Clinician attitudes toward medications for opioid use disorder
FDA-approved medications for opioid use disorder reduce opioid use and risk for overdose, but how clinicians feel about them can influence whether patients choose to take them. This study examined how non-prescribing clinicians perceive and present medications for opioid use disorders, highlighting areas where their perspectives align with or diverge from scientific evidence.
Fewer than a third of individuals with opioid use disorder or active opioid use take an FDA-approved medication like buprenorphine (often prescribed in formulation with naloxone known by the brand name Suboxone). Additionally, many who start medications for opioid use disorder discontinue within weeks.
Research indicates that attitudes and beliefs about medications for opioid use disorder strongly influence treatment acceptance and adherence. Negative perceptions can lead to shame and guilt, a form of stigma known as “intervention stigma,” which discourages continued use. Thus, these attitudes play a crucial, albeit indirect, role on the ultimate public health impact of medications for opioid use disorder. As primary points of contact for patients, therapists and other clinical staff play an important role in shaping perceptions of and access to medications for opioid use disorder. Their attitudes and beliefs can influence whether individuals feel encouraged or discouraged from initiating and maintaining these life-saving treatments.
This study characterized therapist attitudes toward each of the 3 FDA approved medications for opioid use disorder. Because they may have different attitudes toward agonist medications methadone and buprenorphine compared to the antagonist medication naltrexone (often prescribed as a monthly injection known by the brand name Vivitrol), the study assessed therapist perceptions of the advantages and disadvantages of each medication separately.
HOW WAS THIS STUDY CONDUCTED?
From June to December 2021, the research team used free-response questions to survey clinical staff at publicly funded substance use disorder treatment agencies who serve Medicaid recipients in Philadelphia operating under a municipality-wide mandate to offer medications for opioid use disorder. The goal was to understand how they view the benefits and drawbacks of 3 medications for opioid use disorder options: buprenorphine, methadone, and naltrexone.
A total of 271 counselors answered an open-ended question for each medication: “When discussing [medication name] with your patient, what would be the most important advantage and disadvantage to mention?” Their responses were then analyzed to identify recurring themes.
The research team used thematic analysis to characterize perceived advantages and disadvantages. The average clinician was 43 years old, with approximately 11 years of professional experience and nearly five years in their current role. The majority of respondents (71%) identified as women, while 27% identified as men, and 2% did not report their gender. Most staff had a college education, with 88% holding at least a bachelor’s degree and 61% having a master’s degree or higher. Regarding racial and ethnic backgrounds, 51% identified as White, 37% as Black, 3% as Asian/Pacific Islander, 0.4% as Native American, and 7% as another race. Additionally, 7% identified as Hispanic or Latino. Clinicians worked in agencies with varying levels of access to medications for opioid use disorder. The majority (73%) were at agencies that provided buprenorphine, and 82% were at agencies offering naltrexone. The most commonly prescribed form of naltrexone is the extended-release version, known also by the brand name Vivitrol, though this study does not specify the naltrexone formulation. Just less than half worked at agencies that prescribed or dispensed methadone, highlighting a gap in its availability.
WHAT DID THIS STUDY FIND?
