Up in smoke: Can varenicline help youth quit nicotine vaping?
Rates of youth nicotine vaping have rapidly increased as combustible cigarette smoking decreases. Approaches to reduce vaping are urgently needed. This randomized controlled trial tested whether the medication varenicline, in combination with brief remotely delivered support, was helpful in reducing vaping among youth ages 16 to 25.
Youth vaping has risen rapidly over the past 2 decades since the emergence of electronic nicotine delivery systems despite declines in use of most other substances, including cigarette use. These electronic delivery systems are often referred to as e-cigarettes – a broad category that includes “vape pens” as well as “tanks”, “mods”, and “pods” which may differ in how they store nicotine liquid and power the device. Though vaping is generally thought to be less risky than smoking combustible cigarettes and is used as a harm reduction tool by some to help with smoking cessation, vaping among adolescents is risky for a number of reasons. Vaping may lead to nicotine addiction among those who are using it for the first time (i.e., they are “nicotine naïve”), which in turn may lead to smoking of combustible nicotine products. Compared to youth who do not vape nicotine, those who vape nicotine are also more likely later to begin using marijuana and other drugs. Further, while presumably less harmful, vaping is still associated with health concerns such as carcinogen and heavy metal exposure, alongside pulmonary inflammation, and there has not been enough time to adequately characterize the long-term effects of vaping overthe lifespan. Many youths report wanting to stop or reduce vaping, and approaches that can reduce harm among those already vaping would likely yield high impact public health gains that reduce long term use. Varenicline (previously marketed by the brand name Chantix) is one medication approved by the Food and Drug Administration for the treatment of cigarette smoking. Varenicline is a partial nicotinic acetylcholine receptor agonist, meaning that it binds to the same receptor sites as nicotine and has been shown to reduce craving and withdrawal symptoms. Studies have established varenicline’s efficacy in reducing smoking and vaping among adults; however, no study has tested whether varenicline is effective at reducing vaping among youth. This study tested whether varenicline, in combination with brief remotely delivered support, was effective in reducing vaping among youth relative to placebo or remote support only in the context of a randomized clinical trial.
HOW WAS THIS STUDY CONDUCTED?
The researchers used a double-blind three-group randomized clinical trial to evaluate the effect of varenicline (1 mg twice daily) compared to a matched placebo or a text message-based intervention known as This is Quitting) on vaping reduction in a sample of 261 youth between 16 and 25 years of age who were vaping 5+ days per week and smoking tobacco no more than 4 days per week. Both pharmacotherapy interventions (varenicline or placebo) were also paired with brief, weekly cognitive behavioral intervention (20 minutes per session, 12 sessions total) led by lay counselors. The intervention period lasted 12 weeks total. Assessment of primary outcomes were conducted at baseline, the randomization session, weekly for 12 weeks, and 16, 20, and 24 weeks following the randomization session.
The primary outcome was biochemically confirmed continuous nicotine vaping abstinence across study weeks 9-12. The researchers verified abstinence at each visit through self-report and using observed cotinine levels (30 ng/mL or less). The main outcome was whether varenicline plus behavioral counseling resulted in greater vaping abstinence from 9-12 weeks relative to placebo plus behavioral counseling, after statistically controlling for biological sex and baseline electronic cigarette dependence. Such statistical adjustments help to isolate the effect of interest – i.e., whether changes in vaping can be independently attributed to treatment effects. The authors then conducted additional analyses that included the enhanced usual care condition. The authors also tested models only among participants at least 80% adherent to each medication condition. This allowed for the researchers to examine whether there was a treatment effect among those who actually received the full recommended dose.
Medication was provided at baseline, week 2, and week 4, and adherence was monitored via pill counts and through video recording of self-administration by patients. Visits were conducted via Zoom as necessary. Secondary outcomes included biochemically confirmed continuous nicotine vaping abstinence across study weeks 9-24, past 7-day abstinence at week 12, nicotine withdrawal symptoms, vaping craving, mood, anxiety, and general distress ratings. The researchers also measured risks of varenicline, and safety outcomes including treatment discontinuation, incidence of treatment-related adverse events, and initiation of combustible tobacco products. Secondary outcomes were measured weekly and continuously, and the authors used a statistical approach that accounts for repeated measurement over the course of the study. This allows for the authors to control for time since the start of the treatment initiation.
The sample was, on average, 21 years of age, and vaped nicotine every day. There were slightly more females that males enrolled (53%) and slightly more than half of the sample was White (59%). Participants across conditions reported high motivation to quit vaping. At baseline, more than half of participants had used cannabis in the past month, and more than 75% had used alcohol in the past month. Very few participants (e.g., 6 out of 88 in the varenicline group) smoked tobacco in the past 30 days.
