Remote possibilities: Addressing rural opioid treatment gaps through telehealth
People in rural communities face multiple barriers to accessing medications for opioid use disorder. Telehealth services may address some of these barriers and improve treatment access and utilization. This study examined how telehealth implementation impacted access to, and utilization of, medications for opioid use disorder in rural counties.
Rural communities have been especially hard hit by the opioid overdose epidemic – research suggests that the rural communities have had higher increases in overdose death rates. Medications for opioid use disorders are first-line treatments for opioid addiction, which work by mitigating withdrawal symptoms, reducing drug cravings, and for agonists like buprenorphine, maintaining opioid tolerance to reduce overdose risk. For rural communities, however, the availability of medications for opioid use disorder can be limited due to a lack of local clinicians and transportation challenges. One proposed solution to address such opioid care disparities is through the usage of telehealth technologies.
To this end, the current study sought to determine how telehealth services have been utilized (especially for medication for opioid use disorder) among rural US communities. Specifically, this work examined rates of telehealth use within rural communities, how telehealth changed access to opioid use disorder treatment, and explored challenges rural communities faced in using telehealth.
HOW WAS THIS STUDY CONDUCTED?
This study was a mixed methods secondary analysis of data submitted to the Rural Communities Opioid Response Program by representatives of funded consortia (i.e., a collection of funded agencies working together) from September 2019 to September 2022. This initiative was created by the Health Resources and Services Administration to fund organizations providing substance use treatment programs in rural communities. The goal of this work was to create a wide network of programs to provide prevention, treatment, and recovery services to rural communities, with an emphasis on increasing access to medications for opioid use disorder. For the current analysis, data were derived from several sources including Performance Improvement and Measurement System data and progress reports. These data were submitted regularly by program directors of each consortium to the Rural Communities Opioid Response Program.
The outcomes of this work included access to opioid use disorder treatment, the degree to which telehealth services were used, and barriers to utilizing telehealth services in rural areas. These outcomes were measured in several ways. First, individual performance data, including the number of individuals who received medications for opioid use disorders were derived from Performance Improvement and Measurement System reports. Quantitative and qualitative data were also derived from quarterly/biannual progress reports. Such reports contained data on the availability of in-person/telehealth-delivered opioid use disorder treatment services across service areas (at both the county- and consortium-level) and barriers specific to using telehealth for opioid use disorder treatment. The authors also estimated the minimum number of individuals in a service area who should have received medications for opioid use disorder (based on national treatment rates) and then compared this benchmark with the number of individuals in every consortium who received said treatment to determine whether each met or exceeded the national rate.
