WHAT PROBLEM DOES THIS STUDY ADDRESS?
Many justice-involved individuals receive addiction treatment (e.g., medications for opioid use disorder) while incarcerated but have difficulty accessing such treatments after release. Subsequently, the risk of overdose death skyrockets in the first two weeks post-incarceration. Providing medications for opioid use disorder during or after release can reduce mortality risk, but few programs exist to bridge the gap between justice- and community-based addiction treatment. There is a need to develop and evaluate programs which provide treatment coverage between incarceration and post-incarceration. This study describes the implementation and preliminary outcomes of a telehealth program designed to support treatment continuation for recently incarcerated individuals with an opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
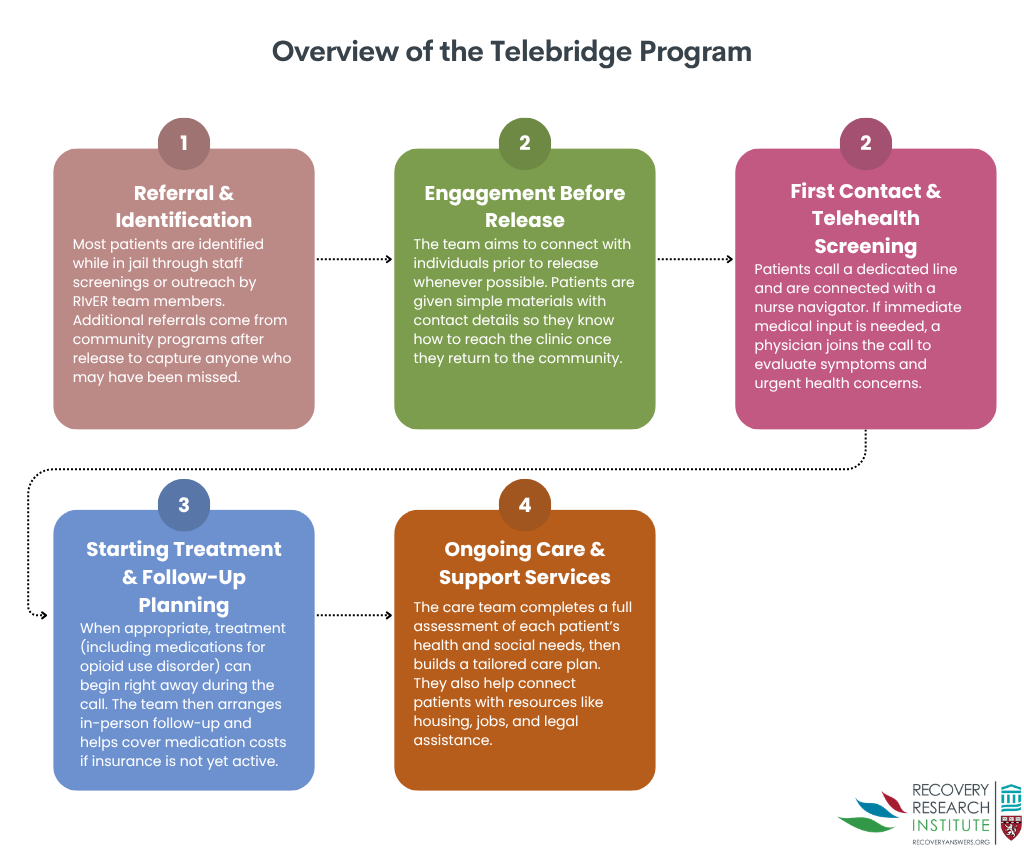
This was a retrospective review of the electronic health records of 250 adults who were released from incarceration with an opioid use disorder between March 1, 2021, and February 1, 2025, and had at least one interaction with the Rethinking Incarceration and Empowering Recovery (RIvER), a telebridge program using telehealth as a “bridge” for individuals between incarceration and healthcare settings. This program, illustrated in the graphic below, engages justice-involved individuals during incarceration and after release to link patients to health care and social services in their communities. Prior to or soon after release, referred patients call the nurse navigator to begin treatment and, if necessary, consult with an on-call physician to address physical health needs (including opioid withdrawal management and opioid use disorder medication prescription). During this telebridge visit, the patient is scheduled for a follow-up in-person appointment. Each patient’s care plan is tailored to meet their individual needs and includes non-medical services such as help finding housing and employment.