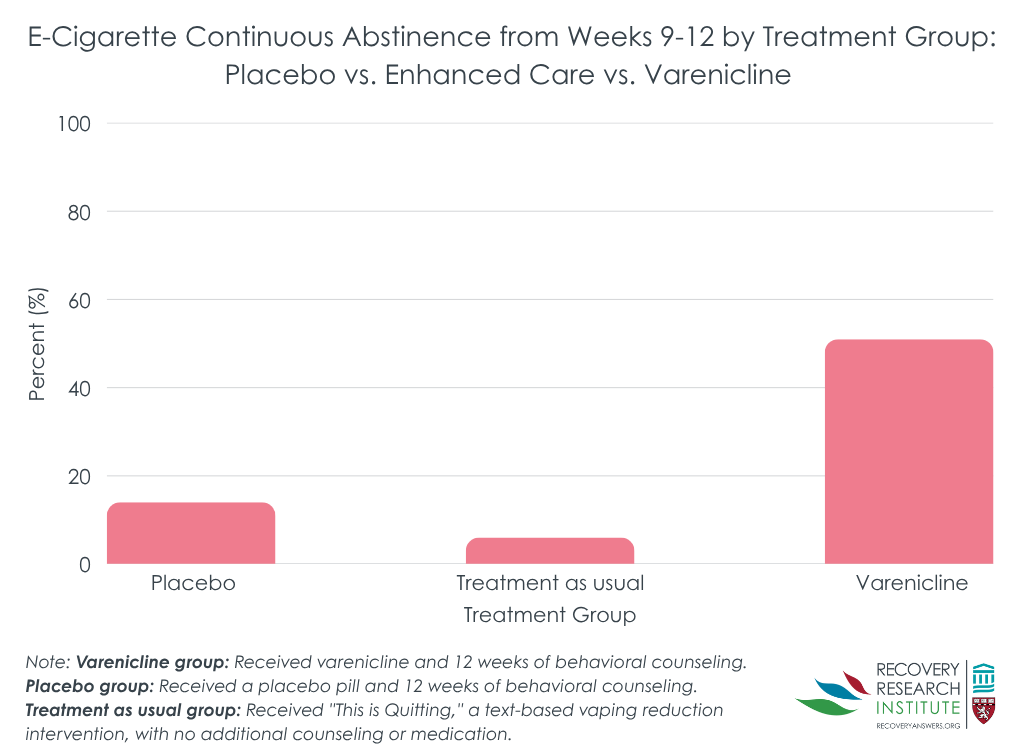
Youth in the varenicline group were 6 times more likely to achieve continuous abstinence from week 9 to week 12 (the primary outcome) compared to the placebo group, and almost 17 times more likely relative to the treatment as usual group (see graph below).
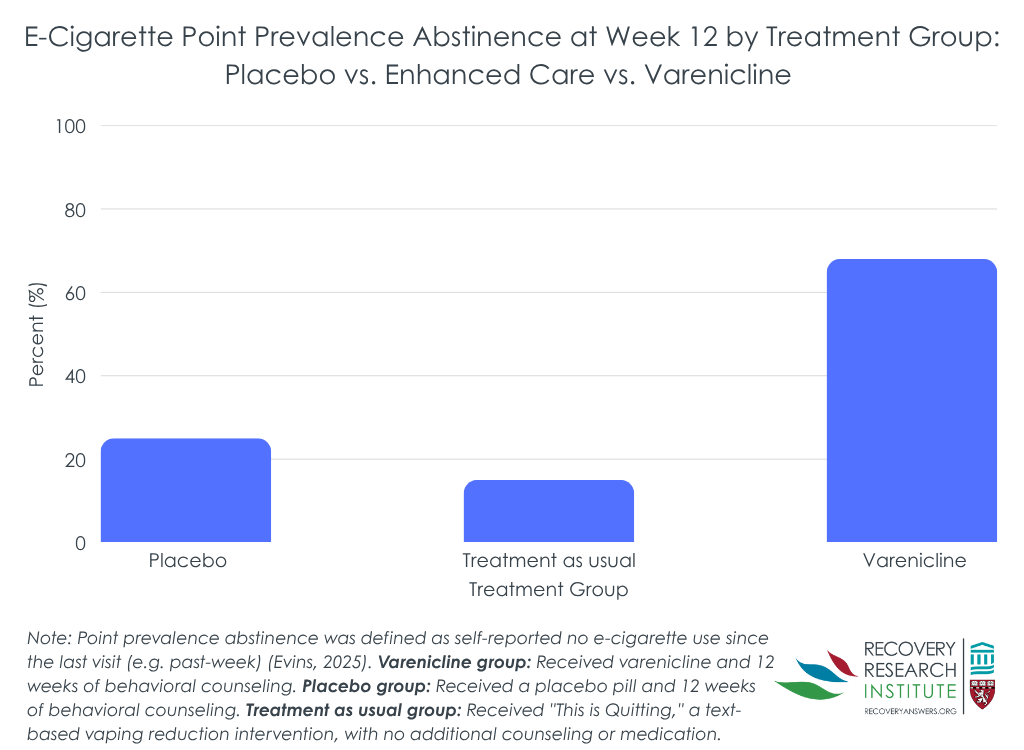
The varenicline group was also much more likely to be abstinent from nicotine vaping during the final week of treatment (see graph below). Finally, the varenicline group remained more likely to be abstinent after the end of the active medication period; 28% of youth in the varenicline group were abstinent from week 9 to week 24, whereas only 7% and 4% of those in the placebo or treatment as usual conditions, respectively, remained abstinent during that period . Though placebo had numerically higher abstinence rates than treatment as usual from week 9 to week 12 and from week 9 to week 24, these differences were not statistically significant, suggesting that they were not meaningfully different.
