WHAT PROBLEM DOES THIS STUDY ADDRESS?
Opioid withdrawal can be extremely uncomfortable, with agitation, flu-like symptoms, sweating, stomach cramps, and sleepless nights that can greatly increase risk for return to opioid use. The body’s stress response system is highly activated during these states with associated sympathetic nervous system engagement (the ‘fight-or-flight’ response) and parasympathetic nervous system inhibition (the ‘rest and digest’ response). Heart rate variability, a measure of the natural variation in the time between heartbeats, provides a window into respective sympathetic and parasympathetic nervous system engagement, and is also a biomarker of health. Higher heart rate variability reflects health, while lower heart rate variability is typically indicative of psychological or physical pathology. Medications like buprenorphine—a semisynthetic opioid used to treat opioid use disorder—help with opioid withdrawal symptoms but do not fully ameliorate the stress state associated with withdrawal. Mindfulness training has been used to offset autonomic dysregulation in other contexts but has more limited utility during acute withdrawal states when individuals are experiencing marked discomfort and typically have difficulty concentrating. Yoga can also directly engage the body’s parasympathetic nervous system to calm stress responses, and in the context of opioid withdrawal treatment, it may be a better fit than mindfulness practices because it uses movement, breathing techniques, and guided relaxation. The researchers in this study tested whether adding a structured yoga program to standard buprenorphine treatment could ease withdrawal symptoms more quickly by reducing the autonomic stress response associated with opioid withdrawal.
HOW WAS THIS STUDY CONDUCTED?
This study, conducted in India, was a randomized controlled trial with 59 adults with opioid use disorder experiencing mild to moderate withdrawal symptoms, comparing a yoga add-on therapy + standard buprenorphine and “routine clinical management” treatment to standard buprenorphine treatment alone and “routine clinical management”. Assessments of withdrawal stabilization and autonomic function were conducted at baseline and 2 weeks post-randomization. Those with severe withdrawal, neurological conditions affecting autonomic function, severe psychiatric conditions, or recent yoga training were excluded. Of 68 individuals screened, 59 were randomized: 30 to yoga add-on therapy and 29 to treatment-as-usual. Importantly, the yoga group was older at first substance use and first opioid use. Descriptively, they also had fewer opioid withdrawal symptoms and a slightly lower buprenorphine stabilization dose; though these differences were not statistically significant, smaller sample sizes like in this study make it difficult to detect small to moderate group differences. Overall, these baseline differences could mean the yoga group was less severe to begin with. All received standard buprenorphine with standard daily dose adjustments. Participants began at very low buprenorphine doses (e.g., 1 mg) and stabilized on very low doses during supervised withdrawal (e.g., 3 mg). The yoga group received 10 supervised 45 minute sessions over 14 days (over 90% completed at least 8 sessions), including relaxation practices, gentle postures, breathing exercises (left nostril breathing and humming breath), and guided relaxation designed to target restlessness, anxiety, and sympathetic nervous system hyperactivity. Primary outcomes were time to withdrawal stabilization (when symptoms dropped to minimal levels and stayed there) controlling for buprenorphine dose and heart rate variability measured via electrocardiography on days 1 and 15. Secondary outcomes included anxiety, self-reported time to fall asleep, and pain, measured at baseline and day 15. The all-male sample (reflecting local patterns) averaged 26 years old; with most identifying tapentadol as the primary opioid they used.
WHAT DID THIS STUDY FIND?
