Given the additional cost, should we still pay for residential treatment? Results of a large longitudinal study within the US VA system
Veterans returning to civilian life are at greater risk than the average person of substance use and other mental health disorders. This large research study offers evidence that residential treatment programs can address this burden, showing promising results for recovery and long-term health.
Veterans are particularly susceptible to the adverse outcomes of substance use disorder, such as increased risk of various medical conditions, mental health diagnoses, and higher mortality rates. In comparison to the general population, veterans with substance use disorder face greater clinical complexity and have heightened treatment needs. The current residential treatment models provide comprehensive 24/7 services for severe substance use disorder, but questions remain regarding their efficacy, especially concerning mortality risk and mental health symptom reduction. Studies of residential and other treatments for veterans can help to guiding future care practices and policy for this at-risk group.
This study used a rigorous quasi-experimental analysis called propensity score matching to compare outcomes of VA patients that were referred to, and attended residential treatment to those who were referred to, but did not attend residential treatment.
HOW WAS THIS STUDY CONDUCTED?
This study included 6177 veterans across more than 60 different residential treatment programs within the VA system matching patients who were referred and attended residential treatment for substance use disorders with a group who were referred but did not attend residential treatment at baseline (i.e., time of referral), 3-, 6-, and 12-months after referral.
The propensity score matching strategy creates a single score from several factors, based on an individual’s likelihood of attending vs. not attending residential treatment – helping to control for the factors associated with selecting into one treatment or another. This is done when randomization to study conditions may not be possible or desirable, but the method helps to build confidence that any observed differences are truly due to the different types of treatments.
The propensity scores were derived from the most recent assessment during the 3 months prior to referral of variables including substance use disorder and other mental health treatment visits, measures of substance use, mental health symptoms (depression, posttraumatic stress and other anxiety, etc.), trauma history, and marital status. The residential vs. comparison group outcomes at 3-, 6-, and 12-month follow-ups included naturalistic observations of health services (i.e., from VA medical record data) and patient reported outcome measures, where analyses used the outcome measures closest in time to each retrospective follow-up point. For the patient reported outcomes, the Brief Addiction Monitor used in this study includes 3 scales: substance use (3 items; 0-90), risk factors (6 items; 0-180), and protective factors (6 items; 0-180) each based on number of days between 0 and 30 for a given item. Of note, the substance use factor captures alcohol use generally, heavy alcohol use days, and other drug use days.
Participants had varying durations of stay in the residential program, but the average time to treatment entry was 24 days after referral and 80% had been discharged by 3 months after referral, suggesting 2-month residential stays were typical. The comparison group did not attend residential treatment during the 12-month study window, but could have attended any combination of standard outpatient services, intensive outpatient programming, acute inpatient or emergency services, primary care or other medical services, or may have also disengaged from care entirely. The comparison group had 9 outpatient substance use disorder visits on average between baseline and 6-months and 15 visits for other mental health concerns.
Participants were 50 years old, on average and 94% male (consistent with the gender make-up at many VAs). With respect to race/ethnicity, 55% were “European American” (White), 34% were “African/Caribbean American” (Black), and 6% were “Latino American” (Hispanic/Latino). Three-quarters were living in urban areas while 20% were married, 39% divorced, and 29% never married.
WHAT DID THIS STUDY FIND?
