engagement in the addiction medicine clinic against a comparison group, and the degree to which recovery capital increased due to participation in the addiction medicine clinic and access to its resources (e.g., services covered financially up to $5000 in value) or for other reasons remains unknown. However, several elements of the case management in the addiction medicine clinic are consistent with robust and evidence-based strategies for reducing substance use disorder common in other treatments approaches, including the strategies used increased access to drug-specific treatment, medical treatment, and alternative, enjoyable activities that compete with substance use. This program also offered transportation, which addresses accessibility for certain aspects of recovery capital, and may be a critical component partially accounting for the success of the program. Future research should determine which of these strategies are the most necessary to increase which aspects of recovery capital.
The researchers did not randomize participants to engagement in the addiction medicine clinic or another control intervention, so while recovery capital did increase, it Is not possible to determine whether engagement with the addiction medicine clinic was the cause of these improvements in recovery capital. Future research should explore particular strategies implemented through addiction medicine clinics or other services to determine which approaches are associated with the greatest boast in recovery capital.
Recovery capital is a multidimensional construct theoretically consisting of four domains: social, physical, human, and cultural capital. In the current study, recovery capital was considered more broadly, and these separate domains were not examined specifically, and so we do not necessarily know whether changes some domains occurred more than others, or whether such changes in some domains were associated with varying reductions in substance use days and criminal activity.
Although the current study explored associations among people diagnosed with an opioid use disorder, a measure of past 30-day illicit opioid use was not included in the study.
Analyses included only study completers and did not include those that did not complete the 6-month assessment. The findings may only apply to those with the greatest levels of motivation for change.
BOTTOM LINE
The period following reentry post-incarceration is a vulnerable time for individuals with opioid use disorder and methamphetamine use disorder associated with higher likelihood of return to drug use and crime recidivism. Incarceration is a process that often systematically constrains access to recovery capital upon re-entry, an effect that can linger post-incarceration through stigma and rights restrictions (e.g., on employment opportunities) for the formerly incarcerated in the United States. Increasing recovery capital may result in decreased likelihood of recidivism and substance use post-incarceration, though more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population.
For individuals and families seeking recovery: Nurturing and growing recovery capital in early recovery can be difficult, particularly when returning to the community from incarceration. While more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population, a strong repertoire of recovery capital may help reduce substance use during this critical time and increase the chances of staying out of prison in the future. These strategies may include linkages to recovery support services such as recovery community centers, mutual-help organizations like alcoholics anonymous, or identifying and working with a peer recovery coach. More generally, spending more time with people who are supportive of your recovery and engaging in enjoyable and meaningful activities, such as exercise, reading, developing a hobby, or becoming involved in a volunteer organization, are also promising strategies for building recovery capital.
For treatment professionals and treatment systems: The findings suggest that targeting recovery capital among those reentering the community post-incarceration may pay dividends in reducing the likelihood of substance use and recidivism. While more research is needed to develop and test strategies that can enhance recovery capital in this vulnerable population, strategies such as those used in the addiction medicine clinic from the current study, such as increasing substance treatment access (e.g., paying for transportation to treatment), medical treatment, and access to meaningful activities (e.g., gym memberships) may be useful for enhancing recovery capital in this population.
For scientists: Findings from the current study continue to build upon a robust literature illustrating the protective nature of recovery capital among people in early recovery by extending such findings longitudinally to a formerly incarcerated population. Future research may clarify which domains of recovery support are the most important in this population. Further, the current study did not use randomization or include a comparison group, and it is unclear whether case management in the addiction management clinic in the current study was responsible for the increases in recovery capital. Future research may determine which strategies are most likely to help mobilize recovery capital among individuals in early recovery. Finally, given that analyses included only completers, the findings may only apply to those with greatest levels of engagement.
For policy makers: One primary goal of incarceration is rehabilitation. This goal may be more likely to be achieved if people reentering the community post-incarceration are provided with opportunities to build recovery capital. This may be accomplished through case management in the context of addiction medicine clinics. More funding to assess recovery capital accrual in the immediate period post-incarceration would help establish the most promising and cost-effective ways to achieve such goals in this population. Working with treatment professionals and scientists to establish policies and regulations may also help maximize rehabilitation and success in building recovery in the period following incarceration.