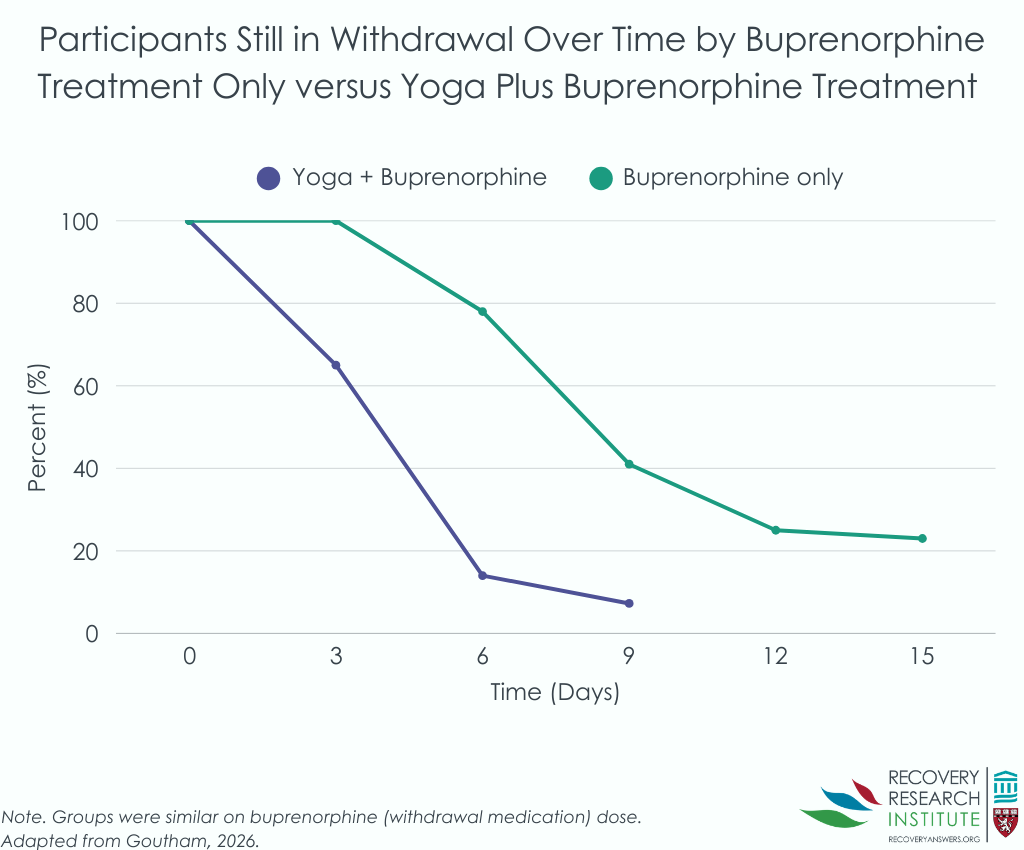
Participants receiving yoga stabilized about 4 times faster than those receiving medication alone, even after accounting for buprenorphine dose. Controlling for buprenorphine dose, median time to stabilization was 5 days in the yoga group versus 9 days in controls, effectively shortening the highest-risk withdrawal period by roughly 4 days (see graph below).
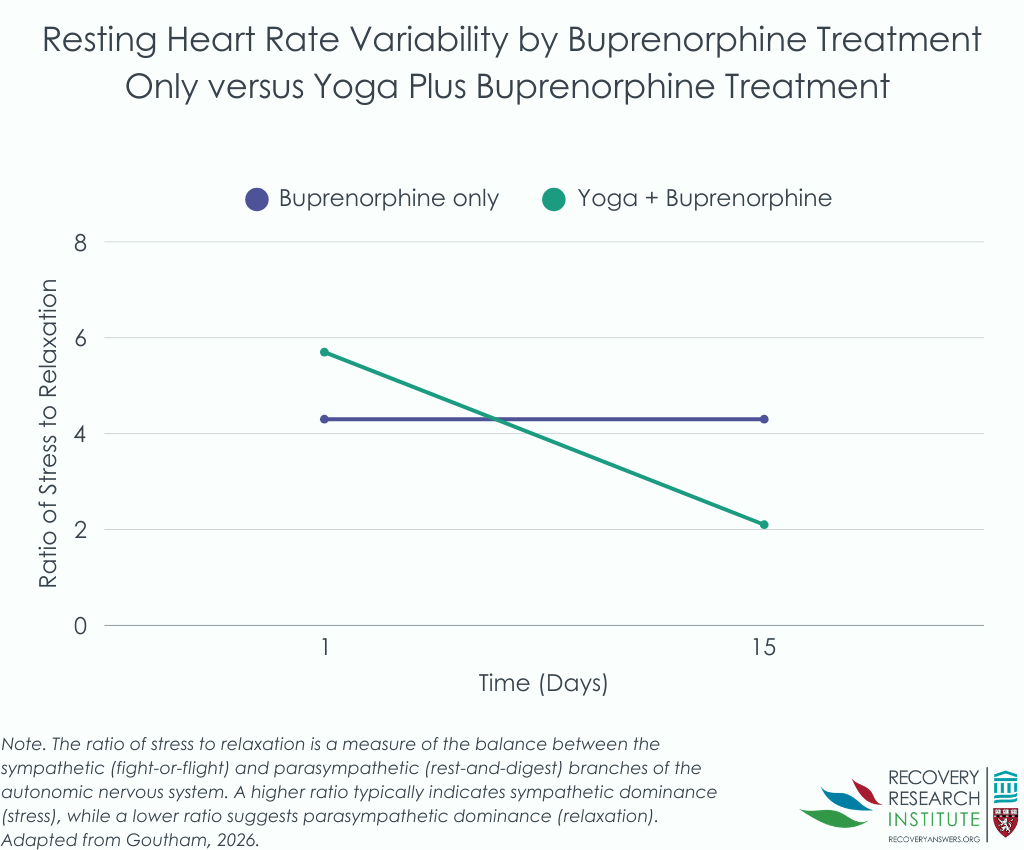
The yoga group showed substantial improvements in heart rate variability indicating enhanced parasympathetic (rest and digest) activity and better overall autonomic balance (see graph below). They had larger increases in high-frequency heart rate variability (a parasympathetic marker). Analyses suggested that increases in parasympathetic activity explained about 23% of yoga’s effect on faster stabilization, highlighting autonomic restoration as a meaningful mechanism.