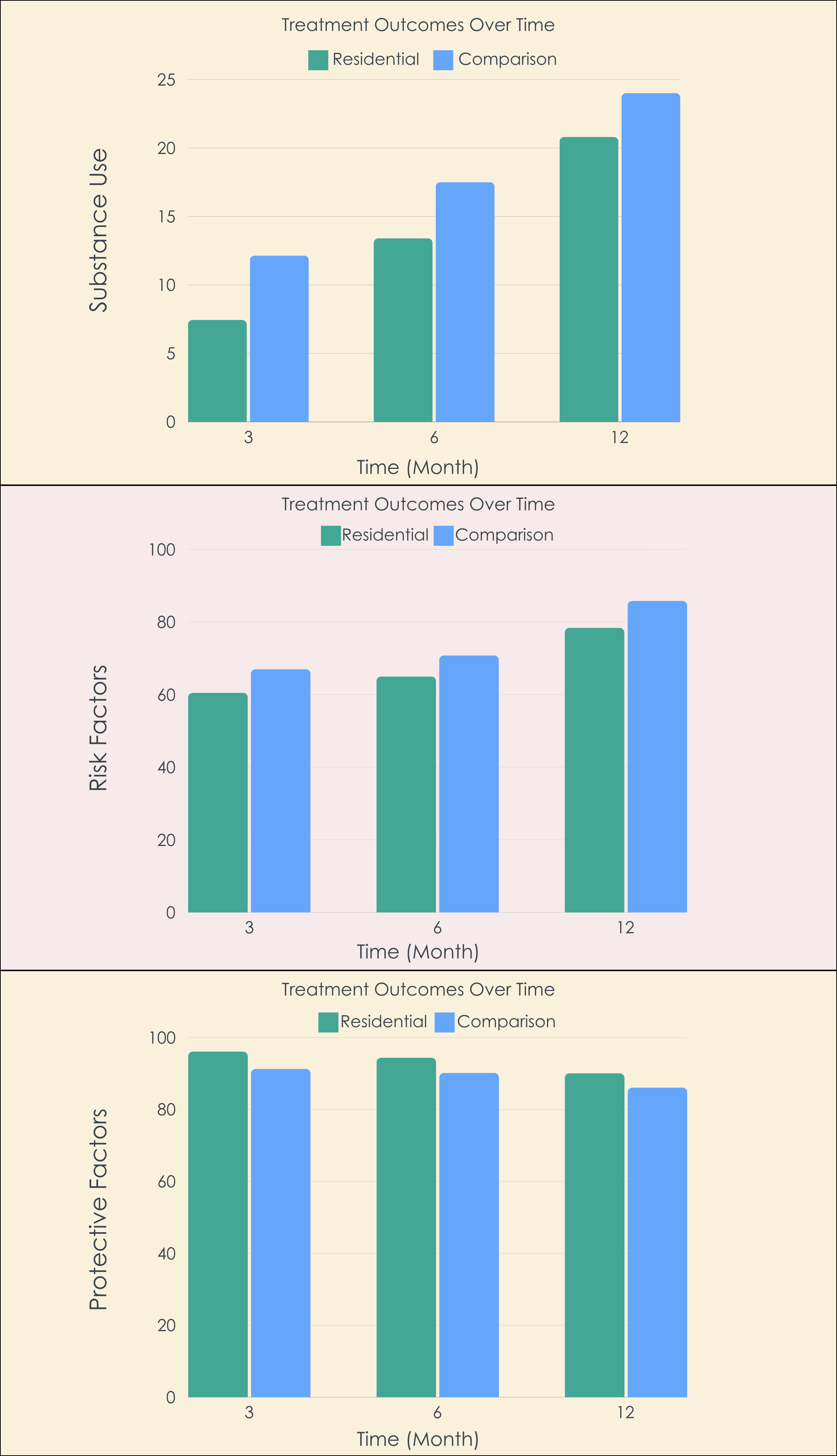
Residential patients with advantage on substance use outcomes
Residential treatment participants had improved substance use, relapse risk, and protective factors relative to the comparison group at 3-, 6-, and 12-month follow-ups.
Residential patients with advantage on behavioral and mental health outcomes too
The residential and comparison groups had similar numbers of emergency room visits, acute inpatient stays, and a measure combining suicide and overdose events. Their depression, posttraumatic stress, and generalized anxiety symptoms, on average, were as good, or better than the comparison group. Notably, at the 12-month follow-up, they had lower posttraumatic stress symptoms, and at the 6-month follow-up lower depressive and generalized anxiety symptoms. Finally, the residential treatment group had 66% lower risk of death during the 12-month follow-up, though the article did not report exact number of participants who died in each group.