Data for the present study was derived from consortia project directors (N=92) distributed across 37 states in the continental US. Most agencies serviced multiple counties in the same state (64%). Nearly a third (31%) worked within service areas with low population density (e.g., 50,000–99,999 people). Most (62%) were led by a medical provider (e.g., a Critical Access Hospital), with 15% being led by a social service provider (e.g., a community-based organization or tribal organization), 12% were led by a university/research affiliated organization, 9% were led by behavioral health provider, and 2% were led by a government entity (e.g., state or local health department). Consortia included 1,120 member agencies, with an average of 12 member agencies per consortium.
WHAT DID THIS STUDY FIND?
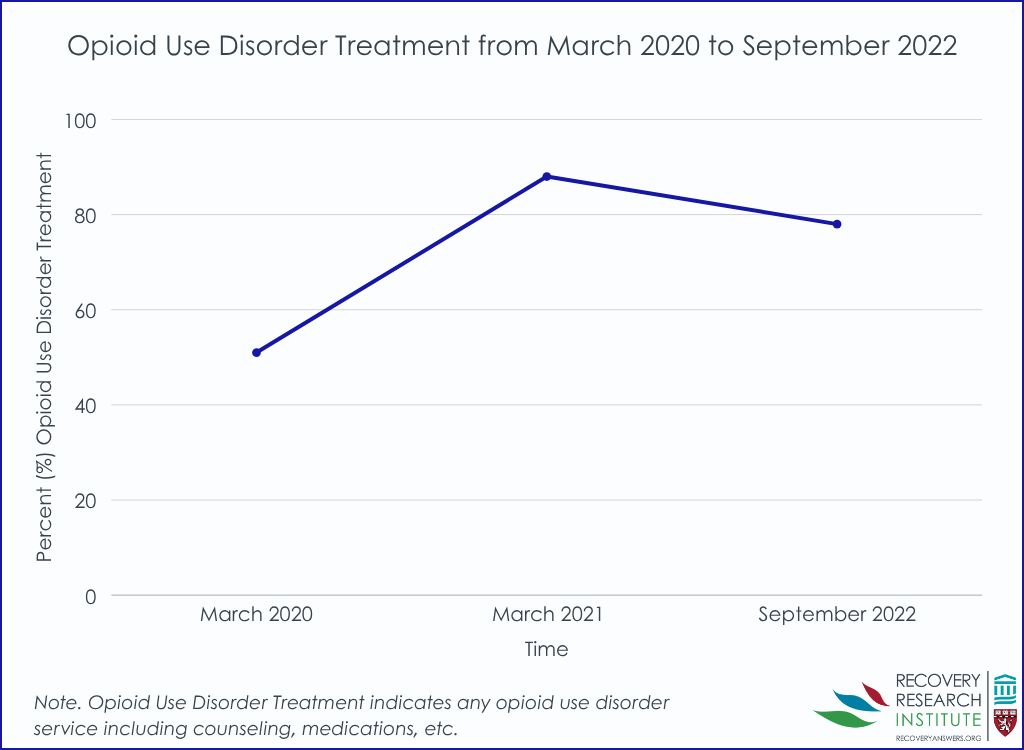
Access to opioid use disorder treatment increased across counties
From March 2020 to March 2021 (the first year of the COVID-19 pandemic), the number of consortia providing telehealth for any opioid use disorder service (counseling, medications, etc.) increased from 47 out of 92 (51%) to 81 out of 92 (88%). However, there was a decline to 70 out of 90 (2 did not report; 78%) in September 2022.
Telehealth services expansion increased opioid disorder treatment access and usage
Programs that implemented telehealth practices reported more individuals receiving medications for opioid use disorder and retained more individuals in treatment (≥3 months) compared to programs that did not use telehealth. These effects were small to medium in magnitude. In addition, 11.5% is the overall rate at which individuals with opioid use disorder receive medications, nationally – communities near programs that provided telehealth were 5 times more likely to beat that national average.
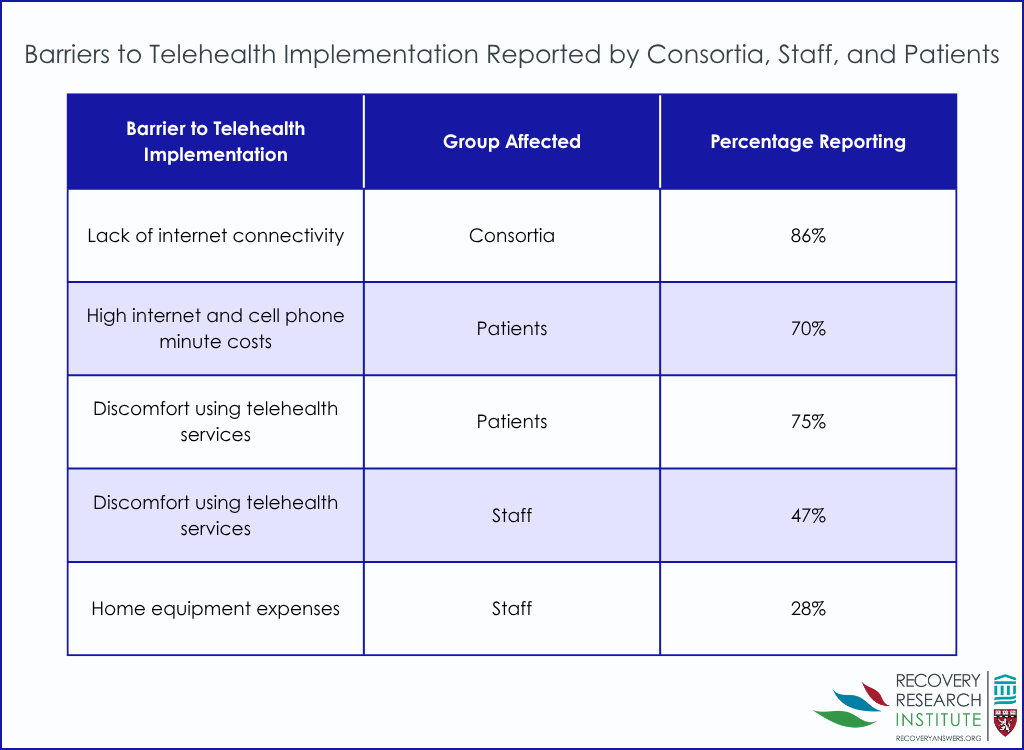
Technological, financial, and comfort challenges impeded implementing telehealth services
A lack of internet connectivity was cited by most consortia (86%) as a challenge to implementing telehealth services. Additionally, telehealth-related costs were also cited as a barrier to effective use (e.g., expenses related to home equipment for staff [28%] and patients reporting high internet and cell phone minute costs [70%]). Finally, general discomfort using telehealth services (both from staff [47%] and patients [75%]) was cited as a barrier to telehealth implementation.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Results of the present study suggest that for those living in the rural US, telehealth can help increase opioid use disorder treatment access and utilization. However, several challenges need to be overcome to facilitate widespread telehealth implementation.
