Psychosocial treatments for Black patients: Do they benefit?
Black Americans experience more harms from substance use relative to people from other racial demographics who use substances, despite similar or lower rates of use. Determining whether treatments help Black individuals can be a challenge because they make up smaller proportions of study samples. This study pooled several randomized controlled trials to determine how Black individuals who use cocaine or opioids respond to psychosocial treatments.
Black Americans who use cocaine bear a disproportionate number of cocaine-related harms relative to other racial demographic groups. Though using comparable or lower amounts of cocaine, Black Americans experience higher rates of cocaine use disorder and have recently experienced greater rates of increase in cocaine-involved deaths. Though effective pharmacotherapeutic treatments for cocaine use remain elusive, there is strong evidence for the efficacy of psychosocial interventions such as contingency management and cognitive behavioral therapy. Most psychosocial treatments have been evaluated with disproportionately white samples, and it is unclear if such treatments are also useful for Black Americans.
HOW WAS THIS STUDY CONDUCTED?
To solve this problem, the authors conducted what is called an “integrative data analysis” of randomized clinical trials of behavioral interventions for substance use that included self-identified Black participants and that measured cocaine use and/or opioid use outcomes. The authors searched the Clinical Trials Network database in 2021 and found 9 randomized clinical trials that met these criteria.
The analyses conducted by the researchers included 1,381 self-identifying Black adults enrolled in one of these 9 clinical trials with baseline cocaine and/or opioid use. The researchers wanted to determine whether psychosocial treatments were effective for Black participants enrolled in the study. The researchers categorized all interventions across the 9 studies into three groups: (1) social-contextual interventions (i.e., that address social and cognitive factors that underlie substance use disorder and recovery), (2) contingency management, and (3) treatment as usual/control. The researchers created 3 “latent” substance severity outcome scores: one for cocaine use outcomes, one for opioid use outcomes, and one for other substance outcomes. The researchers were able to extract data from each clinical trial at baseline, the end of treatment, and then 3-, 6-, 9-, and 12-months after the end of treatment. Because different trials used different substance use outcome measures, the researchers used statistical approaches to make outcomes comparable across studies. The researchers then used statistical analyses to determine how substance use outcomes changed over time separately for each type of treatment. The researchers compared outcomes across treatment groups.