Pre- to post-treatment improvements retained over time
In the entire group of participants that attended residential treatment (not only those with a matched participant in the comparison group), there were medium-to-large improvements in substance use disorder and mental health symptoms observed from pre- to post-residential treatment which were sustained out to 12-month follow-up. This suggests that in this sample of VA residential patients, their gains during residential treatment were maintained over a substantial period.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings from this quasi-experimental study suggest that veterans recommended to attend residential substance use disorder treatment had better substance use and related outcomes over 12-month follow-up relative to a matched comparison group that did not attend residential treatment, many of whom attend outpatient services instead.
One of the most striking outcomes was the significant drop in mortality risk for those in residential care, underscoring the importance of these treatment programs in potentially saving lives for those whose clinical profiles are severe enough to warrant a referral for residential level of care. There were also increases for the residential treatment group in number of mental health treatment sessions attended as well as improvements in anxiety and PTSD. It is possible that the residential treatment program (and its corresponding environmental protections against recurrence of use) allowed for more accurate assessment of co-occurring mental health disorders and, consequently, more targeted recommendations for their treatment. Future studies should see if they replicate this apparent benefit of residential versus outpatient treatment for co-occurring mental health conditions given how commonly substance use and mental health disorders co-occur in veteran populations. Overall, the study’s rigorous quasi-experimental design, particularly its use of propensity score matching, adds a level of confidence in these findings, highlighting the method’s strength in accurately assessing the treatment’s effects.
By examining a diverse group of 6177 participants from more than 60 treatment locations, the study also allows these findings to be applied more broadly, potentially with implications for other community-based health care systems. The VA offers ongoing access to an expansive continuum of substance use disorder and mental health treatment, including the use of measurement-based practices that track patient outcomes while identifying the potential need for re-engagement with care once someone has completed treatment. Recovery management approaches like these consistently outperform approaches that consist primarily of discrete episodes of care while simultaneously saving costs.
The exclusion of medical care received outside the VA healthcare system might lead to an incomplete picture of the veterans’ medical service use and risky behavior patterns.
The study did not report primary substance and did not conduct moderation analyses examining whether the benefits of residential vs. comparison levels of care were present across different primary substances (e.g., alcohol, opioids, stimulants, etc.).
The coinciding of the study timeline with the COVID-19 pandemic poses potential confounds, given that the pandemic may have limited the availability and accessibility of treatment services, which could have muted the potential benefits of outpatient care experienced by those in the comparison group who chose not to attend residential treatment.
BOTTOM LINE
This study suggests that, among veterans who are recommended to attend residential treatment, this level of care improves substance use outcomes and reduces mortality risk compared to lower levels of care.
For individuals and families seeking recovery: These results offer important information regarding benefits of residential treatment for individuals and families when making treatment-related decisions. One caveat is that the study did not examine primary substance or other types of potential moderator variables (e.g., psychiatric comorbidity, physical health conditions etc.) and cannot determine whether these residential benefits were present for all of these subgroups equally.
For treatment professionals and treatment systems: The study’s findings provide strong support for the use of residential treatment in effectively managing substance use disorders among veterans with more severe clinical profiles. Of note, it is possible that these higher levels of care enable more targeted diagnostic assessment of, and recommendations for, co-occurring mental health disorders.
For scientists: This study’s use of propensity score matching and data from a broad national sample enhances confidence that the observed differences between residential and comparison groups were due to differences in the treatment levels of care themselves. In the absence of randomized trials to examine the efficacy of residential versus other treatment levels (which poses ethical problems), this study can help inform future longitudinal and demographic-specific research to dissect the long-term effects and regional consistency of residential treatment outcomes.