Across consortia, reports indicated that lack of reliable internet access was a significant challenge to implementing telehealth services. This is in line with previous evidence showing that lack of internet infrastructure has stymied telehealth uptake. There is a need for improved broadband internet infrastructure in the rural US. In addition, cost was also cited as a challenge to telehealth implementation. Multiple consortia reported that the high costs of cell phone minutes, data plans, and equipment were especially burdensome for rural practitioners and patients. This is not surprising given the poverty rates are high in rural communities. It is critical to identify potential reimbursement/cost saving mechanisms to create sustainable telehealth access in the rural US. Indeed, without robust implementation efforts like the one featured here, rural individuals, many of whom receive Medicaid, may not reap the benefits of increased treatment access through telehealth. Also, this study suggests that service provider and client discomfort with technology was a barrier to telehealth usage. However, the study did not present more detailed data that could help explain why (e.g., what specifically made providers uncomfortable using telehealth services). More work is needed to better understand the specific comfort needs of patients and how these can be addressed via telehealth. Finally, in this study, the patients’ perceived barriers to telehealth use were reported by the consortia leaders and not actual patients. Thus, these data may not be directly reflective of patient experiences.
Ultimately, the results of this study suggest that telehealth can be a viable modality for substance use disorder treatment in rural settings. Despite the cited barriers, areas in which consortia utilized telehealth services use had significantly higher rates of medication for opioid use disorder utilization compared to areas where telehealth was not used. Although the present study did not examine how effective the telehealth services used were at treating substance use disorders, other research suggests that telehealth is an effective treatment option. Therefore, reducing barriers to telehealth in the rural US could be a way to reduce the impact of substance use in such locations. Efforts to ensure access to telehealth services (e.g., access to affordable high-speed internet) should be expanded.
It is unclear how feasible the telehealth services used are beyond the Rural Communities Opioid Response Program. That is, it is unclear how such services can be sustainably implemented without the continued support of federal funding. The authors do not describe how/if consortia would continue beyond the funding obtained via the program. It is important to identify strategies to ensure telehealth initiatives like those included in the present study continue to operate.
The present study did not report the specific kinds of medications prescribed as part of opioid use disorder treatment. This is relevant as different medications have different protocols which may be challenging to adhere to via telehealth (e.g., extended-release naltrexone requiring an initial 5-7 day period of abstinence).
The qualitative data presented in this study are derived from open-ended responses to routine progress reports/questionnaires. Such qualitative data, while valid and informative, lack the “richness” of other forms of qualitative data. Due to a lack of follow-up questions and exploration possible in other forms of qualitative data collection (e.g., in-depth interviews) the authors could only present basic information on the experiences providers/patients had implementing telehealth services. As such, we have a limited understanding of what exactly may have made telehealth challenging to implement in the rural US. Relatedly, it was beyond the scope of this qualitative methodology to explore potential differences in telehealth implementation challenges between consortia that did or did not implement telehealth services. More work is needed to more fully understand how telehealth barriers may manifest in rural areas and how they can be overcome.
The data presented on patients’ telehealth experiences are not clearly reflective of their experiences. That is, the patients’ perceived barriers to telehealth use were reported by the consortia leaders and not actual patients. It is probable that these leaders did receive feedback about patients’ telehealth experiences, but it is also likely that the nuances/details of this feedback may have been lost when relaying it to Rural Communities Opioid Response Program. This makes it difficult to infer how if/how telehealth met patients’ needs and what implementation strategies to pursue in the future.
BOTTOM LINE
This study highlights the potential of telehealth to expand access to opioid use disorder treatment in rural US communities. Telehealth use was associated with higher medication for opioid use disorder treatment usage and retention. However, barriers including limited broadband internet access, financial costs, and provider and patient discomfort hindered implementation. Although the study was conducted under a federally funded program, suggesting limited scalability without continued support, its findings underscore the need for investment in infrastructure, cost-reduction strategies, and patient-centered design. Future efforts should prioritize sustainable telehealth integration and better understanding of patient experiences to close treatment gaps in rural areas.