The sample was, on average, 40 years old and 51.7% male. 56.2% of the sample was single or never married, and 75.5% had a high school degree or lower. The researchers evaluated whether there were demographic differences across treatment groups. Although most identified as only Black, 7.7% identified as multiracial Black. Only marital status differed, with 37% of participants in the contingency management group reporting that they are divorced compared to only 27.9% and 27.5% in the social-contextual interventions and the treatment as usual control groups. To account for this difference, the researchers used an approach called propensity score weighting to control for marital status to isolate the effect of condition (social-contextual interventions vs. contingency management vs. treatment as usual) on substance use outcomes.
WHAT DID THIS STUDY FIND?
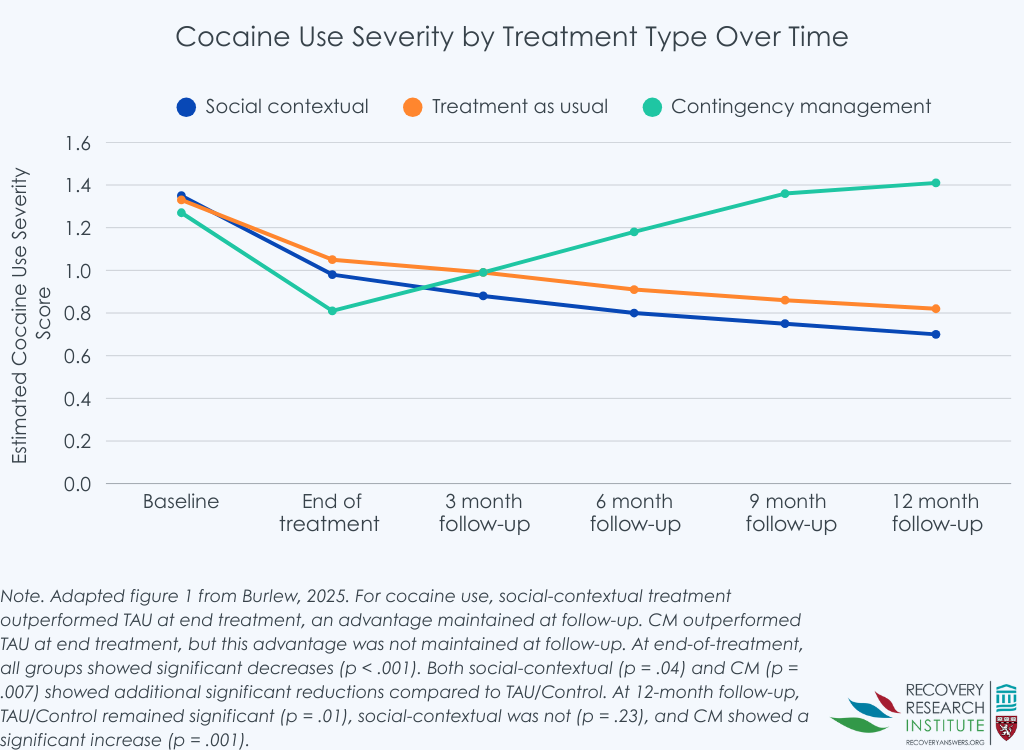
Changes in cocaine use severity across treatment groups
Across all treatments, cocaine use disorder severity decreased from baseline to the end of treatment. Decreases in cocaine severity were the greatest for those in the social-contextual treatments and contingency management relative to treatment as usual (see graph below). At 12 months, reductions in cocaine use from baseline were observed for treatment as usual and social-contextual interventions. There was a small effect size difference between these two conditions, such that cocaine use severity among Black participants in social-contextual interventions was slightly lower (i.e., a better outcome). There were differences in 12-month cocaine use severity between both treatment as usual and social-contextual interventions and contingency management in cocaine use severity, with cocaine use severity in the contingency management condition returning to baseline levels of severity by the 12-month follow up.
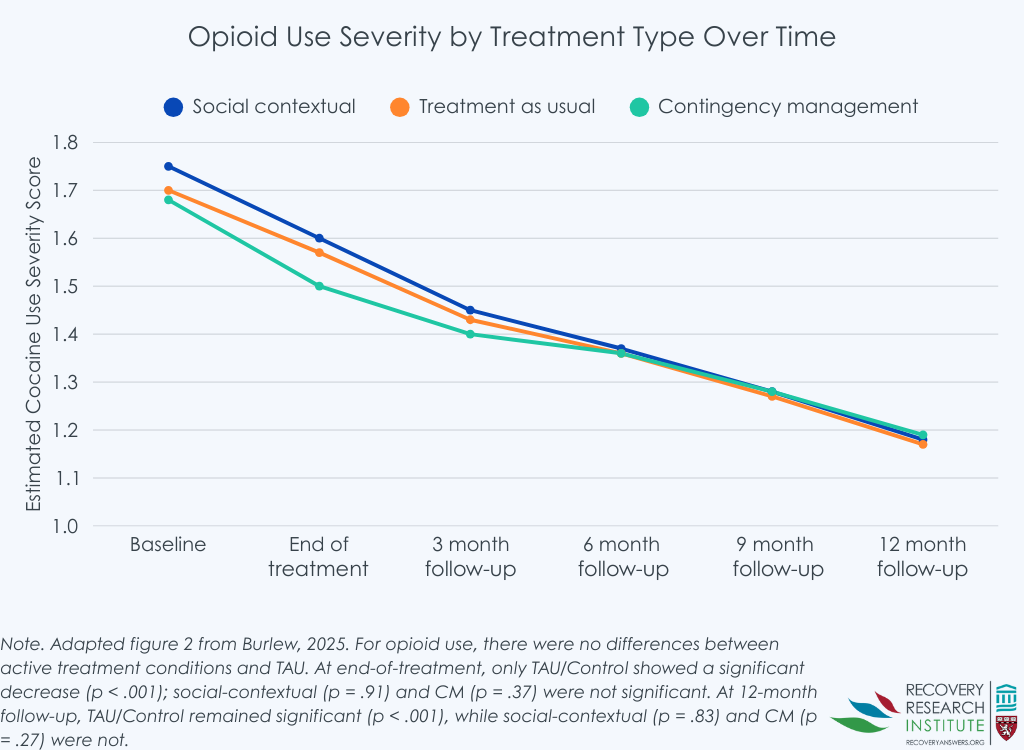
Changes in opioid use severity across treatment groups
Across all treatments, opioid use severity decreased from baseline to the end of treatment. Decreases in opioid severity did not differ between the treatment conditions (see graph below). Opioid severity continued to decline across all treatment conditions through 12 months, and changes did not differ across different groups.
