Can a weight loss medication help with cocaine use disorder?
There are no medications approved by the Food and Drug Administration (FDA) for cocaine use disorder, despite many rigorous clinical trials testing candidates shown initially to be promising. This study tested lorcaserin, a medication that was previously approved to treat obesity, in trial for cocaine use disorder.
Cocaine is a fast acting stimulant known for its high addictive potential. Although the Food and Drug Administration has classified cocaine as a Schedule II drug, meaning that there are some known medical uses, cocaine has a high addictive potential and regular use is typically accompanied by severe consequences. Cocaine use disorder affects an estimated 1.4 million people over the age of 12 in the United States population, with slightly higher prevalence among adults aged 18 to 25 (0.8%) compared to adolescents aged 12 to 17 (0.05%) and adults over the age of 25 (0.5%). Though cocaine withdrawal is typically non-fatal, acute and recurrent cocaine use increases risk for all-cause mortality, and there have been increases in cocaine exposures and cocaine-related mortality in recent years.
Despite decades of research and many rigorous clinical trials, there are currently no FDA-approved pharmacological treatments for cocaine use disorder. Medications for stimulant use disorder in general have been less effective, in contrast to positive public health benefits of medication development for other substance use disorders such as opioid or alcohol use disorder. Given the lack of available effective treatment for cocaine use disorder and the rising rates of mortality, there is a pressing need for effective medication development.
One potential medication candidate is lorcaserin, which is a serotonin agonist that primarily operates in the hypothalamus, affecting appetite. Preclinical studies have also found that lorcaserin may reduce activity in the part of the brain affected by drugs with addictive potential known as the mesolimbic dopamine projection, which is associated with the experience of reward. Further, initial studies using animal models demonstrated that lorcaserin reduced cocaine intake. As a result, lorcaserin has been hypothesized as a candidate medication for cocaine use disorder.
Importantly, lorcaserin was previously FDA approved for weight loss, though discontinued in 2020 due to evidence of slightly increased cancer risk compared to placebo in a longer-term trial, making the risk to benefit ratio no longer favorable, and it was pulled from the market. However, several studies had already tested the medication for cocaine use disorder before the FDA requested its removal from the market in 2020. One such study evaluated whether lorcaserin was effective at reducing cocaine use, craving, and consequences in a sample of human adults with cocaine use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a double-blind randomized controlled trial testing the efficacy of lorcaserin as a medication for cocaine use disorder. Researchers enrolled 272 treatment-seeking adults between the ages of 18 and 65 who met DSM-5 criteria for cocaine use disorder at any level of severity (mild, moderate, and severe). Participants were required to be capable of understanding study procedures, report recent cocaine use (past 30 days), and have a body mass index greater than 20. There was a list of reasons people were excluded as is typical in clinical trials to give the medication the best chance of success (e.g., current opioid use disorder and other psychiatric disorders known to have severe impacts on functioning like psychotic disorder, etc.). Participants were recruited from addiction treatment centers, academic medical center clinics, and contract research sites. After screening and enrollment, participants completed one week of twice daily 15 mg acetazolamide, which is similar in appearance to lorcaserin and was used as a marker of medication adherence. After week 1, participants were randomized to receive either twice daily 10 mg lorcaserin or placebo capsules (double-blind) for the remaining 12 weeks and visited the clinic for a final measurement visit two weeks later. The primary outcome was abstinence (see below for more details on determination of abstinence); the researchers also measured cocaine craving and consequences as secondary outcomes.
All participants in both randomized conditions also participated in weekly 1-hour individual sessions of manualized cognitive behavioral therapy. To increase adherence, participants took medications while engaging with a mobile app that “confirmed the ingestion of study medications” using “facial recognition and motion-sensing technology” and clinical staff reviewed any adherence lapses with patients. In addition to this strategy to increase adherence, the study also examined outcomes separately for those with 8 or more days of cocaine use during the 30 days prior to screening and who had high levels of the adherence marker medication acetazolamide level at Study Day 8 to determine whether the medication was effective in the most medication adherent population.