For policy makers: The results may inform strategic decisions about resource distribution and program enhancement, ensuring veterans with more severe profiles, and potentially those with co-occurring mental health disorders, can attend residential treatment. These findings are also consistent with the known benefits of recovery management approaches employed in VA settings – where patients have long-term access to an expansive set of services in a continuum of care.
Veterans are particularly susceptible to the adverse outcomes of substance use disorder, such as increased risk of various medical conditions, mental health diagnoses, and higher mortality rates. In comparison to the general population, veterans with substance use disorder face greater clinical complexity and have heightened treatment needs. The current residential treatment models provide comprehensive 24/7 services for severe substance use disorder, but questions remain regarding their efficacy, especially concerning mortality risk and mental health symptom reduction. Studies of residential and other treatments for veterans can help to guiding future care practices and policy for this at-risk group.
This study used a rigorous quasi-experimental analysis called propensity score matching to compare outcomes of VA patients that were referred to, and attended residential treatment to those who were referred to, but did not attend residential treatment.
HOW WAS THIS STUDY CONDUCTED?
This study included 6177 veterans across more than 60 different residential treatment programs within the VA system matching patients who were referred and attended residential treatment for substance use disorders with a group who were referred but did not attend residential treatment at baseline (i.e., time of referral), 3-, 6-, and 12-months after referral.
The propensity score matching strategy creates a single score from several factors, based on an individual’s likelihood of attending vs. not attending residential treatment – helping to control for the factors associated with selecting into one treatment or another. This is done when randomization to study conditions may not be possible or desirable, but the method helps to build confidence that any observed differences are truly due to the different types of treatments.
The propensity scores were derived from the most recent assessment during the 3 months prior to referral of variables including substance use disorder and other mental health treatment visits, measures of substance use, mental health symptoms (depression, posttraumatic stress and other anxiety, etc.), trauma history, and marital status. The residential vs. comparison group outcomes at 3-, 6-, and 12-month follow-ups included naturalistic observations of health services (i.e., from VA medical record data) and patient reported outcome measures, where analyses used the outcome measures closest in time to each retrospective follow-up point. For the patient reported outcomes, the Brief Addiction Monitor used in this study includes 3 scales: substance use (3 items; 0-90), risk factors (6 items; 0-180), and protective factors (6 items; 0-180) each based on number of days between 0 and 30 for a given item. Of note, the substance use factor captures alcohol use generally, heavy alcohol use days, and other drug use days.
Participants had varying durations of stay in the residential program, but the average time to treatment entry was 24 days after referral and 80% had been discharged by 3 months after referral, suggesting 2-month residential stays were typical. The comparison group did not attend residential treatment during the 12-month study window, but could have attended any combination of standard outpatient services, intensive outpatient programming, acute inpatient or emergency services, primary care or other medical services, or may have also disengaged from care entirely. The comparison group had 9 outpatient substance use disorder visits on average between baseline and 6-months and 15 visits for other mental health concerns.
Participants were 50 years old, on average and 94% male (consistent with the gender make-up at many VAs). With respect to race/ethnicity, 55% were “European American” (White), 34% were “African/Caribbean American” (Black), and 6% were “Latino American” (Hispanic/Latino). Three-quarters were living in urban areas while 20% were married, 39% divorced, and 29% never married.
WHAT DID THIS STUDY FIND?
Residential patients with advantage on substance use outcomes
Residential treatment participants had improved substance use, relapse risk, and protective factors relative to the comparison group at 3-, 6-, and 12-month follow-ups.
Residential patients with advantage on behavioral and mental health outcomes too
The residential and comparison groups had similar numbers of emergency room visits, acute inpatient stays, and a measure combining suicide and overdose events. Their depression, posttraumatic stress, and generalized anxiety symptoms, on average, were as good, or better than the comparison group. Notably, at the 12-month follow-up, they had lower posttraumatic stress symptoms, and at the 6-month follow-up lower depressive and generalized anxiety symptoms. Finally, the residential treatment group had 66% lower risk of death during the 12-month follow-up, though the article did not report exact number of participants who died in each group.