Anxiety reduction was also substantially greater in the yoga group, with large effects comparable to established anxiety interventions. Sleep latency improved by about an hour more in the yoga group, and pain decreased more, with moderate effect sizes for both.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
These findings suggest that yoga may address a critical gap in standard opioid withdrawal care by targeting autonomic dysregulation that medications alone don’t fully resolve. The mechanistic evidence that autonomic improvements partially explained faster recovery suggests yoga may actually address underlying autonomic hyperarousal in withdrawal states, and not just mask distressing symptoms with positive feelings from yoga. By accelerating stabilization and improving parasympathetic functioning, yoga could shorten the period when individuals are most distressed and at highest risk for treatment dropout and relapse. Concurrent improvements in anxiety, sleep, and pain suggest yoga simultaneously may address multiple interconnected drivers of early relapse risk. One important caveat was that the yoga group may have begun the study with lower severity, which could account for some of their more rapid improvement during detoxification. This study should be replicated in larger samples where randomization is more likely to lead to balanced groups from the start. Nevertheless, yoga may be an especially attractive option as it involves physical and breathing practices accessible to most and deliverable even when one’s ability to concentrate is limited, as might be the case in detoxification settings.
It is worth noting that there are many different types of yoga and the one practiced here may have specific effects that do not generalize to all forms of yoga. That said, given yoga’s relatively low cost compared with prolonged inpatient stays, integrating it into withdrawal protocols could prove valuable if benefits generalize to other settings and populations. More work is needed, however, before broad implementation of yoga for opioid withdrawal. Though the study was well designed and executed, it had some important limitations that reduce its generalizability, including a single-site design, small and all-male sample, and short follow-up. Additionally, this study focused on individuals experiencing mild and moderate opioid withdrawal. Yoga may not help for severe opioid withdrawal given the debilitating nature of this state, but will need testing in that population.
BOTTOM LINE
For individuals with opioid use disorder undergoing medically managed mild or moderate withdrawal, adding structured yoga to standard medication may speed stabilization and help restore stress response functioning that medication alone doesn’t address, though more research in diverse populations and settings is needed. It is important to note that there are many different types of yoga and the one practiced here may have specific effects that do not generalize to all forms of yoga.
- For individuals and families seeking recovery: If you or a family member is entering opioid withdrawal treatment, asking whether yoga or similar breathing practices are available alongside medication may be worthwhile. This study suggests such practices could help the body recover more quickly and better manage the anxiety, sleep problems, and pain that make early recovery so challenging. It is important to note, however, that there are many different types of yoga and the one practiced here may have specific effects that do not generalize to all forms of yoga.
- For treatment professionals and treatment systems: Incorporating supervised yoga into inpatient opioid withdrawal protocols may accelerate stabilization and address autonomic hyperarousal that buprenorphine alone doesn’t fully correct. Implementation would require training yoga therapists or skilled staff and adaptation to local resources and cultural context.
- For scientists: This early-stage trial provides mechanistic evidence that this specific configuration of yoga practices accelerates opioid withdrawal recovery partially through parasympathetic restoration, with mediation analyses indicating heart rate variability changes explain a meaningful portion of the treatment effect. Future studies should incorporate active controls, larger and more diverse samples (including women and individuals using fentanyl), multisite designs, and longer follow-up examining relapse and functional outcomes.
- For policy makers: Evidence that yoga as adjunctive therapy can accelerate withdrawal stabilization while addressing autonomic dysregulation not fully managed by medication suggests potential value in supporting implementation research. Because the intervention is relatively low cost and may reduce time in the highest-risk treatment phase, integrating yoga into publicly funded addiction services could yield clinical and economic benefits if findings generalize. It is important to note, however, that there are many different types of yoga and the one practiced here may have specific effects that do not generalize to all forms of yoga.
CITATIONS
Goutham, S., Bhargav, H., Holla, B., Mahadevan, J., Nagendra, R. P., Jasti, N., Narasimha, V. L., Mehta, U. M., Varambally, S., Venkatasubramanian, G., Chand, P., Gangadhar, B. N., Hill, K. P., Keshavan, M., & Murthy, P. (2026). Yoga for opioid withdrawal and autonomic regulation: A randomized clinical trial. JAMA Psychiatry, 83(3), 238-246. doi: 10.1001/jamapsychiatry.2025.3863.