The primary outcome, abstinence during the last 3 weeks of treatment, was determined based on the following criteria: (1) self-report data indicating no cocaine use during the full 3-week period; (2) at least one bioassay testing for benzoylecgonine, a metabolite of cocaine, within the 3-week period; and 3) negative bioassay results for all samples collected during the 3-week period. If one of these criteria are not met, the individual was deemed to have not met criteria for abstinence for this clinical trial. Participants also engaged in a 1-week medication adherence trial in which they took twice daily 15 mg doses of acetazolamide. In addition to abstinence, the researchers measured changes in craving and problems related to drug use over the study period. The researchers also asked participants whether they were attempting abstinence from alcohol during the course of the study period and the randomization was weighted based on whether alcohol abstinence was a treatment goal so that the treatment groups would contain similar numbers of individuals with an alcohol abstinence treatment goal.
During the first week, 30 participants either withdrew from study participation or excluded prior to randomization. The study sample was 72% male, 50.2 years of age on average, 66% Black 27% White, and 7.4% Hispanic. Smoking was the most common route of cocaine administration (76%) followed by nasal administration (23%). Virtually all (95%) of the sample meeting criteria for moderate (14%) and severe cocaine use disorder (81%), respectively.
WHAT DID THIS STUDY FIND?
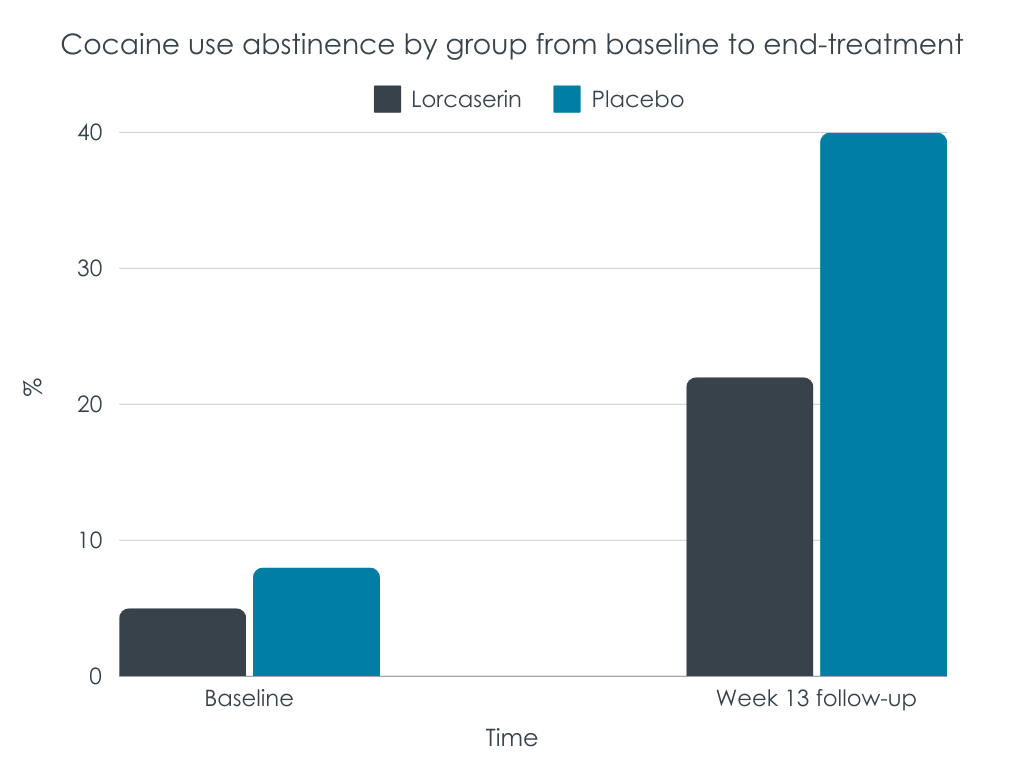
There were no differences in primary outcome
There were no differences in abstinence across groups for the full sample or efficacy population analyses. Within the efficacy population, only 1.1% of the lorcaserin group, and 4.3% of the placebo group, were abstinent during the last 3 weeks of treatment. In the full sample of all randomized participants, 2.5% and 5.6% of the lorcaserin and placebo groups, respectively, were abstinent during the last 3 weeks of treatment. Among those also attempting alcohol abstinence or who were abstinent to start the trial, 6.7% in the placebo group and 0% of the lorcarserin group were abstinent from cocaine in the last 3 weeks of treatment. Over the full course of the study, the number of positive urine tests decreased for both groups with no group differences. At baseline, 87% and 88% of participants had positive cocaine screens in the lorcaserin and placebo conditions, respectively. At week 13, 73% and 72% of participants had positive cocaine screens in the lorcaserin and placebo conditions, respectively.