For individuals and families seeking recovery: The present study suggests that individuals and families seeking recovery in rural settings may find that telehealth is a viable treatment option for substance use disorder. Telehealth services can be useful in overcoming barriers to in-person care, like transportation challenges and limited local provider availability. Families should encourage their loved ones to explore telehealth options, especially if access to local in-person treatment programs is limited. However, those seeking recovery would do well to check insurance coverage. Many insurers cover telehealth services, but such coverage varies across insurance plans. Barriers to utilizing telehealth for substance use disorder treatment may exist depending on location and insurance coverage type. As telehealth continues to expand, being proactive about understanding available resources and advocating for access to high-quality, remote treatment services can help individuals and families navigate recovery more effectively.
For treatment professionals and treatment systems: The present study highlights the need for treatment professionals and those working within treatment systems to address disparities in telehealth utilization. Providers should work to ensure that telehealth options are accessible and effectively integrated into treatment plans, particularly for hard-to-reach (e.g., rural) populations. This may include assisting patients with navigating insurance coverage and providing technical support for telehealth access. By addressing these barriers, treatment professionals and systems can help maximize the potential of telehealth to improve substance use disorder treatment access and outcomes.
For scientists: The present study underscores the need for scientists to further research the accessibility of telehealth for substance use disorder treatment. This study suggests that telehealth can be a viable way to increase access to medications for opioid use disorder. However, this study also suggests that notable implementation barriers exist (e.g., equipment cost). Furthermore, it is unclear how rural patients perceived telehealth services and how well they met their needs. Future research should continue to explore the factors limiting telehealth use and identify ways to facilitate telehealth use in rural communities. By addressing these gaps, researchers can inform policies that enhance telehealth’s role in expanding equitable access to substance use disorder treatment.
For policy makers: The present study suggests that policymakers may consider strategies that improve access to telehealth substance use disorder treatment in rural communities. For example, policymakers could invest in infrastructure to ensure individuals in rural areas have stable broadband internet so they can reliably access telehealth services. Additionally, policymakers could create funding streams supporting rural community health initiatives. This would ensure the sustainability of opioid use disorder treatment beyond time-limited grant mechanisms (e.g., the Rural Communities Opioid Response Program). By prioritizing these policy changes, lawmakers can strengthen the role of telehealth in expanding access to effective, evidence-based substance use disorder treatment in rural areas.
Rural communities have been especially hard hit by the opioid overdose epidemic – research suggests that the rural communities have had higher increases in overdose death rates. Medications for opioid use disorders are first-line treatments for opioid addiction, which work by mitigating withdrawal symptoms, reducing drug cravings, and for agonists like buprenorphine, maintaining opioid tolerance to reduce overdose risk. For rural communities, however, the availability of medications for opioid use disorder can be limited due to a lack of local clinicians and transportation challenges. One proposed solution to address such opioid care disparities is through the usage of telehealth technologies.
To this end, the current study sought to determine how telehealth services have been utilized (especially for medication for opioid use disorder) among rural US communities. Specifically, this work examined rates of telehealth use within rural communities, how telehealth changed access to opioid use disorder treatment, and explored challenges rural communities faced in using telehealth.
HOW WAS THIS STUDY CONDUCTED?
This study was a mixed methods secondary analysis of data submitted to the Rural Communities Opioid Response Program by representatives of funded consortia (i.e., a collection of funded agencies working together) from September 2019 to September 2022. This initiative was created by the Health Resources and Services Administration to fund organizations providing substance use treatment programs in rural communities. The goal of this work was to create a wide network of programs to provide prevention, treatment, and recovery services to rural communities, with an emphasis on increasing access to medications for opioid use disorder. For the current analysis, data were derived from several sources including Performance Improvement and Measurement System data and progress reports. These data were submitted regularly by program directors of each consortium to the Rural Communities Opioid Response Program.
The outcomes of this work included access to opioid use disorder treatment, the degree to which telehealth services were used, and barriers to utilizing telehealth services in rural areas. These outcomes were measured in several ways. First, individual performance data, including the number of individuals who received medications for opioid use disorders were derived from Performance Improvement and Measurement System reports. Quantitative and qualitative data were also derived from quarterly/biannual progress reports. Such reports contained data on the availability of in-person/telehealth-delivered opioid use disorder treatment services across service areas (at both the county- and consortium-level) and barriers specific to using telehealth for opioid use disorder treatment. The authors also estimated the minimum number of individuals in a service area who should have received medications for opioid use disorder (based on national treatment rates) and then compared this benchmark with the number of individuals in every consortium who received said treatment to determine whether each met or exceeded the national rate.
Data for the present study was derived from consortia project directors (N=92) distributed across 37 states in the continental US. Most agencies serviced multiple counties in the same state (64%). Nearly a third (31%) worked within service areas with low population density (e.g., 50,000–99,999 people). Most (62%) were led by a medical provider (e.g., a Critical Access Hospital), with 15% being led by a social service provider (e.g., a community-based organization or tribal organization), 12% were led by a university/research affiliated organization, 9% were led by behavioral health provider, and 2% were led by a government entity (e.g., state or local health department). Consortia included 1,120 member agencies, with an average of 12 member agencies per consortium.