Varenicline was associated with reduced withdrawal symptoms, craving, and general distress
In analyses restricted to varenicline compared to placebo, those in the varenicline condition reported lower levels of withdrawal symptoms, craving, and general distress relative to those in the placebo condition over the course of the active medication period.
Rates of adverse events were similar in the varenicline and placebo conditions
Within the varenicline group, 81% of youth reported an adverse event, whereas 71% reported an adverse event in the placebo condition. Adverse events were primarily mild in nature (68% in the varenicline condition, 65% in the placebo condition, and 61% in the enhanced usual care condition). A smaller percentage of adverse events were deemed to be moderate in nature (32% in the varenicline condition, 34% in the placebo condition, and 38% in the enhanced usual care condition), whereas less than 2% across conditions were severe in nature. The most common adverse events reported in the varenicline condition were nausea (58% reported), cold symptoms (47% reported), vivid dreams (39% reported), and insomnia (31% reported). No youth had initiated tobacco by the end of the study period in any condition.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Youth tobacco, alcohol, and drug use represent major health problems, as use of these substances during the adolescent and emerging adult years is associated with higher risk of substance use across the lifespan. Thus, targeting youth nicotine vaping is important to improving their overall health, both now and in the future. The results from this study suggest that varenicline is helpful at increasing rates of abstinence from vaping over and above placebo. Currently, varenicline is approved by the Food and Drug Administration for use in reducing combustible tobacco use as low as 16 years of age. These results support varenicline as a smoking cessation aid for vaping, which has risen rapidly among youth in the past few decades.
Of note, however, is that the impressive impact of varenicline diminished after discontinuation such that at about 6 months, just 28% remained abstinent from vaping. This suggests that continued use of the medication may be necessary to sustain abstinence or maybe that other relapse prevention skills need to be taught while actively taking the medication that can help youth stay abstinent after stopping the medication.
The researchers also found that nicotine withdrawal symptoms, craving, and general distress were also lower among those in the varenicline group relative to the both placebo and a text-message-based quit line. This is important because high levels of withdrawal, craving, and distress are all risk factors for continued use of nicotine products and may lead to return to vaping during a cessation attempt.
It is important to note that varenicline was evaluated in combination with brief weekly counseling with a lay clinician. Although the placebo group also received the same behavioral counseling, making it clear that varenicline substantially outperforms placebo, it is possible that the adjunctive counseling helped boost the medication’s efficacy to a degree that would be greater than varenicline alone. The current study was not designed to evaluate varenicline with counseling relative to varenicline alone, and, as such, to achieve the very high levels of youth vaping abstinence observed in this study varenicline in combination with adjunctive behavioral counseling is recommended.
The study was not designed to compare the effects of varenicline alone to varenicline plus counseling, and it is unclear what effect the combination of these two treatments may have had relative to either alone.
The researchers excluded individuals who both vape and regularly use combustible tobacco products, and therefore results may not generalize beyond those who only use electronic cigarettes.
BOTTOM LINE
Varenicline plus brief weekly behavioral counseling appears to be well tolerated and substantially improves rates of vaping cessation among youth motivated to quit vaping. The medication is widely available and can be prescribed by a physician and thus represents a relatively low barrier nicotine vaping cessation tool for youth that is broadly available. Relapse to vaping occurs quite quickly after stopping the medication for many suggesting it may be fruitful to conduct trials of continued medication use or perhaps trials where youth are taught cognitive and behavioral relapse prevention coping skills while benefitting from the medication’s effects.
For individuals and families seeking recovery: If you are an adolescent or young adult and you’d like to reduce your vaping, these results suggest that the medication varenicline may increase the chances that you successfully abstain from vaping, even in the months after you stop taking the medication. It may be important to check in weekly with a counselor while you take varenicline to learn cognitive behavioral strategies that may help you explore ambivalence about quitting and teach skills to manage and maintain the change.