Staff felt medications offered unique benefits based on patient needs
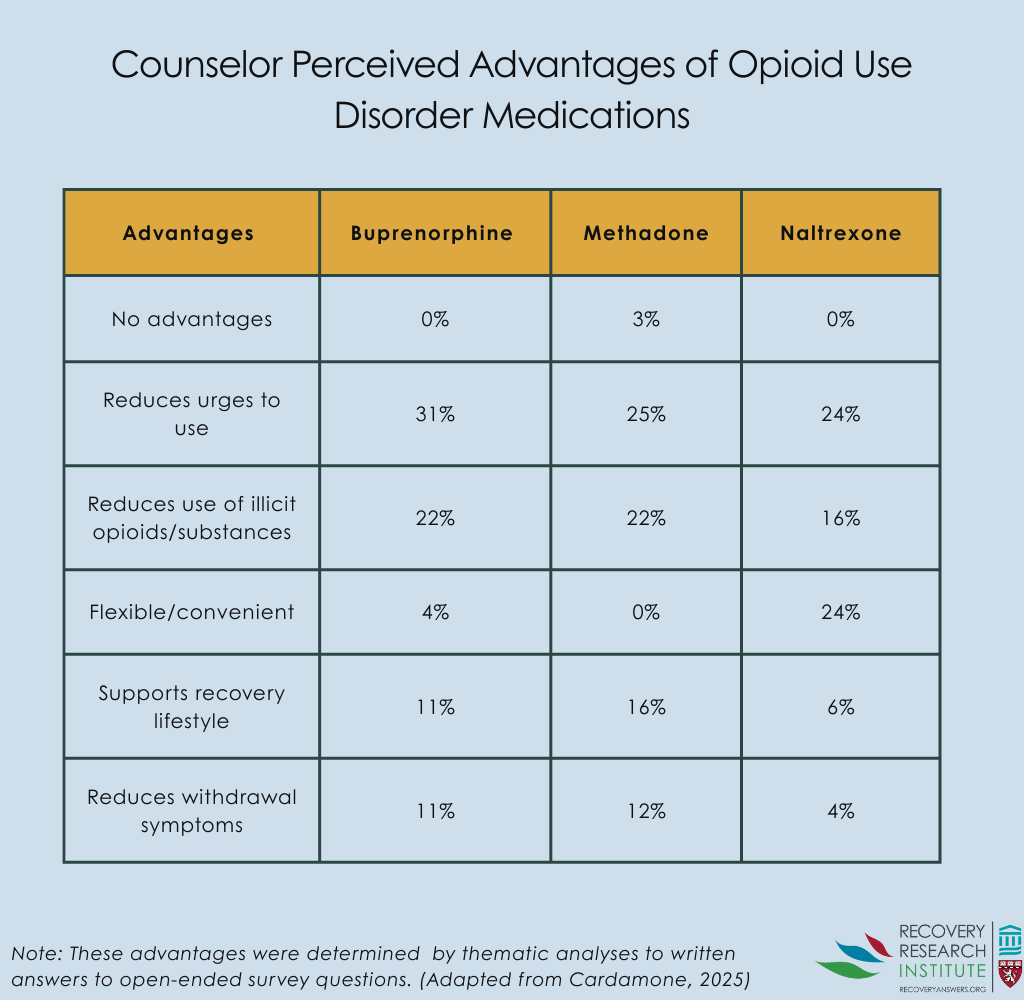
One of the most frequently cited benefits of medications for opioid use disorder generally was its ability to reduce opioid cravings, with 42% of clinicians emphasizing this advantage. The Figure below shows the proportion of staff citing advantages by medication type. Similarly, 37% of clinicians highlighted its role in decreasing illicit opioid use, helping patients transition away from unregulated substances. Convenience was another key factor, with 25% of clinicians identifying flexibility in treatment as a major benefit, particularly for medications with less rigid dosing schedules. Additionally, 20% of clinicians emphasized that medications for opioid use disorder support a stable recovery lifestyle, enabling patients to develop long-term habits that reinforce recovery. Lastly, 17% of clinicians recognized the ability of medications for opioid use disorder to ease withdrawal symptoms, though the degree of relief varied depending on the specific medication.