WHAT DID THIS STUDY FIND?
Access to opioid use disorder treatment increased across counties
From March 2020 to March 2021 (the first year of the COVID-19 pandemic), the number of consortia providing telehealth for any opioid use disorder service (counseling, medications, etc.) increased from 47 out of 92 (51%) to 81 out of 92 (88%). However, there was a decline to 70 out of 90 (2 did not report; 78%) in September 2022.
Telehealth services expansion increased opioid disorder treatment access and usage
Programs that implemented telehealth practices reported more individuals receiving medications for opioid use disorder and retained more individuals in treatment (≥3 months) compared to programs that did not use telehealth. These effects were small to medium in magnitude. In addition, 11.5% is the overall rate at which individuals with opioid use disorder receive medications, nationally – communities near programs that provided telehealth were 5 times more likely to beat that national average.
Technological, financial, and comfort challenges impeded implementing telehealth services
A lack of internet connectivity was cited by most consortia (86%) as a challenge to implementing telehealth services. Additionally, telehealth-related costs were also cited as a barrier to effective use (e.g., expenses related to home equipment for staff [28%] and patients reporting high internet and cell phone minute costs [70%]). Finally, general discomfort using telehealth services (both from staff [47%] and patients [75%]) was cited as a barrier to telehealth implementation.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Results of the present study suggest that for those living in the rural US, telehealth can help increase opioid use disorder treatment access and utilization. However, several challenges need to be overcome to facilitate widespread telehealth implementation.
Across consortia, reports indicated that lack of reliable internet access was a significant challenge to implementing telehealth services. This is in line with previous evidence showing that lack of internet infrastructure has stymied telehealth uptake. There is a need for improved broadband internet infrastructure in the rural US. In addition, cost was also cited as a challenge to telehealth implementation. Multiple consortia reported that the high costs of cell phone minutes, data plans, and equipment were especially burdensome for rural practitioners and patients. This is not surprising given the poverty rates are high in rural communities. It is critical to identify potential reimbursement/cost saving mechanisms to create sustainable telehealth access in the rural US. Indeed, without robust implementation efforts like the one featured here, rural individuals, many of whom receive Medicaid, may not reap the benefits of increased treatment access through telehealth. Also, this study suggests that service provider and client discomfort with technology was a barrier to telehealth usage. However, the study did not present more detailed data that could help explain why (e.g., what specifically made providers uncomfortable using telehealth services). More work is needed to better understand the specific comfort needs of patients and how these can be addressed via telehealth. Finally, in this study, the patients’ perceived barriers to telehealth use were reported by the consortia leaders and not actual patients. Thus, these data may not be directly reflective of patient experiences.
Ultimately, the results of this study suggest that telehealth can be a viable modality for substance use disorder treatment in rural settings. Despite the cited barriers, areas in which consortia utilized telehealth services use had significantly higher rates of medication for opioid use disorder utilization compared to areas where telehealth was not used. Although the present study did not examine how effective the telehealth services used were at treating substance use disorders, other research suggests that telehealth is an effective treatment option. Therefore, reducing barriers to telehealth in the rural US could be a way to reduce the impact of substance use in such locations. Efforts to ensure access to telehealth services (e.g., access to affordable high-speed internet) should be expanded.
It is unclear how feasible the telehealth services used are beyond the Rural Communities Opioid Response Program. That is, it is unclear how such services can be sustainably implemented without the continued support of federal funding. The authors do not describe how/if consortia would continue beyond the funding obtained via the program. It is important to identify strategies to ensure telehealth initiatives like those included in the present study continue to operate.
The present study did not report the specific kinds of medications prescribed as part of opioid use disorder treatment. This is relevant as different medications have different protocols which may be challenging to adhere to via telehealth (e.g., extended-release naltrexone requiring an initial 5-7 day period of abstinence).
The qualitative data presented in this study are derived from open-ended responses to routine progress reports/questionnaires. Such qualitative data, while valid and informative, lack the “richness” of other forms of qualitative data. Due to a lack of follow-up questions and exploration possible in other forms of qualitative data collection (e.g., in-depth interviews) the authors could only present basic information on the experiences providers/patients had implementing telehealth services. As such, we have a limited understanding of what exactly may have made telehealth challenging to implement in the rural US. Relatedly, it was beyond the scope of this qualitative methodology to explore potential differences in telehealth implementation challenges between consortia that did or did not implement telehealth services. More work is needed to more fully understand how telehealth barriers may manifest in rural areas and how they can be overcome.