For treatment professionals and treatment systems: If you are a provider or treatment system serving youth, you are likely to encounter teens and emerging adults who are currently vaping, and many may report they would like to quit. Varenicline when combined with brief cognitive behavioral counseling is a relatively safe option that significantly improves rates of smoking cessation in youth, and providing these medications (or referring to someone who can) may improve your patient’s success in kicking the habit. Though many may be motivated to stop vaping, youth may not know how. A simple, nonjudgmental conversation and education about smoking cessation options may be a good place to start with youth who vape.
For scientists: These results demonstrate the efficacy of varenicline plus cognitive behavioral counseling as a smoking cessation aid. Future research may consider a dismantling study that compares varenicline plus behavioral counseling to varenicline alone or behavioral counseling alone to determine whether the effects are additive or if varenicline may be effective on its own, which would decrease the burden of service delivery on healthcare systems. Although this study showed that varenicline plus behavioral counseling was efficacious, it did not establish effectiveness, that is, the utility of this treatment in the context of real-world healthcare delivery (e.g., prescription from a primary care physician). This is an important next step that would confirm that the treatment’s efficacy is generalizable in real-world conditions.
For policy makers: Varenicline is safe and effective for youth attempting to reduce vaping. More funding is needed to continue to do research to confirm effectiveness of this intervention across healthcare systems. Further, funding that supports the dissemination of information regarding the benefits of varenicline in the real world may help enhance the impact of this intervention on reducing vaping among youth.
CITATIONS
Evins, A. E., Cather, C., Reeder, H. T., Evohr, B., Potter, K., Pachas, G. N., Gray, K. M., Levy, S., Rigotti, N. A., Iroegbulem, V., Dufour, J., Casottana, K., Costello, M. A., Gilman, J. M., & Schuster, R. M. (2025). Varenicline for youth nicotine vaping cessation: A randomized clinical trial.JAMA, 333(21), 1876-1886. doi: 10.1001/jama.2025.3810.
Youth vaping has risen rapidly over the past 2 decades since the emergence of electronic nicotine delivery systems despite declines in use of most other substances, including cigarette use. These electronic delivery systems are often referred to as e-cigarettes – a broad category that includes “vape pens” as well as “tanks”, “mods”, and “pods” which may differ in how they store nicotine liquid and power the device. Though vaping is generally thought to be less risky than smoking combustible cigarettes and is used as a harm reduction tool by some to help with smoking cessation, vaping among adolescents is risky for a number of reasons. Vaping may lead to nicotine addiction among those who are using it for the first time (i.e., they are “nicotine naïve”), which in turn may lead to smoking of combustible nicotine products. Compared to youth who do not vape nicotine, those who vape nicotine are also more likely later to begin using marijuana and other drugs. Further, while presumably less harmful, vaping is still associated with health concerns such as carcinogen and heavy metal exposure, alongside pulmonary inflammation, and there has not been enough time to adequately characterize the long-term effects of vaping overthe lifespan. Many youths report wanting to stop or reduce vaping, and approaches that can reduce harm among those already vaping would likely yield high impact public health gains that reduce long term use. Varenicline (previously marketed by the brand name Chantix) is one medication approved by the Food and Drug Administration for the treatment of cigarette smoking. Varenicline is a partial nicotinic acetylcholine receptor agonist, meaning that it binds to the same receptor sites as nicotine and has been shown to reduce craving and withdrawal symptoms. Studies have established varenicline’s efficacy in reducing smoking and vaping among adults; however, no study has tested whether varenicline is effective at reducing vaping among youth. This study tested whether varenicline, in combination with brief remotely delivered support, was effective in reducing vaping among youth relative to placebo or remote support only in the context of a randomized clinical trial.
HOW WAS THIS STUDY CONDUCTED?
The researchers used a double-blind three-group randomized clinical trial to evaluate the effect of varenicline (1 mg twice daily) compared to a matched placebo or a text message-based intervention known as This is Quitting) on vaping reduction in a sample of 261 youth between 16 and 25 years of age who were vaping 5+ days per week and smoking tobacco no more than 4 days per week. Both pharmacotherapy interventions (varenicline or placebo) were also paired with brief, weekly cognitive behavioral intervention (20 minutes per session, 12 sessions total) led by lay counselors. The intervention period lasted 12 weeks total. Assessment of primary outcomes were conducted at baseline, the randomization session, weekly for 12 weeks, and 16, 20, and 24 weeks following the randomization session.