Staff also felt medications had several disadvantages
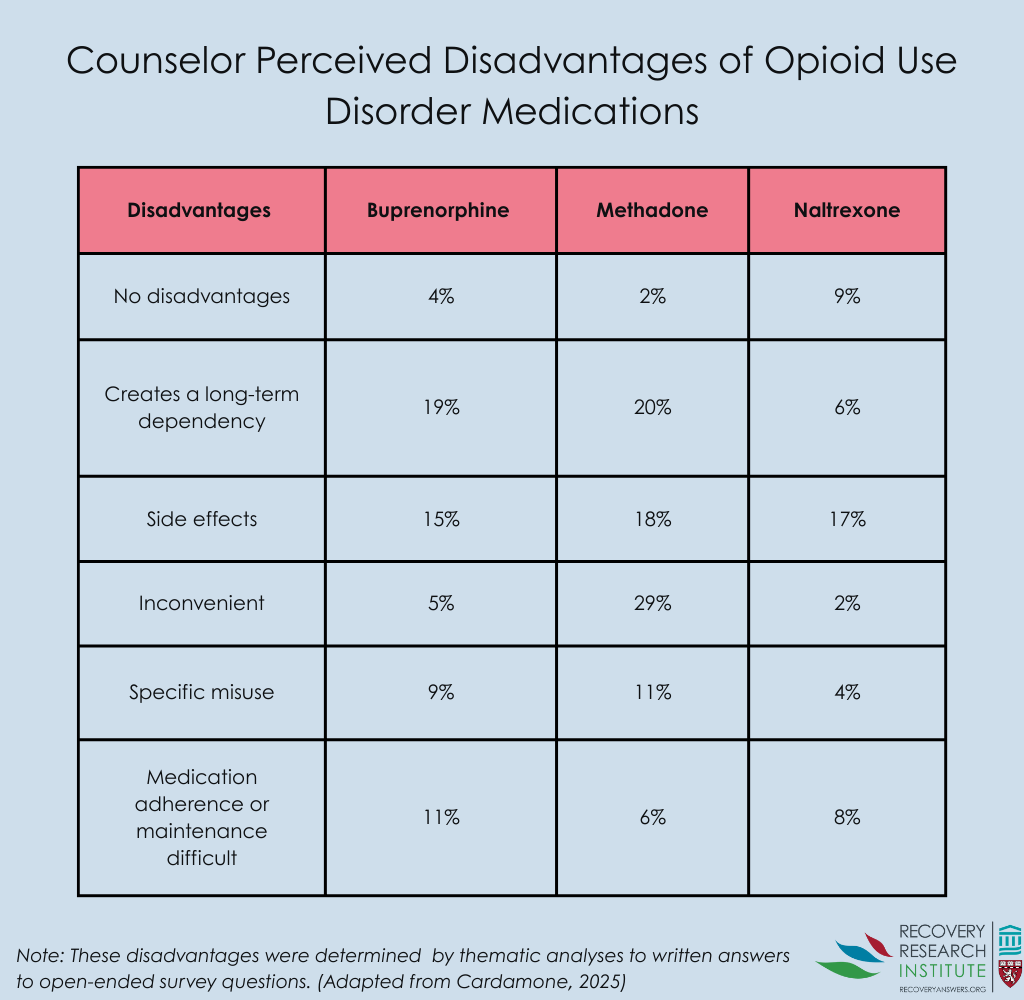
One of the most frequently cited concerns about medications for opioid use disorder was the risk of long-term dependency, with 30% of clinicians expressing this issue, particularly for buprenorphine and methadone. The figure below shows the proportion of staff citing disadvantages by medication type. Side effects were another major drawback, reported by 28% of clinicians, with each medication presenting different physical challenges for patients. Treatment inconvenience was also a significant barrier, highlighted by 27% of clinicians, especially for medications requiring frequent clinic visits or strict adherence to dosing schedules. Additionally, 17% of clinicians raised concerns about misuse and diversion, particularly for buprenorphine (9%) and methadone (11%), citing issues such as selling, mixing with other substances, or improper use. Lastly, 16% of clinicians identified medication adherence and maintenance as a challenge, particularly for buprenorphine (11%), where missed doses or inconsistent refills could disrupt treatment progress.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Clinicians cited many advantages to opioid use disorder medications, most notably their ability to reduce cravings and opioid use. They also cited disadvantages, however, including concerns that for buprenorphine and methadone, they may “create a long-term dependency”. Although explicit stigma was uncommon, some clinicians still framed medications for opioid use disorder as addictive or suggested it was not part of “true” recovery. These views conflict with clinical guidelines, which emphasize that physical dependence on prescribed medication is not synonymous with addiction. That said, some individuals in or seeking recovery do not want to take an agonist medication like buprenorphine or methadone at least, in part, because of worries like these mentioned by clinicians. The study did not assess whether clinicians were in recovery, themselves, however. Shared decision-making models, where clinicians and patients collaborate on treatment choices, could enhance engagement and improve outcomes by ensuring patients receive balanced, evidence-based information about their options.