Changes in overall substance use severity across treatment groups
Overall substance use severity decreased from baseline to the end of treatment for those in the treatment as usual condition. Social-contextual treatments did not differ from treatment as usual in change in overall substance severity from baseline to end of treatment. However, contingency management showed significant decreases in overall substance use severity relative to treatment as usual. From the end of treatment to 12 months, participants in the treatment as usual and social-contextual interventions continued to decrease overall substance use severity. There was no difference in change between social-contextual interventions and treatment as usual. There were differences in 12-month cocaine use severity between both treatment as usual and social-contextual interventions and contingency management in overall substance use severity. Like with cocaine use, overall substance use severity in the contingency management condition returned to baseline levels of severity by the 12-month follow up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For cocaine use and general substance use, there was a slight advantage for social-contextual interventions over treatment as usual conditions, suggesting that interventions specifically targeting factors beyond substance use, such as those that also target trauma, social support, family relationships, or comorbid psychiatric conditions, might be slightly more useful in reducing cocaine use among Black people with cocaine use disorder. However, the effects were quite small, suggesting that the additional added benefit beyond treatment as usual is modest. This is not uncommon – treatment as usual, which in this study varied by trial, but usually included group therapy, individual therapy, and case management is often difficult to “beat” in clinical trials. This may be, in part, due to shared approaches across conditions (i.e., relapse prevention skills, referrals to mutual-help groups, etc.) and their ability to boost common therapeutic factors, like abstinence motivation and self-efficacy.
The study has two important caveats. First, the study did not define “benefit” from treatment for Black participants, but rather compared contingency management and a group of social-contextual treatments (e.g., cognitive-behavioral therapy) to treatment-as-usual, which differs by study but typically involves both individual and group therapies that help participants develop coping and other relapse prevention skills, and refers them to community resources like mutual-help groups (e.g., Alcoholics Anonymous). Because of the lack of definition specific to treatment “benefits”, all that can be said, ultimately, is that there appears to be at least some positive gains related to treatment effects for Black individuals. Second, perhaps an obvious question not addressed in this study, is whether Black individuals respond better or worse than other racial groups. Thus, although there was some improvement in this sample, it remains unclear whether Black patients respond differently somewhat limiting one’s ability to make recommendations for this understudied population of individuals with substance use disorder.
While contingency management was associated with decreases in cocaine, opioid, and overall substance use severity from baseline to the end of treatment, both cocaine use and overall substance use returned to pre-treatment levels. This suggests that contingency management did not have lasting effects for Black participants in these studies. Presumably, contingency management treatment effects were driven by the incentives used in this treatment approach which are removed after the course of treatment. As such, contingency management may be a useful approach for helping to reduce substance use initially, but additional approaches may be necessary to ensure such changes in substances remain beyond treatment.
Although opioid use decreased for all treatment groups, from baseline to end of treatment and through the 12-month follow up, there were no differences between treatment groups. Research has demonstrated that medications for opioid use disorder are consistently effective approaches for reducing opioid use disorder in the general population – with one exception, the treatment as usual conditions did not include medications for opioid use disorder. Importantly, other research shows Black individuals may be skeptical of opioid use disorder medications, due to past negative experiences with them and mistrust toward professional-medical approaches. As the study authors note, work may be necessary to culturally tailor psychosocial interventions to target unique issues facing black individuals (e.g., racial discrimination, etc.) in order to increase efficacy beyond treatment as usual.
The study did not compare outcomes to other racial groups, so it remains unclear whether Black participants response is better or worse than other racial groups. Also, there is no operational definition of treatment “benefit”, thus it remains unclear whether the magnitude of observed improvements in this study signify that Black patients actually “benefit” from treatment.