The data presented on patients’ telehealth experiences are not clearly reflective of their experiences. That is, the patients’ perceived barriers to telehealth use were reported by the consortia leaders and not actual patients. It is probable that these leaders did receive feedback about patients’ telehealth experiences, but it is also likely that the nuances/details of this feedback may have been lost when relaying it to Rural Communities Opioid Response Program. This makes it difficult to infer how if/how telehealth met patients’ needs and what implementation strategies to pursue in the future.
BOTTOM LINE
This study highlights the potential of telehealth to expand access to opioid use disorder treatment in rural US communities. Telehealth use was associated with higher medication for opioid use disorder treatment usage and retention. However, barriers including limited broadband internet access, financial costs, and provider and patient discomfort hindered implementation. Although the study was conducted under a federally funded program, suggesting limited scalability without continued support, its findings underscore the need for investment in infrastructure, cost-reduction strategies, and patient-centered design. Future efforts should prioritize sustainable telehealth integration and better understanding of patient experiences to close treatment gaps in rural areas.
For individuals and families seeking recovery: The present study suggests that individuals and families seeking recovery in rural settings may find that telehealth is a viable treatment option for substance use disorder. Telehealth services can be useful in overcoming barriers to in-person care, like transportation challenges and limited local provider availability. Families should encourage their loved ones to explore telehealth options, especially if access to local in-person treatment programs is limited. However, those seeking recovery would do well to check insurance coverage. Many insurers cover telehealth services, but such coverage varies across insurance plans. Barriers to utilizing telehealth for substance use disorder treatment may exist depending on location and insurance coverage type. As telehealth continues to expand, being proactive about understanding available resources and advocating for access to high-quality, remote treatment services can help individuals and families navigate recovery more effectively.
For treatment professionals and treatment systems: The present study highlights the need for treatment professionals and those working within treatment systems to address disparities in telehealth utilization. Providers should work to ensure that telehealth options are accessible and effectively integrated into treatment plans, particularly for hard-to-reach (e.g., rural) populations. This may include assisting patients with navigating insurance coverage and providing technical support for telehealth access. By addressing these barriers, treatment professionals and systems can help maximize the potential of telehealth to improve substance use disorder treatment access and outcomes.
For scientists: The present study underscores the need for scientists to further research the accessibility of telehealth for substance use disorder treatment. This study suggests that telehealth can be a viable way to increase access to medications for opioid use disorder. However, this study also suggests that notable implementation barriers exist (e.g., equipment cost). Furthermore, it is unclear how rural patients perceived telehealth services and how well they met their needs. Future research should continue to explore the factors limiting telehealth use and identify ways to facilitate telehealth use in rural communities. By addressing these gaps, researchers can inform policies that enhance telehealth’s role in expanding equitable access to substance use disorder treatment.
For policy makers: The present study suggests that policymakers may consider strategies that improve access to telehealth substance use disorder treatment in rural communities. For example, policymakers could invest in infrastructure to ensure individuals in rural areas have stable broadband internet so they can reliably access telehealth services. Additionally, policymakers could create funding streams supporting rural community health initiatives. This would ensure the sustainability of opioid use disorder treatment beyond time-limited grant mechanisms (e.g., the Rural Communities Opioid Response Program). By prioritizing these policy changes, lawmakers can strengthen the role of telehealth in expanding access to effective, evidence-based substance use disorder treatment in rural areas.
Rural communities have been especially hard hit by the opioid overdose epidemic – research suggests that the rural communities have had higher increases in overdose death rates. Medications for opioid use disorders are first-line treatments for opioid addiction, which work by mitigating withdrawal symptoms, reducing drug cravings, and for agonists like buprenorphine, maintaining opioid tolerance to reduce overdose risk. For rural communities, however, the availability of medications for opioid use disorder can be limited due to a lack of local clinicians and transportation challenges. One proposed solution to address such opioid care disparities is through the usage of telehealth technologies.
To this end, the current study sought to determine how telehealth services have been utilized (especially for medication for opioid use disorder) among rural US communities. Specifically, this work examined rates of telehealth use within rural communities, how telehealth changed access to opioid use disorder treatment, and explored challenges rural communities faced in using telehealth.
HOW WAS THIS STUDY CONDUCTED?
This study was a mixed methods secondary analysis of data submitted to the Rural Communities Opioid Response Program by representatives of funded consortia (i.e., a collection of funded agencies working together) from September 2019 to September 2022. This initiative was created by the Health Resources and Services Administration to fund organizations providing substance use treatment programs in rural communities. The goal of this work was to create a wide network of programs to provide prevention, treatment, and recovery services to rural communities, with an emphasis on increasing access to medications for opioid use disorder. For the current analysis, data were derived from several sources including Performance Improvement and Measurement System data and progress reports. These data were submitted regularly by program directors of each consortium to the Rural Communities Opioid Response Program.