Outcomes of this study included time between initial contact with the program nurse and medication for opioid use disorder prescription, treatment retention after initial telebridge visit, rate of completion of in-person clinic visits, number of emergency department visits within 1 year prior to and 1 year post-telebridge appointment, and fatal overdose rates. The goal of these analyses was to describe how the Rethinking Incarceration and Empowering Recovery program impacted substance use treatment utilization and health outcomes (e.g., overdose deaths) among those recently released from incarceration. However, given there was no control group for comparison it is impossible to determine the relative impact of the program on these outcomes. As such, results should be considered descriptive; further research is needed to determine the relative impact of such telebridge programs relative to the usual treatment.
WHAT DID THIS STUDY FIND?
The time between initial telebridge visit and prescription for opioid use disorder medications was short; most patients (91.6%) received a prescription the same day as their initial clinic contact. Patient retention was relatively high: 73.6% of patients attended an in-person clinic appointment after their initial telebridge contact, and 58% of patients attended at least 5 additional appointments within a year of their initial telebridge prescription.
Emergency department utilization trended downward after the telebridge visit. Specifically, 33 patients had fewer emergency department visits in the year after their first telebridge visit than in the year before, although the overall pre-post decline was not statistically significant. One out of 250 patients died of a fatal opioid overdose after completing a telebridge visit.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests the potential utility of programs like Rethinking Incarceration and Empowering Recovery for overcoming barriers to continuing opioid use disorder treatment post-incarceration. Most patients received an opioid use disorder medication prescription the same day as their telebridge visit, which may have reduced the possibility of treatment discontinuation due to delayed access. The use of telemedicine also eliminated the need for transportation to treatment, a common barrier for justice-involved individuals seeking care. Study results are promising, but it is difficult to judge the relative impact of the program because there was no control condition with which to compare results. For instance, it is impossible to know if contact with the program reduced emergency department visits relative to usual care since this was only measured among patients with at least one interaction with the program. In addition, because all included patients contacted the program after referral, bridge programs may be especially useful for individuals already motivated to reduce their opioid use. Regardless of these limitations, findings suggest that this innovative program may help reduce barriers to continuing opioid use disorder treatment post-incarceration. Other promising approaches for justice-involved individuals include diversion programs, which link individuals with addiction treatment instead of jail. Similar programs that bridge the gap between justice- and community-based treatment may be critically important to addressing personal and societal burdens of substance use disorder. However, more research is needed to compare the impact of such programs with usual care.
BOTTOM LINE
Individuals recently released from incarceration face major challenges to initiating or continuing opioid use disorder treatment. Programs that bridge the gap between opioid use disorder treatment received in jails or prisons and in the community may be critical for improving the health outcomes of justice-involved individuals.
- For individuals and families seeking recovery: Beginning or continuing treatment after jail or prison is critical for justice-involved individuals with opioid use disorders. The program described here is innovative and ultimately may help save lives.
- For treatment professionals and treatment systems: This study showed that many justice-involved individuals are willing and able to begin or continue opioid use disorder treatment post-incarceration. Strategies that reduce barriers to treatment access, such as telemedicine approaches, may do a better job at helping facilitate the continuation of treatment after release from jail or prison.
- For scientists: The telebridge program described here is innovative though its relative benefit (i.e., compared to care as usual) remains unclear. It is important that scientists continue developing such programs and compare patient outcomes between participants and appropriate comparison groups.
- For policy makers: If shown to be effective, funding is needed to support innovative opioid use disorder bridge programs like the one described here that improve continuity of care and health outcomes for justice-involved individuals.
CITATIONS
Golden, J., Venkat, D., Yin, Y., & Robertson, T. (2025). Mind the gap: A quality improvement study to determine health care value of rapid-access telemedicine addiction treatment in recently incarcerated individuals. BMC Health Services Research, 25(1), 1351. doi: 10.1186/s12913-025-13520-z.