There were no differences on secondary outcomes, either
In the most adherent group of participants, both the lorcaserin and placebo groups demonstrated comparable decreases in craving from baseline to 13 weeks (-3.4 and -3.5, respectively; Scale, 0-80). There group differences observed on decreases in drug and alcohol-related problems were in the opposite direction as that hypothesized: they favored the placebo group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research did not find support for lorcaserin as an effective medication for cocaine use disorder, and in some cases, the placebo condition appeared to outperform the medication condition. It is also important to reiterate that this study and others testing lorcaserin for cocaine use disorder were, by all accounts, completed before the Food and Drug administration revoked approval of the medication for weight loss due to high cancer risk. The failed clinical trial in context of it having been already pulled from the market in February 2020 highlights the intractability of lorcaserin as a potential therapeutic for cocaine use disorder.
The finding that lorcaserin is not efficacious at reducing cocaine use is consistent with decades of medications trials failing to show benefits for stimulant use disorder generally and cocaine use disorder in particular. Other medications and medication classes that have been tested yet lack efficacy at treating cocaine use disorder include cannabidiol, Vigabatrin, various antipsychotics, anticonvulsants, antidepressants, dopamine agonists, opioids, and other psychostimulants. There are other medications that are under consideration as medications for cocaine use disorder, including Ketamine. Novel directions in medication development for cocaine use disorder has shifted toward targeting multiple neurobiological mechanisms, with the hope that more comprehensive coverage may be associated with greater efficacy. For example, drug combinations are being considered, with some evidence that buprenorphine, naloxone, and naltrexone may work in combination to enhance cocaine abstinence.
Although it is important to continue medication development, it is important to highlight that medications are not the only option. Contingency management, which is a broadly defined collection of programs that systematically use incentives to reward (i.e., positively reinforce) cocaine abstinence (e.g., by providing monetary vouchers to patients for testing negative for cocaine use via urinalysis), has consistently demonstrated efficacy at treating cocaine use disorder. Increasing access to contingency management may improve public health management of cocaine use disorder. At the same time, the benefits of contingency management may quickly fade once the protocol of systematic rewards are removed. Therefore, it is also important that psychosocial interventions based on 12-step facilitation approaches have also been shown to improve cocaine use outcomes. These treatments actively link patients with community-based 12-step mutual-help organizations, which can be accessed for free over the long term, while providing recovery psychoeducation and helping them to develop skills to initiate and maintain abstinence.
There also have been acknowledgements of alternative efficacy outcomes in medication development. Abstinence is the traditional outcome in medications trials and is the outcome with the greatest overall positive health impact. However, other harm reduction targets such as reductions in substance use are increasingly considered and may still result in increases in psychosocial functioning and quality of life. Prior research has demonstrated that medications such as Topiramate may be considered efficacious using goals other than full abstinence, and may help individuals develop efficacy toward recovery and reduce harms in the interim.
The sample did not include those with a diagnosis of another substance use disorder, which are common among people with cocaine use disorder. Thus, the sample may represent a relatively small portion of those with cocaine use disorder, and results may not generalize.
BOTTOM LINE
In this well controlled randomized study testing whether lorcaserin reduced cocaine use, craving, and consequences, lorcaserin did not appear to be helpful in addressing cocaine use disorder.
For individuals and families seeking recovery: Although there are no FDA-approved medications for cocaine use disorder, contingency management has been shown to be helpful at increasing abstinence in dozens of studies. It is also important to mention that scientists continue to explore other medication options, with some emerging as potential therapeutics that will be tested in further clinical trials.
For treatment professionals and treatment systems: To date, scientists have been unable to develop an effective medication for cocaine use disorder. However, contingency management is helpful at increasing cocaine abstinence. Consider requesting or attending a training hosted by SAMHSA on contingency management (see www.opioidresponsenetwork.org) or referring patients to treatment providers and treatments centers that use this approach.
For scientists: Preclinical studies using drug choice procedures have typically been predictive of failed medication trials; however, these paradigms are not always used in preclinical trials. Studies using drug-choice procedures may be more likely to accurately detect translation to therapeutics in medications trials. Additionally, novel neurobiological approaches, such as targeting multiple mechanisms, may be the most effective way to identify an efficacious medication for cocaine use disorder. Finally, research on the contextual factors associated with return to cocaine use during treatment and recovery, may identify novel targets to improve recovery outcomes for this population.