The primary outcome was biochemically confirmed continuous nicotine vaping abstinence across study weeks 9-12. The researchers verified abstinence at each visit through self-report and using observed cotinine levels (30 ng/mL or less). The main outcome was whether varenicline plus behavioral counseling resulted in greater vaping abstinence from 9-12 weeks relative to placebo plus behavioral counseling, after statistically controlling for biological sex and baseline electronic cigarette dependence. Such statistical adjustments help to isolate the effect of interest – i.e., whether changes in vaping can be independently attributed to treatment effects. The authors then conducted additional analyses that included the enhanced usual care condition. The authors also tested models only among participants at least 80% adherent to each medication condition. This allowed for the researchers to examine whether there was a treatment effect among those who actually received the full recommended dose.
Medication was provided at baseline, week 2, and week 4, and adherence was monitored via pill counts and through video recording of self-administration by patients. Visits were conducted via Zoom as necessary. Secondary outcomes included biochemically confirmed continuous nicotine vaping abstinence across study weeks 9-24, past 7-day abstinence at week 12, nicotine withdrawal symptoms, vaping craving, mood, anxiety, and general distress ratings. The researchers also measured risks of varenicline, and safety outcomes including treatment discontinuation, incidence of treatment-related adverse events, and initiation of combustible tobacco products. Secondary outcomes were measured weekly and continuously, and the authors used a statistical approach that accounts for repeated measurement over the course of the study. This allows for the authors to control for time since the start of the treatment initiation.
The sample was, on average, 21 years of age, and vaped nicotine every day. There were slightly more females that males enrolled (53%) and slightly more than half of the sample was White (59%). Participants across conditions reported high motivation to quit vaping. At baseline, more than half of participants had used cannabis in the past month, and more than 75% had used alcohol in the past month. Very few participants (e.g., 6 out of 88 in the varenicline group) smoked tobacco in the past 30 days.
Youth in the varenicline group were 6 times more likely to achieve continuous abstinence from week 9 to week 12 (the primary outcome) compared to the placebo group, and almost 17 times more likely relative to the treatment as usual group (see graph below).
The varenicline group was also much more likely to be abstinent from nicotine vaping during the final week of treatment (see graph below). Finally, the varenicline group remained more likely to be abstinent after the end of the active medication period; 28% of youth in the varenicline group were abstinent from week 9 to week 24, whereas only 7% and 4% of those in the placebo or treatment as usual conditions, respectively, remained abstinent during that period . Though placebo had numerically higher abstinence rates than treatment as usual from week 9 to week 12 and from week 9 to week 24, these differences were not statistically significant, suggesting that they were not meaningfully different.
Varenicline was associated with reduced withdrawal symptoms, craving, and general distress
In analyses restricted to varenicline compared to placebo, those in the varenicline condition reported lower levels of withdrawal symptoms, craving, and general distress relative to those in the placebo condition over the course of the active medication period.
Rates of adverse events were similar in the varenicline and placebo conditions
Within the varenicline group, 81% of youth reported an adverse event, whereas 71% reported an adverse event in the placebo condition. Adverse events were primarily mild in nature (68% in the varenicline condition, 65% in the placebo condition, and 61% in the enhanced usual care condition). A smaller percentage of adverse events were deemed to be moderate in nature (32% in the varenicline condition, 34% in the placebo condition, and 38% in the enhanced usual care condition), whereas less than 2% across conditions were severe in nature. The most common adverse events reported in the varenicline condition were nausea (58% reported), cold symptoms (47% reported), vivid dreams (39% reported), and insomnia (31% reported). No youth had initiated tobacco by the end of the study period in any condition.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Youth tobacco, alcohol, and drug use represent major health problems, as use of these substances during the adolescent and emerging adult years is associated with higher risk of substance use across the lifespan. Thus, targeting youth nicotine vaping is important to improving their overall health, both now and in the future. The results from this study suggest that varenicline is helpful at increasing rates of abstinence from vaping over and above placebo. Currently, varenicline is approved by the Food and Drug Administration for use in reducing combustible tobacco use as low as 16 years of age. These results support varenicline as a smoking cessation aid for vaping, which has risen rapidly among youth in the past few decades.
Of note, however, is that the impressive impact of varenicline diminished after discontinuation such that at about 6 months, just 28% remained abstinent from vaping. This suggests that continued use of the medication may be necessary to sustain abstinence or maybe that other relapse prevention skills need to be taught while actively taking the medication that can help youth stay abstinent after stopping the medication.
The researchers also found that nicotine withdrawal symptoms, craving, and general distress were also lower among those in the varenicline group relative to the both placebo and a text-message-based quit line. This is important because high levels of withdrawal, craving, and distress are all risk factors for continued use of nicotine products and may lead to return to vaping during a cessation attempt.
It is important to note that varenicline was evaluated in combination with brief weekly counseling with a lay clinician. Although the placebo group also received the same behavioral counseling, making it clear that varenicline substantially outperforms placebo, it is possible that the adjunctive counseling helped boost the medication’s efficacy to a degree that would be greater than varenicline alone. The current study was not designed to evaluate varenicline with counseling relative to varenicline alone, and, as such, to achieve the very high levels of youth vaping abstinence observed in this study varenicline in combination with adjunctive behavioral counseling is recommended.