The outcomes of this work included access to opioid use disorder treatment, the degree to which telehealth services were used, and barriers to utilizing telehealth services in rural areas. These outcomes were measured in several ways. First, individual performance data, including the number of individuals who received medications for opioid use disorders were derived from Performance Improvement and Measurement System reports. Quantitative and qualitative data were also derived from quarterly/biannual progress reports. Such reports contained data on the availability of in-person/telehealth-delivered opioid use disorder treatment services across service areas (at both the county- and consortium-level) and barriers specific to using telehealth for opioid use disorder treatment. The authors also estimated the minimum number of individuals in a service area who should have received medications for opioid use disorder (based on national treatment rates) and then compared this benchmark with the number of individuals in every consortium who received said treatment to determine whether each met or exceeded the national rate.
Data for the present study was derived from consortia project directors (N=92) distributed across 37 states in the continental US. Most agencies serviced multiple counties in the same state (64%). Nearly a third (31%) worked within service areas with low population density (e.g., 50,000–99,999 people). Most (62%) were led by a medical provider (e.g., a Critical Access Hospital), with 15% being led by a social service provider (e.g., a community-based organization or tribal organization), 12% were led by a university/research affiliated organization, 9% were led by behavioral health provider, and 2% were led by a government entity (e.g., state or local health department). Consortia included 1,120 member agencies, with an average of 12 member agencies per consortium.
WHAT DID THIS STUDY FIND?
Access to opioid use disorder treatment increased across counties
From March 2020 to March 2021 (the first year of the COVID-19 pandemic), the number of consortia providing telehealth for any opioid use disorder service (counseling, medications, etc.) increased from 47 out of 92 (51%) to 81 out of 92 (88%). However, there was a decline to 70 out of 90 (2 did not report; 78%) in September 2022.
Telehealth services expansion increased opioid disorder treatment access and usage
Programs that implemented telehealth practices reported more individuals receiving medications for opioid use disorder and retained more individuals in treatment (≥3 months) compared to programs that did not use telehealth. These effects were small to medium in magnitude. In addition, 11.5% is the overall rate at which individuals with opioid use disorder receive medications, nationally – communities near programs that provided telehealth were 5 times more likely to beat that national average.
Technological, financial, and comfort challenges impeded implementing telehealth services
A lack of internet connectivity was cited by most consortia (86%) as a challenge to implementing telehealth services. Additionally, telehealth-related costs were also cited as a barrier to effective use (e.g., expenses related to home equipment for staff [28%] and patients reporting high internet and cell phone minute costs [70%]). Finally, general discomfort using telehealth services (both from staff [47%] and patients [75%]) was cited as a barrier to telehealth implementation.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Results of the present study suggest that for those living in the rural US, telehealth can help increase opioid use disorder treatment access and utilization. However, several challenges need to be overcome to facilitate widespread telehealth implementation.
Across consortia, reports indicated that lack of reliable internet access was a significant challenge to implementing telehealth services. This is in line with previous evidence showing that lack of internet infrastructure has stymied telehealth uptake. There is a need for improved broadband internet infrastructure in the rural US. In addition, cost was also cited as a challenge to telehealth implementation. Multiple consortia reported that the high costs of cell phone minutes, data plans, and equipment were especially burdensome for rural practitioners and patients. This is not surprising given the poverty rates are high in rural communities. It is critical to identify potential reimbursement/cost saving mechanisms to create sustainable telehealth access in the rural US. Indeed, without robust implementation efforts like the one featured here, rural individuals, many of whom receive Medicaid, may not reap the benefits of increased treatment access through telehealth. Also, this study suggests that service provider and client discomfort with technology was a barrier to telehealth usage. However, the study did not present more detailed data that could help explain why (e.g., what specifically made providers uncomfortable using telehealth services). More work is needed to better understand the specific comfort needs of patients and how these can be addressed via telehealth. Finally, in this study, the patients’ perceived barriers to telehealth use were reported by the consortia leaders and not actual patients. Thus, these data may not be directly reflective of patient experiences.
Ultimately, the results of this study suggest that telehealth can be a viable modality for substance use disorder treatment in rural settings. Despite the cited barriers, areas in which consortia utilized telehealth services use had significantly higher rates of medication for opioid use disorder utilization compared to areas where telehealth was not used. Although the present study did not examine how effective the telehealth services used were at treating substance use disorders, other research suggests that telehealth is an effective treatment option. Therefore, reducing barriers to telehealth in the rural US could be a way to reduce the impact of substance use in such locations. Efforts to ensure access to telehealth services (e.g., access to affordable high-speed internet) should be expanded.