For policy makers: Although there is not an FDA-approved medication for cocaine use disorder, continued research may eventually help uncover a novel therapeutic that will become an essential tool in the treatment of cocaine use disorder. For this reason, medication development funding to treat cocaine use disorder remains a priority. However, contingency management has demonstrated efficacy for reducing cocaine use disorder. Increasing the availability of contingency management, including through insurance reimbursement, would likely improve public health response to cocaine use disorder. Alternative targets for medications development may also prove to reduce overall harm, such as reduction of cocaine consumption rather than full abstinence.
Cocaine is a fast acting stimulant known for its high addictive potential. Although the Food and Drug Administration has classified cocaine as a Schedule II drug, meaning that there are some known medical uses, cocaine has a high addictive potential and regular use is typically accompanied by severe consequences. Cocaine use disorder affects an estimated 1.4 million people over the age of 12 in the United States population, with slightly higher prevalence among adults aged 18 to 25 (0.8%) compared to adolescents aged 12 to 17 (0.05%) and adults over the age of 25 (0.5%). Though cocaine withdrawal is typically non-fatal, acute and recurrent cocaine use increases risk for all-cause mortality, and there have been increases in cocaine exposures and cocaine-related mortality in recent years.
Despite decades of research and many rigorous clinical trials, there are currently no FDA-approved pharmacological treatments for cocaine use disorder. Medications for stimulant use disorder in general have been less effective, in contrast to positive public health benefits of medication development for other substance use disorders such as opioid or alcohol use disorder. Given the lack of available effective treatment for cocaine use disorder and the rising rates of mortality, there is a pressing need for effective medication development.
One potential medication candidate is lorcaserin, which is a serotonin agonist that primarily operates in the hypothalamus, affecting appetite. Preclinical studies have also found that lorcaserin may reduce activity in the part of the brain affected by drugs with addictive potential known as the mesolimbic dopamine projection, which is associated with the experience of reward. Further, initial studies using animal models demonstrated that lorcaserin reduced cocaine intake. As a result, lorcaserin has been hypothesized as a candidate medication for cocaine use disorder.
Importantly, lorcaserin was previously FDA approved for weight loss, though discontinued in 2020 due to evidence of slightly increased cancer risk compared to placebo in a longer-term trial, making the risk to benefit ratio no longer favorable, and it was pulled from the market. However, several studies had already tested the medication for cocaine use disorder before the FDA requested its removal from the market in 2020. One such study evaluated whether lorcaserin was effective at reducing cocaine use, craving, and consequences in a sample of human adults with cocaine use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a double-blind randomized controlled trial testing the efficacy of lorcaserin as a medication for cocaine use disorder. Researchers enrolled 272 treatment-seeking adults between the ages of 18 and 65 who met DSM-5 criteria for cocaine use disorder at any level of severity (mild, moderate, and severe). Participants were required to be capable of understanding study procedures, report recent cocaine use (past 30 days), and have a body mass index greater than 20. There was a list of reasons people were excluded as is typical in clinical trials to give the medication the best chance of success (e.g., current opioid use disorder and other psychiatric disorders known to have severe impacts on functioning like psychotic disorder, etc.). Participants were recruited from addiction treatment centers, academic medical center clinics, and contract research sites. After screening and enrollment, participants completed one week of twice daily 15 mg acetazolamide, which is similar in appearance to lorcaserin and was used as a marker of medication adherence. After week 1, participants were randomized to receive either twice daily 10 mg lorcaserin or placebo capsules (double-blind) for the remaining 12 weeks and visited the clinic for a final measurement visit two weeks later. The primary outcome was abstinence (see below for more details on determination of abstinence); the researchers also measured cocaine craving and consequences as secondary outcomes.
All participants in both randomized conditions also participated in weekly 1-hour individual sessions of manualized cognitive behavioral therapy. To increase adherence, participants took medications while engaging with a mobile app that “confirmed the ingestion of study medications” using “facial recognition and motion-sensing technology” and clinical staff reviewed any adherence lapses with patients. In addition to this strategy to increase adherence, the study also examined outcomes separately for those with 8 or more days of cocaine use during the 30 days prior to screening and who had high levels of the adherence marker medication acetazolamide level at Study Day 8 to determine whether the medication was effective in the most medication adherent population.