This study combined different treatments and compared against different control groups. Control conditions ranged from an informational pamphlet to assessment and referral to treatment, to group/individual offerings, ranging from 1-6 sessions. The relative difference between treatment as usual and the various active treatment conditions may differ depending on the comparison condition. However, this was not examined in the study.
BOTTOM LINE
For Black individuals, social-contextual interventions that target factors underlying substance use disorder and recovery (e.g., family relationships, social support, etc.) have a modest benefit over treatment as usual in reducing cocaine and general substance use, and the benefits persist after the end of treatment. Contingency management is associated with decreases in cocaine and general substance use during treatment, but these benefits are short-lived as substance use returns to pre-treatment levels after the treatment ends.
For individuals and families seeking recovery: If you are a person self-identifying as Black and you are seeking treatment for substance use disorder, you may be more likely to benefit from treatments that target both substances and other important factors such as trauma, family, or other conditions that commonly co-occur with substance use. Importantly, while contingency management may be beneficial during the treatment, it may be important to identify additional resources to maintain reductions after the treatment ends.
For treatment professionals and treatment systems: If you are a treatment provider, it may be important to use interventions that target social-contextual factors, such as family, trauma, or other co-occurring conditions, in addition to substance use when working with patients who are Black.
For scientists: There was some evidence that social-contextual treatments were more effective than control interventions at reducing cocaine use and overall substance use among Black participants. However, the benefits were modest. More research is needed to determine whether other treatments might be more effective for Black populations. Further, there have been recent calls for more culturally tailored interventions, which may be able to increase efficacy beyond that of interventions that are not culturally tailored. Finally, alternative approaches beyond traditional psychotherapy, such as mutual support groups or other recovery support services, are additional potential options that should be tested within Black populations to determine efficacy.
For policy makers: The current study was based on randomized clinical trials that tested interventions in Black populations; however, only nine trials met inclusion criteria. Policy that increases funding for clinical trials in diverse populations may increase the number of clinical trials available for this type of work and may ultimately improve our ability to answer questions about the efficacy of specific trials in specific populations.
Black Americans who use cocaine bear a disproportionate number of cocaine-related harms relative to other racial demographic groups. Though using comparable or lower amounts of cocaine, Black Americans experience higher rates of cocaine use disorder and have recently experienced greater rates of increase in cocaine-involved deaths. Though effective pharmacotherapeutic treatments for cocaine use remain elusive, there is strong evidence for the efficacy of psychosocial interventions such as contingency management and cognitive behavioral therapy. Most psychosocial treatments have been evaluated with disproportionately white samples, and it is unclear if such treatments are also useful for Black Americans.
HOW WAS THIS STUDY CONDUCTED?
To solve this problem, the authors conducted what is called an “integrative data analysis” of randomized clinical trials of behavioral interventions for substance use that included self-identified Black participants and that measured cocaine use and/or opioid use outcomes. The authors searched the Clinical Trials Network database in 2021 and found 9 randomized clinical trials that met these criteria.
The analyses conducted by the researchers included 1,381 self-identifying Black adults enrolled in one of these 9 clinical trials with baseline cocaine and/or opioid use. The researchers wanted to determine whether psychosocial treatments were effective for Black participants enrolled in the study. The researchers categorized all interventions across the 9 studies into three groups: (1) social-contextual interventions (i.e., that address social and cognitive factors that underlie substance use disorder and recovery), (2) contingency management, and (3) treatment as usual/control. The researchers created 3 “latent” substance severity outcome scores: one for cocaine use outcomes, one for opioid use outcomes, and one for other substance outcomes. The researchers were able to extract data from each clinical trial at baseline, the end of treatment, and then 3-, 6-, 9-, and 12-months after the end of treatment. Because different trials used different substance use outcome measures, the researchers used statistical approaches to make outcomes comparable across studies. The researchers then used statistical analyses to determine how substance use outcomes changed over time separately for each type of treatment. The researchers compared outcomes across treatment groups.
The sample was, on average, 40 years old and 51.7% male. 56.2% of the sample was single or never married, and 75.5% had a high school degree or lower. The researchers evaluated whether there were demographic differences across treatment groups. Although most identified as only Black, 7.7% identified as multiracial Black. Only marital status differed, with 37% of participants in the contingency management group reporting that they are divorced compared to only 27.9% and 27.5% in the social-contextual interventions and the treatment as usual control groups. To account for this difference, the researchers used an approach called propensity score weighting to control for marital status to isolate the effect of condition (social-contextual interventions vs. contingency management vs. treatment as usual) on substance use outcomes.