Finally, compared to buprenorphine and methadone, clinicians had fewer overall opinions about naltrexone, indicating lower familiarity and adoption. This is likely due to its more recent FDA approval (2010) and limited availability, both locally and nationally. Some research suggests naltrexone faces less stigma than other medications for opioid use disorder options, but if clinicians are unfamiliar with it, they may be less likely to present it as a treatment option.
The study aimed to capture a broad range of perspectives, but some distinctions between advantages and disadvantages may be blurred, as what is beneficial for one patient may be a challenge for another, depending on their stage in recovery.
The survey did not explicitly consider how medications for opioid use disorder suitability varies across the recovery timeline, such as how structural supports may be helpful in early treatment but burdensome later.
Since there is no comprehensive registry of substance use disorder clinicians, recruitment relied on a convenience sample, and it is unclear whether non-responding clinicians differed significantly from those who participated.
Clinicians’ familiarity with medications for opioid use disorder varied across agencies, particularly regarding different formulations (oral, sublingual, injectable), which may have influenced their perceptions.
The study was conducted in a single urban area, and findings may not apply to regions where abstinence-based treatment is more common or where clinicians have less exposure to medications for opioid use disorder.
BOTTOM LINE
This research aimed to understand how non-prescribing substance use disorder clinicians perceive and present medications for opioid use disorder to their patients. Clinicians cited many of the benefits of medications for opioid use disorder in reducing cravings and supporting recovery. Their primary concern regarding long-term dependency is not consistent with clinical guidelines but echoes worries from some patients. These insights underscore the need for targeted education and standardized training to ensure that patients receive evidence-based information, to help them make informed decisions about the opioid use disorder care they receive.
For individuals and families seeking recovery: Therapists you work with are likely to have their own views about opioid use disorder medications, including perceived advantages and disadvantages. It may be helpful to ask about the science regarding these medications so that you can make an informed decision based on your treatment goals and needs.
For treatment professionals and treatment systems: Treatment professionals and systems play a crucial role in ensuring that the benefit to risk ratio regarding medications for opioid use disorder are presented accurately and without stigma, helping patients make informed decisions based on the latest evidence. Training and education may help to address misconceptions regarding differences between long-term dependence and addiction. Incorporating shared decision-making models and person-centered care approaches may further enhance patient experiences and strengthen the overall impact of medications for opioid use disorder programs.
For scientists: Recovery scientists may benefit from exploring how clinician beliefs and training shape regarding medications for opioid use disorder influence patient uptake, helping to bridge gaps between research and treatment practices. Further research on the effectiveness of education and stigma-reduction interventions for non-prescribing treatment professionals may help improve implementation.
For policy makers: Treatment professionals and systems play a crucial role in ensuring that the benefit to risk ratio regarding medications for opioid use disorder are presented accurately and without stigma, helping patients make informed decisions based on the latest evidence. Training and education may help to address misconceptions regarding differences between long-term dependence and addiction. Funding for clinician education may help ensure any personal perspectives on medications for opioid use disorder do not affect the information they provide to patients.
Fewer than a third of individuals with opioid use disorder or active opioid use take an FDA-approved medication like buprenorphine (often prescribed in formulation with naloxone known by the brand name Suboxone). Additionally, many who start medications for opioid use disorder discontinue within weeks.
Research indicates that attitudes and beliefs about medications for opioid use disorder strongly influence treatment acceptance and adherence. Negative perceptions can lead to shame and guilt, a form of stigma known as “intervention stigma,” which discourages continued use. Thus, these attitudes play a crucial, albeit indirect, role on the ultimate public health impact of medications for opioid use disorder. As primary points of contact for patients, therapists and other clinical staff play an important role in shaping perceptions of and access to medications for opioid use disorder. Their attitudes and beliefs can influence whether individuals feel encouraged or discouraged from initiating and maintaining these life-saving treatments.