The primary outcome, abstinence during the last 3 weeks of treatment, was determined based on the following criteria: (1) self-report data indicating no cocaine use during the full 3-week period; (2) at least one bioassay testing for benzoylecgonine, a metabolite of cocaine, within the 3-week period; and 3) negative bioassay results for all samples collected during the 3-week period. If one of these criteria are not met, the individual was deemed to have not met criteria for abstinence for this clinical trial. Participants also engaged in a 1-week medication adherence trial in which they took twice daily 15 mg doses of acetazolamide. In addition to abstinence, the researchers measured changes in craving and problems related to drug use over the study period. The researchers also asked participants whether they were attempting abstinence from alcohol during the course of the study period and the randomization was weighted based on whether alcohol abstinence was a treatment goal so that the treatment groups would contain similar numbers of individuals with an alcohol abstinence treatment goal.
During the first week, 30 participants either withdrew from study participation or excluded prior to randomization. The study sample was 72% male, 50.2 years of age on average, 66% Black 27% White, and 7.4% Hispanic. Smoking was the most common route of cocaine administration (76%) followed by nasal administration (23%). Virtually all (95%) of the sample meeting criteria for moderate (14%) and severe cocaine use disorder (81%), respectively.
WHAT DID THIS STUDY FIND?
There were no differences in primary outcome
There were no differences in abstinence across groups for the full sample or efficacy population analyses. Within the efficacy population, only 1.1% of the lorcaserin group, and 4.3% of the placebo group, were abstinent during the last 3 weeks of treatment. In the full sample of all randomized participants, 2.5% and 5.6% of the lorcaserin and placebo groups, respectively, were abstinent during the last 3 weeks of treatment. Among those also attempting alcohol abstinence or who were abstinent to start the trial, 6.7% in the placebo group and 0% of the lorcarserin group were abstinent from cocaine in the last 3 weeks of treatment. Over the full course of the study, the number of positive urine tests decreased for both groups with no group differences. At baseline, 87% and 88% of participants had positive cocaine screens in the lorcaserin and placebo conditions, respectively. At week 13, 73% and 72% of participants had positive cocaine screens in the lorcaserin and placebo conditions, respectively.
There were no differences on secondary outcomes, either
In the most adherent group of participants, both the lorcaserin and placebo groups demonstrated comparable decreases in craving from baseline to 13 weeks (-3.4 and -3.5, respectively; Scale, 0-80). There group differences observed on decreases in drug and alcohol-related problems were in the opposite direction as that hypothesized: they favored the placebo group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research did not find support for lorcaserin as an effective medication for cocaine use disorder, and in some cases, the placebo condition appeared to outperform the medication condition. It is also important to reiterate that this study and others testing lorcaserin for cocaine use disorder were, by all accounts, completed before the Food and Drug administration revoked approval of the medication for weight loss due to high cancer risk. The failed clinical trial in context of it having been already pulled from the market in February 2020 highlights the intractability of lorcaserin as a potential therapeutic for cocaine use disorder.
The finding that lorcaserin is not efficacious at reducing cocaine use is consistent with decades of medications trials failing to show benefits for stimulant use disorder generally and cocaine use disorder in particular. Other medications and medication classes that have been tested yet lack efficacy at treating cocaine use disorder include cannabidiol, Vigabatrin, various antipsychotics, anticonvulsants, antidepressants, dopamine agonists, opioids, and other psychostimulants. There are other medications that are under consideration as medications for cocaine use disorder, including Ketamine. Novel directions in medication development for cocaine use disorder has shifted toward targeting multiple neurobiological mechanisms, with the hope that more comprehensive coverage may be associated with greater efficacy. For example, drug combinations are being considered, with some evidence that buprenorphine, naloxone, and naltrexone may work in combination to enhance cocaine abstinence.
Although it is important to continue medication development, it is important to highlight that medications are not the only option. Contingency management, which is a broadly defined collection of programs that systematically use incentives to reward (i.e., positively reinforce) cocaine abstinence (e.g., by providing monetary vouchers to patients for testing negative for cocaine use via urinalysis), has consistently demonstrated efficacy at treating cocaine use disorder. Increasing access to contingency management may improve public health management of cocaine use disorder. At the same time, the benefits of contingency management may quickly fade once the protocol of systematic rewards are removed. Therefore, it is also important that psychosocial interventions based on 12-step facilitation approaches have also been shown to improve cocaine use outcomes. These treatments actively link patients with community-based 12-step mutual-help organizations, which can be accessed for free over the long term, while providing recovery psychoeducation and helping them to develop skills to initiate and maintain abstinence.