Pre- to post-treatment improvements retained over time
In the entire group of participants that attended residential treatment (not only those with a matched participant in the comparison group), there were medium-to-large improvements in substance use disorder and mental health symptoms observed from pre- to post-residential treatment which were sustained out to 12-month follow-up. This suggests that in this sample of VA residential patients, their gains during residential treatment were maintained over a substantial period.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings from this quasi-experimental study suggest that veterans recommended to attend residential substance use disorder treatment had better substance use and related outcomes over 12-month follow-up relative to a matched comparison group that did not attend residential treatment, many of whom attend outpatient services instead.
One of the most striking outcomes was the significant drop in mortality risk for those in residential care, underscoring the importance of these treatment programs in potentially saving lives for those whose clinical profiles are severe enough to warrant a referral for residential level of care. There were also increases for the residential treatment group in number of mental health treatment sessions attended as well as improvements in anxiety and PTSD. It is possible that the residential treatment program (and its corresponding environmental protections against recurrence of use) allowed for more accurate assessment of co-occurring mental health disorders and, consequently, more targeted recommendations for their treatment. Future studies should see if they replicate this apparent benefit of residential versus outpatient treatment for co-occurring mental health conditions given how commonly substance use and mental health disorders co-occur in veteran populations. Overall, the study’s rigorous quasi-experimental design, particularly its use of propensity score matching, adds a level of confidence in these findings, highlighting the method’s strength in accurately assessing the treatment’s effects.
By examining a diverse group of 6177 participants from more than 60 treatment locations, the study also allows these findings to be applied more broadly, potentially with implications for other community-based health care systems. The VA offers ongoing access to an expansive continuum of substance use disorder and mental health treatment, including the use of measurement-based practices that track patient outcomes while identifying the potential need for re-engagement with care once someone has completed treatment. Recovery management approaches like these consistently outperform approaches that consist primarily of discrete episodes of care while simultaneously saving costs.
The exclusion of medical care received outside the VA healthcare system might lead to an incomplete picture of the veterans’ medical service use and risky behavior patterns.
The study did not report primary substance and did not conduct moderation analyses examining whether the benefits of residential vs. comparison levels of care were present across different primary substances (e.g., alcohol, opioids, stimulants, etc.).
The coinciding of the study timeline with the COVID-19 pandemic poses potential confounds, given that the pandemic may have limited the availability and accessibility of treatment services, which could have muted the potential benefits of outpatient care experienced by those in the comparison group who chose not to attend residential treatment.
BOTTOM LINE
This study suggests that, among veterans who are recommended to attend residential treatment, this level of care improves substance use outcomes and reduces mortality risk compared to lower levels of care.
For individuals and families seeking recovery: These results offer important information regarding benefits of residential treatment for individuals and families when making treatment-related decisions. One caveat is that the study did not examine primary substance or other types of potential moderator variables (e.g., psychiatric comorbidity, physical health conditions etc.) and cannot determine whether these residential benefits were present for all of these subgroups equally.
For treatment professionals and treatment systems: The study’s findings provide strong support for the use of residential treatment in effectively managing substance use disorders among veterans with more severe clinical profiles. Of note, it is possible that these higher levels of care enable more targeted diagnostic assessment of, and recommendations for, co-occurring mental health disorders.
For scientists: This study’s use of propensity score matching and data from a broad national sample enhances confidence that the observed differences between residential and comparison groups were due to differences in the treatment levels of care themselves. In the absence of randomized trials to examine the efficacy of residential versus other treatment levels (which poses ethical problems), this study can help inform future longitudinal and demographic-specific research to dissect the long-term effects and regional consistency of residential treatment outcomes.
For policy makers: The results may inform strategic decisions about resource distribution and program enhancement, ensuring veterans with more severe profiles, and potentially those with co-occurring mental health disorders, can attend residential treatment. These findings are also consistent with the known benefits of recovery management approaches employed in VA settings – where patients have long-term access to an expansive set of services in a continuum of care.