This study characterized therapist attitudes toward each of the 3 FDA approved medications for opioid use disorder. Because they may have different attitudes toward agonist medications methadone and buprenorphine compared to the antagonist medication naltrexone (often prescribed as a monthly injection known by the brand name Vivitrol), the study assessed therapist perceptions of the advantages and disadvantages of each medication separately.
HOW WAS THIS STUDY CONDUCTED?
From June to December 2021, the research team used free-response questions to survey clinical staff at publicly funded substance use disorder treatment agencies who serve Medicaid recipients in Philadelphia operating under a municipality-wide mandate to offer medications for opioid use disorder. The goal was to understand how they view the benefits and drawbacks of 3 medications for opioid use disorder options: buprenorphine, methadone, and naltrexone.
A total of 271 counselors answered an open-ended question for each medication: “When discussing [medication name] with your patient, what would be the most important advantage and disadvantage to mention?” Their responses were then analyzed to identify recurring themes.
The research team used thematic analysis to characterize perceived advantages and disadvantages. The average clinician was 43 years old, with approximately 11 years of professional experience and nearly five years in their current role. The majority of respondents (71%) identified as women, while 27% identified as men, and 2% did not report their gender. Most staff had a college education, with 88% holding at least a bachelor’s degree and 61% having a master’s degree or higher. Regarding racial and ethnic backgrounds, 51% identified as White, 37% as Black, 3% as Asian/Pacific Islander, 0.4% as Native American, and 7% as another race. Additionally, 7% identified as Hispanic or Latino. Clinicians worked in agencies with varying levels of access to medications for opioid use disorder. The majority (73%) were at agencies that provided buprenorphine, and 82% were at agencies offering naltrexone. The most commonly prescribed form of naltrexone is the extended-release version, known also by the brand name Vivitrol, though this study does not specify the naltrexone formulation. Just less than half worked at agencies that prescribed or dispensed methadone, highlighting a gap in its availability.
WHAT DID THIS STUDY FIND?
Staff felt medications offered unique benefits based on patient needs
One of the most frequently cited benefits of medications for opioid use disorder generally was its ability to reduce opioid cravings, with 42% of clinicians emphasizing this advantage. The Figure below shows the proportion of staff citing advantages by medication type. Similarly, 37% of clinicians highlighted its role in decreasing illicit opioid use, helping patients transition away from unregulated substances. Convenience was another key factor, with 25% of clinicians identifying flexibility in treatment as a major benefit, particularly for medications with less rigid dosing schedules. Additionally, 20% of clinicians emphasized that medications for opioid use disorder support a stable recovery lifestyle, enabling patients to develop long-term habits that reinforce recovery. Lastly, 17% of clinicians recognized the ability of medications for opioid use disorder to ease withdrawal symptoms, though the degree of relief varied depending on the specific medication.
Staff also felt medications had several disadvantages
One of the most frequently cited concerns about medications for opioid use disorder was the risk of long-term dependency, with 30% of clinicians expressing this issue, particularly for buprenorphine and methadone. The figure below shows the proportion of staff citing disadvantages by medication type. Side effects were another major drawback, reported by 28% of clinicians, with each medication presenting different physical challenges for patients. Treatment inconvenience was also a significant barrier, highlighted by 27% of clinicians, especially for medications requiring frequent clinic visits or strict adherence to dosing schedules. Additionally, 17% of clinicians raised concerns about misuse and diversion, particularly for buprenorphine (9%) and methadone (11%), citing issues such as selling, mixing with other substances, or improper use. Lastly, 16% of clinicians identified medication adherence and maintenance as a challenge, particularly for buprenorphine (11%), where missed doses or inconsistent refills could disrupt treatment progress.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Clinicians cited many advantages to opioid use disorder medications, most notably their ability to reduce cravings and opioid use. They also cited disadvantages, however, including concerns that for buprenorphine and methadone, they may “create a long-term dependency”. Although explicit stigma was uncommon, some clinicians still framed medications for opioid use disorder as addictive or suggested it was not part of “true” recovery. These views conflict with clinical guidelines, which emphasize that physical dependence on prescribed medication is not synonymous with addiction. That said, some individuals in or seeking recovery do not want to take an agonist medication like buprenorphine or methadone at least, in part, because of worries like these mentioned by clinicians. The study did not assess whether clinicians were in recovery, themselves, however. Shared decision-making models, where clinicians and patients collaborate on treatment choices, could enhance engagement and improve outcomes by ensuring patients receive balanced, evidence-based information about their options.