There also have been acknowledgements of alternative efficacy outcomes in medication development. Abstinence is the traditional outcome in medications trials and is the outcome with the greatest overall positive health impact. However, other harm reduction targets such as reductions in substance use are increasingly considered and may still result in increases in psychosocial functioning and quality of life. Prior research has demonstrated that medications such as Topiramate may be considered efficacious using goals other than full abstinence, and may help individuals develop efficacy toward recovery and reduce harms in the interim.
The sample did not include those with a diagnosis of another substance use disorder, which are common among people with cocaine use disorder. Thus, the sample may represent a relatively small portion of those with cocaine use disorder, and results may not generalize.
BOTTOM LINE
In this well controlled randomized study testing whether lorcaserin reduced cocaine use, craving, and consequences, lorcaserin did not appear to be helpful in addressing cocaine use disorder.
For individuals and families seeking recovery: Although there are no FDA-approved medications for cocaine use disorder, contingency management has been shown to be helpful at increasing abstinence in dozens of studies. It is also important to mention that scientists continue to explore other medication options, with some emerging as potential therapeutics that will be tested in further clinical trials.
For treatment professionals and treatment systems: To date, scientists have been unable to develop an effective medication for cocaine use disorder. However, contingency management is helpful at increasing cocaine abstinence. Consider requesting or attending a training hosted by SAMHSA on contingency management (see www.opioidresponsenetwork.org) or referring patients to treatment providers and treatments centers that use this approach.
For scientists: Preclinical studies using drug choice procedures have typically been predictive of failed medication trials; however, these paradigms are not always used in preclinical trials. Studies using drug-choice procedures may be more likely to accurately detect translation to therapeutics in medications trials. Additionally, novel neurobiological approaches, such as targeting multiple mechanisms, may be the most effective way to identify an efficacious medication for cocaine use disorder. Finally, research on the contextual factors associated with return to cocaine use during treatment and recovery, may identify novel targets to improve recovery outcomes for this population.
For policy makers: Although there is not an FDA-approved medication for cocaine use disorder, continued research may eventually help uncover a novel therapeutic that will become an essential tool in the treatment of cocaine use disorder. For this reason, medication development funding to treat cocaine use disorder remains a priority. However, contingency management has demonstrated efficacy for reducing cocaine use disorder. Increasing the availability of contingency management, including through insurance reimbursement, would likely improve public health response to cocaine use disorder. Alternative targets for medications development may also prove to reduce overall harm, such as reduction of cocaine consumption rather than full abstinence.
Cocaine is a fast acting stimulant known for its high addictive potential. Although the Food and Drug Administration has classified cocaine as a Schedule II drug, meaning that there are some known medical uses, cocaine has a high addictive potential and regular use is typically accompanied by severe consequences. Cocaine use disorder affects an estimated 1.4 million people over the age of 12 in the United States population, with slightly higher prevalence among adults aged 18 to 25 (0.8%) compared to adolescents aged 12 to 17 (0.05%) and adults over the age of 25 (0.5%). Though cocaine withdrawal is typically non-fatal, acute and recurrent cocaine use increases risk for all-cause mortality, and there have been increases in cocaine exposures and cocaine-related mortality in recent years.
Despite decades of research and many rigorous clinical trials, there are currently no FDA-approved pharmacological treatments for cocaine use disorder. Medications for stimulant use disorder in general have been less effective, in contrast to positive public health benefits of medication development for other substance use disorders such as opioid or alcohol use disorder. Given the lack of available effective treatment for cocaine use disorder and the rising rates of mortality, there is a pressing need for effective medication development.
One potential medication candidate is lorcaserin, which is a serotonin agonist that primarily operates in the hypothalamus, affecting appetite. Preclinical studies have also found that lorcaserin may reduce activity in the part of the brain affected by drugs with addictive potential known as the mesolimbic dopamine projection, which is associated with the experience of reward. Further, initial studies using animal models demonstrated that lorcaserin reduced cocaine intake. As a result, lorcaserin has been hypothesized as a candidate medication for cocaine use disorder.
Importantly, lorcaserin was previously FDA approved for weight loss, though discontinued in 2020 due to evidence of slightly increased cancer risk compared to placebo in a longer-term trial, making the risk to benefit ratio no longer favorable, and it was pulled from the market. However, several studies had already tested the medication for cocaine use disorder before the FDA requested its removal from the market in 2020. One such study evaluated whether lorcaserin was effective at reducing cocaine use, craving, and consequences in a sample of human adults with cocaine use disorder.