It is unclear how feasible the telehealth services used are beyond the Rural Communities Opioid Response Program. That is, it is unclear how such services can be sustainably implemented without the continued support of federal funding. The authors do not describe how/if consortia would continue beyond the funding obtained via the program. It is important to identify strategies to ensure telehealth initiatives like those included in the present study continue to operate.
The present study did not report the specific kinds of medications prescribed as part of opioid use disorder treatment. This is relevant as different medications have different protocols which may be challenging to adhere to via telehealth (e.g., extended-release naltrexone requiring an initial 5-7 day period of abstinence).
The qualitative data presented in this study are derived from open-ended responses to routine progress reports/questionnaires. Such qualitative data, while valid and informative, lack the “richness” of other forms of qualitative data. Due to a lack of follow-up questions and exploration possible in other forms of qualitative data collection (e.g., in-depth interviews) the authors could only present basic information on the experiences providers/patients had implementing telehealth services. As such, we have a limited understanding of what exactly may have made telehealth challenging to implement in the rural US. Relatedly, it was beyond the scope of this qualitative methodology to explore potential differences in telehealth implementation challenges between consortia that did or did not implement telehealth services. More work is needed to more fully understand how telehealth barriers may manifest in rural areas and how they can be overcome.
The data presented on patients’ telehealth experiences are not clearly reflective of their experiences. That is, the patients’ perceived barriers to telehealth use were reported by the consortia leaders and not actual patients. It is probable that these leaders did receive feedback about patients’ telehealth experiences, but it is also likely that the nuances/details of this feedback may have been lost when relaying it to Rural Communities Opioid Response Program. This makes it difficult to infer how if/how telehealth met patients’ needs and what implementation strategies to pursue in the future.
BOTTOM LINE
This study highlights the potential of telehealth to expand access to opioid use disorder treatment in rural US communities. Telehealth use was associated with higher medication for opioid use disorder treatment usage and retention. However, barriers including limited broadband internet access, financial costs, and provider and patient discomfort hindered implementation. Although the study was conducted under a federally funded program, suggesting limited scalability without continued support, its findings underscore the need for investment in infrastructure, cost-reduction strategies, and patient-centered design. Future efforts should prioritize sustainable telehealth integration and better understanding of patient experiences to close treatment gaps in rural areas.
For individuals and families seeking recovery: The present study suggests that individuals and families seeking recovery in rural settings may find that telehealth is a viable treatment option for substance use disorder. Telehealth services can be useful in overcoming barriers to in-person care, like transportation challenges and limited local provider availability. Families should encourage their loved ones to explore telehealth options, especially if access to local in-person treatment programs is limited. However, those seeking recovery would do well to check insurance coverage. Many insurers cover telehealth services, but such coverage varies across insurance plans. Barriers to utilizing telehealth for substance use disorder treatment may exist depending on location and insurance coverage type. As telehealth continues to expand, being proactive about understanding available resources and advocating for access to high-quality, remote treatment services can help individuals and families navigate recovery more effectively.
For treatment professionals and treatment systems: The present study highlights the need for treatment professionals and those working within treatment systems to address disparities in telehealth utilization. Providers should work to ensure that telehealth options are accessible and effectively integrated into treatment plans, particularly for hard-to-reach (e.g., rural) populations. This may include assisting patients with navigating insurance coverage and providing technical support for telehealth access. By addressing these barriers, treatment professionals and systems can help maximize the potential of telehealth to improve substance use disorder treatment access and outcomes.
For scientists: The present study underscores the need for scientists to further research the accessibility of telehealth for substance use disorder treatment. This study suggests that telehealth can be a viable way to increase access to medications for opioid use disorder. However, this study also suggests that notable implementation barriers exist (e.g., equipment cost). Furthermore, it is unclear how rural patients perceived telehealth services and how well they met their needs. Future research should continue to explore the factors limiting telehealth use and identify ways to facilitate telehealth use in rural communities. By addressing these gaps, researchers can inform policies that enhance telehealth’s role in expanding equitable access to substance use disorder treatment.
For policy makers: The present study suggests that policymakers may consider strategies that improve access to telehealth substance use disorder treatment in rural communities. For example, policymakers could invest in infrastructure to ensure individuals in rural areas have stable broadband internet so they can reliably access telehealth services. Additionally, policymakers could create funding streams supporting rural community health initiatives. This would ensure the sustainability of opioid use disorder treatment beyond time-limited grant mechanisms (e.g., the Rural Communities Opioid Response Program). By prioritizing these policy changes, lawmakers can strengthen the role of telehealth in expanding access to effective, evidence-based substance use disorder treatment in rural areas.