Veterans are particularly susceptible to the adverse outcomes of substance use disorder, such as increased risk of various medical conditions, mental health diagnoses, and higher mortality rates. In comparison to the general population, veterans with substance use disorder face greater clinical complexity and have heightened treatment needs. The current residential treatment models provide comprehensive 24/7 services for severe substance use disorder, but questions remain regarding their efficacy, especially concerning mortality risk and mental health symptom reduction. Studies of residential and other treatments for veterans can help to guiding future care practices and policy for this at-risk group.
This study used a rigorous quasi-experimental analysis called propensity score matching to compare outcomes of VA patients that were referred to, and attended residential treatment to those who were referred to, but did not attend residential treatment.
HOW WAS THIS STUDY CONDUCTED?
This study included 6177 veterans across more than 60 different residential treatment programs within the VA system matching patients who were referred and attended residential treatment for substance use disorders with a group who were referred but did not attend residential treatment at baseline (i.e., time of referral), 3-, 6-, and 12-months after referral.
The propensity score matching strategy creates a single score from several factors, based on an individual’s likelihood of attending vs. not attending residential treatment – helping to control for the factors associated with selecting into one treatment or another. This is done when randomization to study conditions may not be possible or desirable, but the method helps to build confidence that any observed differences are truly due to the different types of treatments.
The propensity scores were derived from the most recent assessment during the 3 months prior to referral of variables including substance use disorder and other mental health treatment visits, measures of substance use, mental health symptoms (depression, posttraumatic stress and other anxiety, etc.), trauma history, and marital status. The residential vs. comparison group outcomes at 3-, 6-, and 12-month follow-ups included naturalistic observations of health services (i.e., from VA medical record data) and patient reported outcome measures, where analyses used the outcome measures closest in time to each retrospective follow-up point. For the patient reported outcomes, the Brief Addiction Monitor used in this study includes 3 scales: substance use (3 items; 0-90), risk factors (6 items; 0-180), and protective factors (6 items; 0-180) each based on number of days between 0 and 30 for a given item. Of note, the substance use factor captures alcohol use generally, heavy alcohol use days, and other drug use days.
Participants had varying durations of stay in the residential program, but the average time to treatment entry was 24 days after referral and 80% had been discharged by 3 months after referral, suggesting 2-month residential stays were typical. The comparison group did not attend residential treatment during the 12-month study window, but could have attended any combination of standard outpatient services, intensive outpatient programming, acute inpatient or emergency services, primary care or other medical services, or may have also disengaged from care entirely. The comparison group had 9 outpatient substance use disorder visits on average between baseline and 6-months and 15 visits for other mental health concerns.
Participants were 50 years old, on average and 94% male (consistent with the gender make-up at many VAs). With respect to race/ethnicity, 55% were “European American” (White), 34% were “African/Caribbean American” (Black), and 6% were “Latino American” (Hispanic/Latino). Three-quarters were living in urban areas while 20% were married, 39% divorced, and 29% never married.
WHAT DID THIS STUDY FIND?
Residential patients with advantage on substance use outcomes
Residential treatment participants had improved substance use, relapse risk, and protective factors relative to the comparison group at 3-, 6-, and 12-month follow-ups.
Residential patients with advantage on behavioral and mental health outcomes too
The residential and comparison groups had similar numbers of emergency room visits, acute inpatient stays, and a measure combining suicide and overdose events. Their depression, posttraumatic stress, and generalized anxiety symptoms, on average, were as good, or better than the comparison group. Notably, at the 12-month follow-up, they had lower posttraumatic stress symptoms, and at the 6-month follow-up lower depressive and generalized anxiety symptoms. Finally, the residential treatment group had 66% lower risk of death during the 12-month follow-up, though the article did not report exact number of participants who died in each group.