HOW WAS THIS STUDY CONDUCTED?
This was a double-blind randomized controlled trial testing the efficacy of lorcaserin as a medication for cocaine use disorder. Researchers enrolled 272 treatment-seeking adults between the ages of 18 and 65 who met DSM-5 criteria for cocaine use disorder at any level of severity (mild, moderate, and severe). Participants were required to be capable of understanding study procedures, report recent cocaine use (past 30 days), and have a body mass index greater than 20. There was a list of reasons people were excluded as is typical in clinical trials to give the medication the best chance of success (e.g., current opioid use disorder and other psychiatric disorders known to have severe impacts on functioning like psychotic disorder, etc.). Participants were recruited from addiction treatment centers, academic medical center clinics, and contract research sites. After screening and enrollment, participants completed one week of twice daily 15 mg acetazolamide, which is similar in appearance to lorcaserin and was used as a marker of medication adherence. After week 1, participants were randomized to receive either twice daily 10 mg lorcaserin or placebo capsules (double-blind) for the remaining 12 weeks and visited the clinic for a final measurement visit two weeks later. The primary outcome was abstinence (see below for more details on determination of abstinence); the researchers also measured cocaine craving and consequences as secondary outcomes.
All participants in both randomized conditions also participated in weekly 1-hour individual sessions of manualized cognitive behavioral therapy. To increase adherence, participants took medications while engaging with a mobile app that “confirmed the ingestion of study medications” using “facial recognition and motion-sensing technology” and clinical staff reviewed any adherence lapses with patients. In addition to this strategy to increase adherence, the study also examined outcomes separately for those with 8 or more days of cocaine use during the 30 days prior to screening and who had high levels of the adherence marker medication acetazolamide level at Study Day 8 to determine whether the medication was effective in the most medication adherent population.
The primary outcome, abstinence during the last 3 weeks of treatment, was determined based on the following criteria: (1) self-report data indicating no cocaine use during the full 3-week period; (2) at least one bioassay testing for benzoylecgonine, a metabolite of cocaine, within the 3-week period; and 3) negative bioassay results for all samples collected during the 3-week period. If one of these criteria are not met, the individual was deemed to have not met criteria for abstinence for this clinical trial. Participants also engaged in a 1-week medication adherence trial in which they took twice daily 15 mg doses of acetazolamide. In addition to abstinence, the researchers measured changes in craving and problems related to drug use over the study period. The researchers also asked participants whether they were attempting abstinence from alcohol during the course of the study period and the randomization was weighted based on whether alcohol abstinence was a treatment goal so that the treatment groups would contain similar numbers of individuals with an alcohol abstinence treatment goal.
During the first week, 30 participants either withdrew from study participation or excluded prior to randomization. The study sample was 72% male, 50.2 years of age on average, 66% Black 27% White, and 7.4% Hispanic. Smoking was the most common route of cocaine administration (76%) followed by nasal administration (23%). Virtually all (95%) of the sample meeting criteria for moderate (14%) and severe cocaine use disorder (81%), respectively.
WHAT DID THIS STUDY FIND?
There were no differences in primary outcome
There were no differences in abstinence across groups for the full sample or efficacy population analyses. Within the efficacy population, only 1.1% of the lorcaserin group, and 4.3% of the placebo group, were abstinent during the last 3 weeks of treatment. In the full sample of all randomized participants, 2.5% and 5.6% of the lorcaserin and placebo groups, respectively, were abstinent during the last 3 weeks of treatment. Among those also attempting alcohol abstinence or who were abstinent to start the trial, 6.7% in the placebo group and 0% of the lorcarserin group were abstinent from cocaine in the last 3 weeks of treatment. Over the full course of the study, the number of positive urine tests decreased for both groups with no group differences. At baseline, 87% and 88% of participants had positive cocaine screens in the lorcaserin and placebo conditions, respectively. At week 13, 73% and 72% of participants had positive cocaine screens in the lorcaserin and placebo conditions, respectively.
There were no differences on secondary outcomes, either
In the most adherent group of participants, both the lorcaserin and placebo groups demonstrated comparable decreases in craving from baseline to 13 weeks (-3.4 and -3.5, respectively; Scale, 0-80). There group differences observed on decreases in drug and alcohol-related problems were in the opposite direction as that hypothesized: they favored the placebo group.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research did not find support for lorcaserin as an effective medication for cocaine use disorder, and in some cases, the placebo condition appeared to outperform the medication condition. It is also important to reiterate that this study and others testing lorcaserin for cocaine use disorder were, by all accounts, completed before the Food and Drug administration revoked approval of the medication for weight loss due to high cancer risk. The failed clinical trial in context of it having been already pulled from the market in February 2020 highlights the intractability of lorcaserin as a potential therapeutic for cocaine use disorder.