Finally, compared to buprenorphine and methadone, clinicians had fewer overall opinions about naltrexone, indicating lower familiarity and adoption. This is likely due to its more recent FDA approval (2010) and limited availability, both locally and nationally. Some research suggests naltrexone faces less stigma than other medications for opioid use disorder options, but if clinicians are unfamiliar with it, they may be less likely to present it as a treatment option.
The study aimed to capture a broad range of perspectives, but some distinctions between advantages and disadvantages may be blurred, as what is beneficial for one patient may be a challenge for another, depending on their stage in recovery.
The survey did not explicitly consider how medications for opioid use disorder suitability varies across the recovery timeline, such as how structural supports may be helpful in early treatment but burdensome later.
Since there is no comprehensive registry of substance use disorder clinicians, recruitment relied on a convenience sample, and it is unclear whether non-responding clinicians differed significantly from those who participated.
Clinicians’ familiarity with medications for opioid use disorder varied across agencies, particularly regarding different formulations (oral, sublingual, injectable), which may have influenced their perceptions.
The study was conducted in a single urban area, and findings may not apply to regions where abstinence-based treatment is more common or where clinicians have less exposure to medications for opioid use disorder.
BOTTOM LINE
This research aimed to understand how non-prescribing substance use disorder clinicians perceive and present medications for opioid use disorder to their patients. Clinicians cited many of the benefits of medications for opioid use disorder in reducing cravings and supporting recovery. Their primary concern regarding long-term dependency is not consistent with clinical guidelines but echoes worries from some patients. These insights underscore the need for targeted education and standardized training to ensure that patients receive evidence-based information, to help them make informed decisions about the opioid use disorder care they receive.
For individuals and families seeking recovery: Therapists you work with are likely to have their own views about opioid use disorder medications, including perceived advantages and disadvantages. It may be helpful to ask about the science regarding these medications so that you can make an informed decision based on your treatment goals and needs.
For treatment professionals and treatment systems: Treatment professionals and systems play a crucial role in ensuring that the benefit to risk ratio regarding medications for opioid use disorder are presented accurately and without stigma, helping patients make informed decisions based on the latest evidence. Training and education may help to address misconceptions regarding differences between long-term dependence and addiction. Incorporating shared decision-making models and person-centered care approaches may further enhance patient experiences and strengthen the overall impact of medications for opioid use disorder programs.
For scientists: Recovery scientists may benefit from exploring how clinician beliefs and training shape regarding medications for opioid use disorder influence patient uptake, helping to bridge gaps between research and treatment practices. Further research on the effectiveness of education and stigma-reduction interventions for non-prescribing treatment professionals may help improve implementation.
For policy makers: Treatment professionals and systems play a crucial role in ensuring that the benefit to risk ratio regarding medications for opioid use disorder are presented accurately and without stigma, helping patients make informed decisions based on the latest evidence. Training and education may help to address misconceptions regarding differences between long-term dependence and addiction. Funding for clinician education may help ensure any personal perspectives on medications for opioid use disorder do not affect the information they provide to patients.
Fewer than a third of individuals with opioid use disorder or active opioid use take an FDA-approved medication like buprenorphine (often prescribed in formulation with naloxone known by the brand name Suboxone). Additionally, many who start medications for opioid use disorder discontinue within weeks.