The study was not designed to compare the effects of varenicline alone to varenicline plus counseling, and it is unclear what effect the combination of these two treatments may have had relative to either alone.
The researchers excluded individuals who both vape and regularly use combustible tobacco products, and therefore results may not generalize beyond those who only use electronic cigarettes.
BOTTOM LINE
Varenicline plus brief weekly behavioral counseling appears to be well tolerated and substantially improves rates of vaping cessation among youth motivated to quit vaping. The medication is widely available and can be prescribed by a physician and thus represents a relatively low barrier nicotine vaping cessation tool for youth that is broadly available. Relapse to vaping occurs quite quickly after stopping the medication for many suggesting it may be fruitful to conduct trials of continued medication use or perhaps trials where youth are taught cognitive and behavioral relapse prevention coping skills while benefitting from the medication’s effects.
For individuals and families seeking recovery: If you are an adolescent or young adult and you’d like to reduce your vaping, these results suggest that the medication varenicline may increase the chances that you successfully abstain from vaping, even in the months after you stop taking the medication. It may be important to check in weekly with a counselor while you take varenicline to learn cognitive behavioral strategies that may help you explore ambivalence about quitting and teach skills to manage and maintain the change.
For treatment professionals and treatment systems: If you are a provider or treatment system serving youth, you are likely to encounter teens and emerging adults who are currently vaping, and many may report they would like to quit. Varenicline when combined with brief cognitive behavioral counseling is a relatively safe option that significantly improves rates of smoking cessation in youth, and providing these medications (or referring to someone who can) may improve your patient’s success in kicking the habit. Though many may be motivated to stop vaping, youth may not know how. A simple, nonjudgmental conversation and education about smoking cessation options may be a good place to start with youth who vape.
For scientists: These results demonstrate the efficacy of varenicline plus cognitive behavioral counseling as a smoking cessation aid. Future research may consider a dismantling study that compares varenicline plus behavioral counseling to varenicline alone or behavioral counseling alone to determine whether the effects are additive or if varenicline may be effective on its own, which would decrease the burden of service delivery on healthcare systems. Although this study showed that varenicline plus behavioral counseling was efficacious, it did not establish effectiveness, that is, the utility of this treatment in the context of real-world healthcare delivery (e.g., prescription from a primary care physician). This is an important next step that would confirm that the treatment’s efficacy is generalizable in real-world conditions.
For policy makers: Varenicline is safe and effective for youth attempting to reduce vaping. More funding is needed to continue to do research to confirm effectiveness of this intervention across healthcare systems. Further, funding that supports the dissemination of information regarding the benefits of varenicline in the real world may help enhance the impact of this intervention on reducing vaping among youth.
CITATIONS
Evins, A. E., Cather, C., Reeder, H. T., Evohr, B., Potter, K., Pachas, G. N., Gray, K. M., Levy, S., Rigotti, N. A., Iroegbulem, V., Dufour, J., Casottana, K., Costello, M. A., Gilman, J. M., & Schuster, R. M. (2025). Varenicline for youth nicotine vaping cessation: A randomized clinical trial.JAMA, 333(21), 1876-1886. doi: 10.1001/jama.2025.3810.
Youth vaping has risen rapidly over the past 2 decades since the emergence of electronic nicotine delivery systems despite declines in use of most other substances, including cigarette use. These electronic delivery systems are often referred to as e-cigarettes – a broad category that includes “vape pens” as well as “tanks”, “mods”, and “pods” which may differ in how they store nicotine liquid and power the device. Though vaping is generally thought to be less risky than smoking combustible cigarettes and is used as a harm reduction tool by some to help with smoking cessation, vaping among adolescents is risky for a number of reasons. Vaping may lead to nicotine addiction among those who are using it for the first time (i.e., they are “nicotine naïve”), which in turn may lead to smoking of combustible nicotine products. Compared to youth who do not vape nicotine, those who vape nicotine are also more likely later to begin using marijuana and other drugs. Further, while presumably less harmful, vaping is still associated with health concerns such as carcinogen and heavy metal exposure, alongside pulmonary inflammation, and there has not been enough time to adequately characterize the long-term effects of vaping overthe lifespan. Many youths report wanting to stop or reduce vaping, and approaches that can reduce harm among those already vaping would likely yield high impact public health gains that reduce long term use. Varenicline (previously marketed by the brand name Chantix) is one medication approved by the Food and Drug Administration for the treatment of cigarette smoking. Varenicline is a partial nicotinic acetylcholine receptor agonist, meaning that it binds to the same receptor sites as nicotine and has been shown to reduce craving and withdrawal symptoms. Studies have established varenicline’s efficacy in reducing smoking and vaping among adults; however, no study has tested whether varenicline is effective at reducing vaping among youth. This study tested whether varenicline, in combination with brief remotely delivered support, was effective in reducing vaping among youth relative to placebo or remote support only in the context of a randomized clinical trial.