The finding that lorcaserin is not efficacious at reducing cocaine use is consistent with decades of medications trials failing to show benefits for stimulant use disorder generally and cocaine use disorder in particular. Other medications and medication classes that have been tested yet lack efficacy at treating cocaine use disorder include cannabidiol, Vigabatrin, various antipsychotics, anticonvulsants, antidepressants, dopamine agonists, opioids, and other psychostimulants. There are other medications that are under consideration as medications for cocaine use disorder, including Ketamine. Novel directions in medication development for cocaine use disorder has shifted toward targeting multiple neurobiological mechanisms, with the hope that more comprehensive coverage may be associated with greater efficacy. For example, drug combinations are being considered, with some evidence that buprenorphine, naloxone, and naltrexone may work in combination to enhance cocaine abstinence.
Although it is important to continue medication development, it is important to highlight that medications are not the only option. Contingency management, which is a broadly defined collection of programs that systematically use incentives to reward (i.e., positively reinforce) cocaine abstinence (e.g., by providing monetary vouchers to patients for testing negative for cocaine use via urinalysis), has consistently demonstrated efficacy at treating cocaine use disorder. Increasing access to contingency management may improve public health management of cocaine use disorder. At the same time, the benefits of contingency management may quickly fade once the protocol of systematic rewards are removed. Therefore, it is also important that psychosocial interventions based on 12-step facilitation approaches have also been shown to improve cocaine use outcomes. These treatments actively link patients with community-based 12-step mutual-help organizations, which can be accessed for free over the long term, while providing recovery psychoeducation and helping them to develop skills to initiate and maintain abstinence.
There also have been acknowledgements of alternative efficacy outcomes in medication development. Abstinence is the traditional outcome in medications trials and is the outcome with the greatest overall positive health impact. However, other harm reduction targets such as reductions in substance use are increasingly considered and may still result in increases in psychosocial functioning and quality of life. Prior research has demonstrated that medications such as Topiramate may be considered efficacious using goals other than full abstinence, and may help individuals develop efficacy toward recovery and reduce harms in the interim.
The sample did not include those with a diagnosis of another substance use disorder, which are common among people with cocaine use disorder. Thus, the sample may represent a relatively small portion of those with cocaine use disorder, and results may not generalize.
BOTTOM LINE
In this well controlled randomized study testing whether lorcaserin reduced cocaine use, craving, and consequences, lorcaserin did not appear to be helpful in addressing cocaine use disorder.
For individuals and families seeking recovery: Although there are no FDA-approved medications for cocaine use disorder, contingency management has been shown to be helpful at increasing abstinence in dozens of studies. It is also important to mention that scientists continue to explore other medication options, with some emerging as potential therapeutics that will be tested in further clinical trials.
For treatment professionals and treatment systems: To date, scientists have been unable to develop an effective medication for cocaine use disorder. However, contingency management is helpful at increasing cocaine abstinence. Consider requesting or attending a training hosted by SAMHSA on contingency management (see www.opioidresponsenetwork.org) or referring patients to treatment providers and treatments centers that use this approach.
For scientists: Preclinical studies using drug choice procedures have typically been predictive of failed medication trials; however, these paradigms are not always used in preclinical trials. Studies using drug-choice procedures may be more likely to accurately detect translation to therapeutics in medications trials. Additionally, novel neurobiological approaches, such as targeting multiple mechanisms, may be the most effective way to identify an efficacious medication for cocaine use disorder. Finally, research on the contextual factors associated with return to cocaine use during treatment and recovery, may identify novel targets to improve recovery outcomes for this population.
For policy makers: Although there is not an FDA-approved medication for cocaine use disorder, continued research may eventually help uncover a novel therapeutic that will become an essential tool in the treatment of cocaine use disorder. For this reason, medication development funding to treat cocaine use disorder remains a priority. However, contingency management has demonstrated efficacy for reducing cocaine use disorder. Increasing the availability of contingency management, including through insurance reimbursement, would likely improve public health response to cocaine use disorder. Alternative targets for medications development may also prove to reduce overall harm, such as reduction of cocaine consumption rather than full abstinence.