WHAT DID THIS STUDY FIND?
Changes in cocaine use severity across treatment groups
Across all treatments, cocaine use disorder severity decreased from baseline to the end of treatment. Decreases in cocaine severity were the greatest for those in the social-contextual treatments and contingency management relative to treatment as usual (see graph below). At 12 months, reductions in cocaine use from baseline were observed for treatment as usual and social-contextual interventions. There was a small effect size difference between these two conditions, such that cocaine use severity among Black participants in social-contextual interventions was slightly lower (i.e., a better outcome). There were differences in 12-month cocaine use severity between both treatment as usual and social-contextual interventions and contingency management in cocaine use severity, with cocaine use severity in the contingency management condition returning to baseline levels of severity by the 12-month follow up.
Changes in opioid use severity across treatment groups
Across all treatments, opioid use severity decreased from baseline to the end of treatment. Decreases in opioid severity did not differ between the treatment conditions (see graph below). Opioid severity continued to decline across all treatment conditions through 12 months, and changes did not differ across different groups.
Changes in overall substance use severity across treatment groups
Overall substance use severity decreased from baseline to the end of treatment for those in the treatment as usual condition. Social-contextual treatments did not differ from treatment as usual in change in overall substance severity from baseline to end of treatment. However, contingency management showed significant decreases in overall substance use severity relative to treatment as usual. From the end of treatment to 12 months, participants in the treatment as usual and social-contextual interventions continued to decrease overall substance use severity. There was no difference in change between social-contextual interventions and treatment as usual. There were differences in 12-month cocaine use severity between both treatment as usual and social-contextual interventions and contingency management in overall substance use severity. Like with cocaine use, overall substance use severity in the contingency management condition returned to baseline levels of severity by the 12-month follow up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For cocaine use and general substance use, there was a slight advantage for social-contextual interventions over treatment as usual conditions, suggesting that interventions specifically targeting factors beyond substance use, such as those that also target trauma, social support, family relationships, or comorbid psychiatric conditions, might be slightly more useful in reducing cocaine use among Black people with cocaine use disorder. However, the effects were quite small, suggesting that the additional added benefit beyond treatment as usual is modest. This is not uncommon – treatment as usual, which in this study varied by trial, but usually included group therapy, individual therapy, and case management is often difficult to “beat” in clinical trials. This may be, in part, due to shared approaches across conditions (i.e., relapse prevention skills, referrals to mutual-help groups, etc.) and their ability to boost common therapeutic factors, like abstinence motivation and self-efficacy.
The study has two important caveats. First, the study did not define “benefit” from treatment for Black participants, but rather compared contingency management and a group of social-contextual treatments (e.g., cognitive-behavioral therapy) to treatment-as-usual, which differs by study but typically involves both individual and group therapies that help participants develop coping and other relapse prevention skills, and refers them to community resources like mutual-help groups (e.g., Alcoholics Anonymous). Because of the lack of definition specific to treatment “benefits”, all that can be said, ultimately, is that there appears to be at least some positive gains related to treatment effects for Black individuals. Second, perhaps an obvious question not addressed in this study, is whether Black individuals respond better or worse than other racial groups. Thus, although there was some improvement in this sample, it remains unclear whether Black patients respond differently somewhat limiting one’s ability to make recommendations for this understudied population of individuals with substance use disorder.
While contingency management was associated with decreases in cocaine, opioid, and overall substance use severity from baseline to the end of treatment, both cocaine use and overall substance use returned to pre-treatment levels. This suggests that contingency management did not have lasting effects for Black participants in these studies. Presumably, contingency management treatment effects were driven by the incentives used in this treatment approach which are removed after the course of treatment. As such, contingency management may be a useful approach for helping to reduce substance use initially, but additional approaches may be necessary to ensure such changes in substances remain beyond treatment.