HOW WAS THIS STUDY CONDUCTED?
The researchers used a double-blind three-group randomized clinical trial to evaluate the effect of varenicline (1 mg twice daily) compared to a matched placebo or a text message-based intervention known as This is Quitting) on vaping reduction in a sample of 261 youth between 16 and 25 years of age who were vaping 5+ days per week and smoking tobacco no more than 4 days per week. Both pharmacotherapy interventions (varenicline or placebo) were also paired with brief, weekly cognitive behavioral intervention (20 minutes per session, 12 sessions total) led by lay counselors. The intervention period lasted 12 weeks total. Assessment of primary outcomes were conducted at baseline, the randomization session, weekly for 12 weeks, and 16, 20, and 24 weeks following the randomization session.
The primary outcome was biochemically confirmed continuous nicotine vaping abstinence across study weeks 9-12. The researchers verified abstinence at each visit through self-report and using observed cotinine levels (30 ng/mL or less). The main outcome was whether varenicline plus behavioral counseling resulted in greater vaping abstinence from 9-12 weeks relative to placebo plus behavioral counseling, after statistically controlling for biological sex and baseline electronic cigarette dependence. Such statistical adjustments help to isolate the effect of interest – i.e., whether changes in vaping can be independently attributed to treatment effects. The authors then conducted additional analyses that included the enhanced usual care condition. The authors also tested models only among participants at least 80% adherent to each medication condition. This allowed for the researchers to examine whether there was a treatment effect among those who actually received the full recommended dose.
Medication was provided at baseline, week 2, and week 4, and adherence was monitored via pill counts and through video recording of self-administration by patients. Visits were conducted via Zoom as necessary. Secondary outcomes included biochemically confirmed continuous nicotine vaping abstinence across study weeks 9-24, past 7-day abstinence at week 12, nicotine withdrawal symptoms, vaping craving, mood, anxiety, and general distress ratings. The researchers also measured risks of varenicline, and safety outcomes including treatment discontinuation, incidence of treatment-related adverse events, and initiation of combustible tobacco products. Secondary outcomes were measured weekly and continuously, and the authors used a statistical approach that accounts for repeated measurement over the course of the study. This allows for the authors to control for time since the start of the treatment initiation.
The sample was, on average, 21 years of age, and vaped nicotine every day. There were slightly more females that males enrolled (53%) and slightly more than half of the sample was White (59%). Participants across conditions reported high motivation to quit vaping. At baseline, more than half of participants had used cannabis in the past month, and more than 75% had used alcohol in the past month. Very few participants (e.g., 6 out of 88 in the varenicline group) smoked tobacco in the past 30 days.
Youth in the varenicline group were 6 times more likely to achieve continuous abstinence from week 9 to week 12 (the primary outcome) compared to the placebo group, and almost 17 times more likely relative to the treatment as usual group (see graph below).
The varenicline group was also much more likely to be abstinent from nicotine vaping during the final week of treatment (see graph below). Finally, the varenicline group remained more likely to be abstinent after the end of the active medication period; 28% of youth in the varenicline group were abstinent from week 9 to week 24, whereas only 7% and 4% of those in the placebo or treatment as usual conditions, respectively, remained abstinent during that period . Though placebo had numerically higher abstinence rates than treatment as usual from week 9 to week 12 and from week 9 to week 24, these differences were not statistically significant, suggesting that they were not meaningfully different.
Varenicline was associated with reduced withdrawal symptoms, craving, and general distress
In analyses restricted to varenicline compared to placebo, those in the varenicline condition reported lower levels of withdrawal symptoms, craving, and general distress relative to those in the placebo condition over the course of the active medication period.
Rates of adverse events were similar in the varenicline and placebo conditions
Within the varenicline group, 81% of youth reported an adverse event, whereas 71% reported an adverse event in the placebo condition. Adverse events were primarily mild in nature (68% in the varenicline condition, 65% in the placebo condition, and 61% in the enhanced usual care condition). A smaller percentage of adverse events were deemed to be moderate in nature (32% in the varenicline condition, 34% in the placebo condition, and 38% in the enhanced usual care condition), whereas less than 2% across conditions were severe in nature. The most common adverse events reported in the varenicline condition were nausea (58% reported), cold symptoms (47% reported), vivid dreams (39% reported), and insomnia (31% reported). No youth had initiated tobacco by the end of the study period in any condition.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Youth tobacco, alcohol, and drug use represent major health problems, as use of these substances during the adolescent and emerging adult years is associated with higher risk of substance use across the lifespan. Thus, targeting youth nicotine vaping is important to improving their overall health, both now and in the future. The results from this study suggest that varenicline is helpful at increasing rates of abstinence from vaping over and above placebo. Currently, varenicline is approved by the Food and Drug Administration for use in reducing combustible tobacco use as low as 16 years of age. These results support varenicline as a smoking cessation aid for vaping, which has risen rapidly among youth in the past few decades.