Research indicates that attitudes and beliefs about medications for opioid use disorder strongly influence treatment acceptance and adherence. Negative perceptions can lead to shame and guilt, a form of stigma known as “intervention stigma,” which discourages continued use. Thus, these attitudes play a crucial, albeit indirect, role on the ultimate public health impact of medications for opioid use disorder. As primary points of contact for patients, therapists and other clinical staff play an important role in shaping perceptions of and access to medications for opioid use disorder. Their attitudes and beliefs can influence whether individuals feel encouraged or discouraged from initiating and maintaining these life-saving treatments.
This study characterized therapist attitudes toward each of the 3 FDA approved medications for opioid use disorder. Because they may have different attitudes toward agonist medications methadone and buprenorphine compared to the antagonist medication naltrexone (often prescribed as a monthly injection known by the brand name Vivitrol), the study assessed therapist perceptions of the advantages and disadvantages of each medication separately.
HOW WAS THIS STUDY CONDUCTED?
From June to December 2021, the research team used free-response questions to survey clinical staff at publicly funded substance use disorder treatment agencies who serve Medicaid recipients in Philadelphia operating under a municipality-wide mandate to offer medications for opioid use disorder. The goal was to understand how they view the benefits and drawbacks of 3 medications for opioid use disorder options: buprenorphine, methadone, and naltrexone.
A total of 271 counselors answered an open-ended question for each medication: “When discussing [medication name] with your patient, what would be the most important advantage and disadvantage to mention?” Their responses were then analyzed to identify recurring themes.
The research team used thematic analysis to characterize perceived advantages and disadvantages. The average clinician was 43 years old, with approximately 11 years of professional experience and nearly five years in their current role. The majority of respondents (71%) identified as women, while 27% identified as men, and 2% did not report their gender. Most staff had a college education, with 88% holding at least a bachelor’s degree and 61% having a master’s degree or higher. Regarding racial and ethnic backgrounds, 51% identified as White, 37% as Black, 3% as Asian/Pacific Islander, 0.4% as Native American, and 7% as another race. Additionally, 7% identified as Hispanic or Latino. Clinicians worked in agencies with varying levels of access to medications for opioid use disorder. The majority (73%) were at agencies that provided buprenorphine, and 82% were at agencies offering naltrexone. The most commonly prescribed form of naltrexone is the extended-release version, known also by the brand name Vivitrol, though this study does not specify the naltrexone formulation. Just less than half worked at agencies that prescribed or dispensed methadone, highlighting a gap in its availability.
WHAT DID THIS STUDY FIND?
Staff felt medications offered unique benefits based on patient needs
One of the most frequently cited benefits of medications for opioid use disorder generally was its ability to reduce opioid cravings, with 42% of clinicians emphasizing this advantage. The Figure below shows the proportion of staff citing advantages by medication type. Similarly, 37% of clinicians highlighted its role in decreasing illicit opioid use, helping patients transition away from unregulated substances. Convenience was another key factor, with 25% of clinicians identifying flexibility in treatment as a major benefit, particularly for medications with less rigid dosing schedules. Additionally, 20% of clinicians emphasized that medications for opioid use disorder support a stable recovery lifestyle, enabling patients to develop long-term habits that reinforce recovery. Lastly, 17% of clinicians recognized the ability of medications for opioid use disorder to ease withdrawal symptoms, though the degree of relief varied depending on the specific medication.