Although opioid use decreased for all treatment groups, from baseline to end of treatment and through the 12-month follow up, there were no differences between treatment groups. Research has demonstrated that medications for opioid use disorder are consistently effective approaches for reducing opioid use disorder in the general population – with one exception, the treatment as usual conditions did not include medications for opioid use disorder. Importantly, other research shows Black individuals may be skeptical of opioid use disorder medications, due to past negative experiences with them and mistrust toward professional-medical approaches. As the study authors note, work may be necessary to culturally tailor psychosocial interventions to target unique issues facing black individuals (e.g., racial discrimination, etc.) in order to increase efficacy beyond treatment as usual.
The study did not compare outcomes to other racial groups, so it remains unclear whether Black participants response is better or worse than other racial groups. Also, there is no operational definition of treatment “benefit”, thus it remains unclear whether the magnitude of observed improvements in this study signify that Black patients actually “benefit” from treatment.
This study combined different treatments and compared against different control groups. Control conditions ranged from an informational pamphlet to assessment and referral to treatment, to group/individual offerings, ranging from 1-6 sessions. The relative difference between treatment as usual and the various active treatment conditions may differ depending on the comparison condition. However, this was not examined in the study.
BOTTOM LINE
For Black individuals, social-contextual interventions that target factors underlying substance use disorder and recovery (e.g., family relationships, social support, etc.) have a modest benefit over treatment as usual in reducing cocaine and general substance use, and the benefits persist after the end of treatment. Contingency management is associated with decreases in cocaine and general substance use during treatment, but these benefits are short-lived as substance use returns to pre-treatment levels after the treatment ends.
For individuals and families seeking recovery: If you are a person self-identifying as Black and you are seeking treatment for substance use disorder, you may be more likely to benefit from treatments that target both substances and other important factors such as trauma, family, or other conditions that commonly co-occur with substance use. Importantly, while contingency management may be beneficial during the treatment, it may be important to identify additional resources to maintain reductions after the treatment ends.
For treatment professionals and treatment systems: If you are a treatment provider, it may be important to use interventions that target social-contextual factors, such as family, trauma, or other co-occurring conditions, in addition to substance use when working with patients who are Black.
For scientists: There was some evidence that social-contextual treatments were more effective than control interventions at reducing cocaine use and overall substance use among Black participants. However, the benefits were modest. More research is needed to determine whether other treatments might be more effective for Black populations. Further, there have been recent calls for more culturally tailored interventions, which may be able to increase efficacy beyond that of interventions that are not culturally tailored. Finally, alternative approaches beyond traditional psychotherapy, such as mutual support groups or other recovery support services, are additional potential options that should be tested within Black populations to determine efficacy.
For policy makers: The current study was based on randomized clinical trials that tested interventions in Black populations; however, only nine trials met inclusion criteria. Policy that increases funding for clinical trials in diverse populations may increase the number of clinical trials available for this type of work and may ultimately improve our ability to answer questions about the efficacy of specific trials in specific populations.
Black Americans who use cocaine bear a disproportionate number of cocaine-related harms relative to other racial demographic groups. Though using comparable or lower amounts of cocaine, Black Americans experience higher rates of cocaine use disorder and have recently experienced greater rates of increase in cocaine-involved deaths. Though effective pharmacotherapeutic treatments for cocaine use remain elusive, there is strong evidence for the efficacy of psychosocial interventions such as contingency management and cognitive behavioral therapy. Most psychosocial treatments have been evaluated with disproportionately white samples, and it is unclear if such treatments are also useful for Black Americans.
HOW WAS THIS STUDY CONDUCTED?
To solve this problem, the authors conducted what is called an “integrative data analysis” of randomized clinical trials of behavioral interventions for substance use that included self-identified Black participants and that measured cocaine use and/or opioid use outcomes. The authors searched the Clinical Trials Network database in 2021 and found 9 randomized clinical trials that met these criteria.
The analyses conducted by the researchers included 1,381 self-identifying Black adults enrolled in one of these 9 clinical trials with baseline cocaine and/or opioid use. The researchers wanted to determine whether psychosocial treatments were effective for Black participants enrolled in the study. The researchers categorized all interventions across the 9 studies into three groups: (1) social-contextual interventions (i.e., that address social and cognitive factors that underlie substance use disorder and recovery), (2) contingency management, and (3) treatment as usual/control. The researchers created 3 “latent” substance severity outcome scores: one for cocaine use outcomes, one for opioid use outcomes, and one for other substance outcomes. The researchers were able to extract data from each clinical trial at baseline, the end of treatment, and then 3-, 6-, 9-, and 12-months after the end of treatment. Because different trials used different substance use outcome measures, the researchers used statistical approaches to make outcomes comparable across studies. The researchers then used statistical analyses to determine how substance use outcomes changed over time separately for each type of treatment. The researchers compared outcomes across treatment groups.