Of note, however, is that the impressive impact of varenicline diminished after discontinuation such that at about 6 months, just 28% remained abstinent from vaping. This suggests that continued use of the medication may be necessary to sustain abstinence or maybe that other relapse prevention skills need to be taught while actively taking the medication that can help youth stay abstinent after stopping the medication.
The researchers also found that nicotine withdrawal symptoms, craving, and general distress were also lower among those in the varenicline group relative to the both placebo and a text-message-based quit line. This is important because high levels of withdrawal, craving, and distress are all risk factors for continued use of nicotine products and may lead to return to vaping during a cessation attempt.
It is important to note that varenicline was evaluated in combination with brief weekly counseling with a lay clinician. Although the placebo group also received the same behavioral counseling, making it clear that varenicline substantially outperforms placebo, it is possible that the adjunctive counseling helped boost the medication’s efficacy to a degree that would be greater than varenicline alone. The current study was not designed to evaluate varenicline with counseling relative to varenicline alone, and, as such, to achieve the very high levels of youth vaping abstinence observed in this study varenicline in combination with adjunctive behavioral counseling is recommended.
The study was not designed to compare the effects of varenicline alone to varenicline plus counseling, and it is unclear what effect the combination of these two treatments may have had relative to either alone.
The researchers excluded individuals who both vape and regularly use combustible tobacco products, and therefore results may not generalize beyond those who only use electronic cigarettes.
BOTTOM LINE
Varenicline plus brief weekly behavioral counseling appears to be well tolerated and substantially improves rates of vaping cessation among youth motivated to quit vaping. The medication is widely available and can be prescribed by a physician and thus represents a relatively low barrier nicotine vaping cessation tool for youth that is broadly available. Relapse to vaping occurs quite quickly after stopping the medication for many suggesting it may be fruitful to conduct trials of continued medication use or perhaps trials where youth are taught cognitive and behavioral relapse prevention coping skills while benefitting from the medication’s effects.
For individuals and families seeking recovery: If you are an adolescent or young adult and you’d like to reduce your vaping, these results suggest that the medication varenicline may increase the chances that you successfully abstain from vaping, even in the months after you stop taking the medication. It may be important to check in weekly with a counselor while you take varenicline to learn cognitive behavioral strategies that may help you explore ambivalence about quitting and teach skills to manage and maintain the change.
For treatment professionals and treatment systems: If you are a provider or treatment system serving youth, you are likely to encounter teens and emerging adults who are currently vaping, and many may report they would like to quit. Varenicline when combined with brief cognitive behavioral counseling is a relatively safe option that significantly improves rates of smoking cessation in youth, and providing these medications (or referring to someone who can) may improve your patient’s success in kicking the habit. Though many may be motivated to stop vaping, youth may not know how. A simple, nonjudgmental conversation and education about smoking cessation options may be a good place to start with youth who vape.
For scientists: These results demonstrate the efficacy of varenicline plus cognitive behavioral counseling as a smoking cessation aid. Future research may consider a dismantling study that compares varenicline plus behavioral counseling to varenicline alone or behavioral counseling alone to determine whether the effects are additive or if varenicline may be effective on its own, which would decrease the burden of service delivery on healthcare systems. Although this study showed that varenicline plus behavioral counseling was efficacious, it did not establish effectiveness, that is, the utility of this treatment in the context of real-world healthcare delivery (e.g., prescription from a primary care physician). This is an important next step that would confirm that the treatment’s efficacy is generalizable in real-world conditions.
For policy makers: Varenicline is safe and effective for youth attempting to reduce vaping. More funding is needed to continue to do research to confirm effectiveness of this intervention across healthcare systems. Further, funding that supports the dissemination of information regarding the benefits of varenicline in the real world may help enhance the impact of this intervention on reducing vaping among youth.
CITATIONS
Evins, A. E., Cather, C., Reeder, H. T., Evohr, B., Potter, K., Pachas, G. N., Gray, K. M., Levy, S., Rigotti, N. A., Iroegbulem, V., Dufour, J., Casottana, K., Costello, M. A., Gilman, J. M., & Schuster, R. M. (2025). Varenicline for youth nicotine vaping cessation: A randomized clinical trial.JAMA, 333(21), 1876-1886. doi: 10.1001/jama.2025.3810.