Pre- to post-treatment improvements retained over time
In the entire group of participants that attended residential treatment (not only those with a matched participant in the comparison group), there were medium-to-large improvements in substance use disorder and mental health symptoms observed from pre- to post-residential treatment which were sustained out to 12-month follow-up. This suggests that in this sample of VA residential patients, their gains during residential treatment were maintained over a substantial period.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings from this quasi-experimental study suggest that veterans recommended to attend residential substance use disorder treatment had better substance use and related outcomes over 12-month follow-up relative to a matched comparison group that did not attend residential treatment, many of whom attend outpatient services instead.
One of the most striking outcomes was the significant drop in mortality risk for those in residential care, underscoring the importance of these treatment programs in potentially saving lives for those whose clinical profiles are severe enough to warrant a referral for residential level of care. There were also increases for the residential treatment group in number of mental health treatment sessions attended as well as improvements in anxiety and PTSD. It is possible that the residential treatment program (and its corresponding environmental protections against recurrence of use) allowed for more accurate assessment of co-occurring mental health disorders and, consequently, more targeted recommendations for their treatment. Future studies should see if they replicate this apparent benefit of residential versus outpatient treatment for co-occurring mental health conditions given how commonly substance use and mental health disorders co-occur in veteran populations. Overall, the study’s rigorous quasi-experimental design, particularly its use of propensity score matching, adds a level of confidence in these findings, highlighting the method’s strength in accurately assessing the treatment’s effects.
By examining a diverse group of 6177 participants from more than 60 treatment locations, the study also allows these findings to be applied more broadly, potentially with implications for other community-based health care systems. The VA offers ongoing access to an expansive continuum of substance use disorder and mental health treatment, including the use of measurement-based practices that track patient outcomes while identifying the potential need for re-engagement with care once someone has completed treatment. Recovery management approaches like these consistently outperform approaches that consist primarily of discrete episodes of care while simultaneously saving costs.
The exclusion of medical care received outside the VA healthcare system might lead to an incomplete picture of the veterans’ medical service use and risky behavior patterns.
The study did not report primary substance and did not conduct moderation analyses examining whether the benefits of residential vs. comparison levels of care were present across different primary substances (e.g., alcohol, opioids, stimulants, etc.).
The coinciding of the study timeline with the COVID-19 pandemic poses potential confounds, given that the pandemic may have limited the availability and accessibility of treatment services, which could have muted the potential benefits of outpatient care experienced by those in the comparison group who chose not to attend residential treatment.
BOTTOM LINE
This study suggests that, among veterans who are recommended to attend residential treatment, this level of care improves substance use outcomes and reduces mortality risk compared to lower levels of care.
For individuals and families seeking recovery: These results offer important information regarding benefits of residential treatment for individuals and families when making treatment-related decisions. One caveat is that the study did not examine primary substance or other types of potential moderator variables (e.g., psychiatric comorbidity, physical health conditions etc.) and cannot determine whether these residential benefits were present for all of these subgroups equally.
For treatment professionals and treatment systems: The study’s findings provide strong support for the use of residential treatment in effectively managing substance use disorders among veterans with more severe clinical profiles. Of note, it is possible that these higher levels of care enable more targeted diagnostic assessment of, and recommendations for, co-occurring mental health disorders.
For scientists: This study’s use of propensity score matching and data from a broad national sample enhances confidence that the observed differences between residential and comparison groups were due to differences in the treatment levels of care themselves. In the absence of randomized trials to examine the efficacy of residential versus other treatment levels (which poses ethical problems), this study can help inform future longitudinal and demographic-specific research to dissect the long-term effects and regional consistency of residential treatment outcomes.
For policy makers: The results may inform strategic decisions about resource distribution and program enhancement, ensuring veterans with more severe profiles, and potentially those with co-occurring mental health disorders, can attend residential treatment. These findings are also consistent with the known benefits of recovery management approaches employed in VA settings – where patients have long-term access to an expansive set of services in a continuum of care.