Staff also felt medications had several disadvantages
One of the most frequently cited concerns about medications for opioid use disorder was the risk of long-term dependency, with 30% of clinicians expressing this issue, particularly for buprenorphine and methadone. The figure below shows the proportion of staff citing disadvantages by medication type. Side effects were another major drawback, reported by 28% of clinicians, with each medication presenting different physical challenges for patients. Treatment inconvenience was also a significant barrier, highlighted by 27% of clinicians, especially for medications requiring frequent clinic visits or strict adherence to dosing schedules. Additionally, 17% of clinicians raised concerns about misuse and diversion, particularly for buprenorphine (9%) and methadone (11%), citing issues such as selling, mixing with other substances, or improper use. Lastly, 16% of clinicians identified medication adherence and maintenance as a challenge, particularly for buprenorphine (11%), where missed doses or inconsistent refills could disrupt treatment progress.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Clinicians cited many advantages to opioid use disorder medications, most notably their ability to reduce cravings and opioid use. They also cited disadvantages, however, including concerns that for buprenorphine and methadone, they may “create a long-term dependency”. Although explicit stigma was uncommon, some clinicians still framed medications for opioid use disorder as addictive or suggested it was not part of “true” recovery. These views conflict with clinical guidelines, which emphasize that physical dependence on prescribed medication is not synonymous with addiction. That said, some individuals in or seeking recovery do not want to take an agonist medication like buprenorphine or methadone at least, in part, because of worries like these mentioned by clinicians. The study did not assess whether clinicians were in recovery, themselves, however. Shared decision-making models, where clinicians and patients collaborate on treatment choices, could enhance engagement and improve outcomes by ensuring patients receive balanced, evidence-based information about their options.
Finally, compared to buprenorphine and methadone, clinicians had fewer overall opinions about naltrexone, indicating lower familiarity and adoption. This is likely due to its more recent FDA approval (2010) and limited availability, both locally and nationally. Some research suggests naltrexone faces less stigma than other medications for opioid use disorder options, but if clinicians are unfamiliar with it, they may be less likely to present it as a treatment option.
The study aimed to capture a broad range of perspectives, but some distinctions between advantages and disadvantages may be blurred, as what is beneficial for one patient may be a challenge for another, depending on their stage in recovery.
The survey did not explicitly consider how medications for opioid use disorder suitability varies across the recovery timeline, such as how structural supports may be helpful in early treatment but burdensome later.
Since there is no comprehensive registry of substance use disorder clinicians, recruitment relied on a convenience sample, and it is unclear whether non-responding clinicians differed significantly from those who participated.
Clinicians’ familiarity with medications for opioid use disorder varied across agencies, particularly regarding different formulations (oral, sublingual, injectable), which may have influenced their perceptions.
The study was conducted in a single urban area, and findings may not apply to regions where abstinence-based treatment is more common or where clinicians have less exposure to medications for opioid use disorder.
BOTTOM LINE
This research aimed to understand how non-prescribing substance use disorder clinicians perceive and present medications for opioid use disorder to their patients. Clinicians cited many of the benefits of medications for opioid use disorder in reducing cravings and supporting recovery. Their primary concern regarding long-term dependency is not consistent with clinical guidelines but echoes worries from some patients. These insights underscore the need for targeted education and standardized training to ensure that patients receive evidence-based information, to help them make informed decisions about the opioid use disorder care they receive.
For individuals and families seeking recovery: Therapists you work with are likely to have their own views about opioid use disorder medications, including perceived advantages and disadvantages. It may be helpful to ask about the science regarding these medications so that you can make an informed decision based on your treatment goals and needs.
For treatment professionals and treatment systems: Treatment professionals and systems play a crucial role in ensuring that the benefit to risk ratio regarding medications for opioid use disorder are presented accurately and without stigma, helping patients make informed decisions based on the latest evidence. Training and education may help to address misconceptions regarding differences between long-term dependence and addiction. Incorporating shared decision-making models and person-centered care approaches may further enhance patient experiences and strengthen the overall impact of medications for opioid use disorder programs.
For scientists: Recovery scientists may benefit from exploring how clinician beliefs and training shape regarding medications for opioid use disorder influence patient uptake, helping to bridge gaps between research and treatment practices. Further research on the effectiveness of education and stigma-reduction interventions for non-prescribing treatment professionals may help improve implementation.
For policy makers: Treatment professionals and systems play a crucial role in ensuring that the benefit to risk ratio regarding medications for opioid use disorder are presented accurately and without stigma, helping patients make informed decisions based on the latest evidence. Training and education may help to address misconceptions regarding differences between long-term dependence and addiction. Funding for clinician education may help ensure any personal perspectives on medications for opioid use disorder do not affect the information they provide to patients.