The sample was, on average, 40 years old and 51.7% male. 56.2% of the sample was single or never married, and 75.5% had a high school degree or lower. The researchers evaluated whether there were demographic differences across treatment groups. Although most identified as only Black, 7.7% identified as multiracial Black. Only marital status differed, with 37% of participants in the contingency management group reporting that they are divorced compared to only 27.9% and 27.5% in the social-contextual interventions and the treatment as usual control groups. To account for this difference, the researchers used an approach called propensity score weighting to control for marital status to isolate the effect of condition (social-contextual interventions vs. contingency management vs. treatment as usual) on substance use outcomes.
WHAT DID THIS STUDY FIND?
Changes in cocaine use severity across treatment groups
Across all treatments, cocaine use disorder severity decreased from baseline to the end of treatment. Decreases in cocaine severity were the greatest for those in the social-contextual treatments and contingency management relative to treatment as usual (see graph below). At 12 months, reductions in cocaine use from baseline were observed for treatment as usual and social-contextual interventions. There was a small effect size difference between these two conditions, such that cocaine use severity among Black participants in social-contextual interventions was slightly lower (i.e., a better outcome). There were differences in 12-month cocaine use severity between both treatment as usual and social-contextual interventions and contingency management in cocaine use severity, with cocaine use severity in the contingency management condition returning to baseline levels of severity by the 12-month follow up.
Changes in opioid use severity across treatment groups
Across all treatments, opioid use severity decreased from baseline to the end of treatment. Decreases in opioid severity did not differ between the treatment conditions (see graph below). Opioid severity continued to decline across all treatment conditions through 12 months, and changes did not differ across different groups.
Changes in overall substance use severity across treatment groups
Overall substance use severity decreased from baseline to the end of treatment for those in the treatment as usual condition. Social-contextual treatments did not differ from treatment as usual in change in overall substance severity from baseline to end of treatment. However, contingency management showed significant decreases in overall substance use severity relative to treatment as usual. From the end of treatment to 12 months, participants in the treatment as usual and social-contextual interventions continued to decrease overall substance use severity. There was no difference in change between social-contextual interventions and treatment as usual. There were differences in 12-month cocaine use severity between both treatment as usual and social-contextual interventions and contingency management in overall substance use severity. Like with cocaine use, overall substance use severity in the contingency management condition returned to baseline levels of severity by the 12-month follow up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For cocaine use and general substance use, there was a slight advantage for social-contextual interventions over treatment as usual conditions, suggesting that interventions specifically targeting factors beyond substance use, such as those that also target trauma, social support, family relationships, or comorbid psychiatric conditions, might be slightly more useful in reducing cocaine use among Black people with cocaine use disorder. However, the effects were quite small, suggesting that the additional added benefit beyond treatment as usual is modest. This is not uncommon – treatment as usual, which in this study varied by trial, but usually included group therapy, individual therapy, and case management is often difficult to “beat” in clinical trials. This may be, in part, due to shared approaches across conditions (i.e., relapse prevention skills, referrals to mutual-help groups, etc.) and their ability to boost common therapeutic factors, like abstinence motivation and self-efficacy.
The study has two important caveats. First, the study did not define “benefit” from treatment for Black participants, but rather compared contingency management and a group of social-contextual treatments (e.g., cognitive-behavioral therapy) to treatment-as-usual, which differs by study but typically involves both individual and group therapies that help participants develop coping and other relapse prevention skills, and refers them to community resources like mutual-help groups (e.g., Alcoholics Anonymous). Because of the lack of definition specific to treatment “benefits”, all that can be said, ultimately, is that there appears to be at least some positive gains related to treatment effects for Black individuals. Second, perhaps an obvious question not addressed in this study, is whether Black individuals respond better or worse than other racial groups. Thus, although there was some improvement in this sample, it remains unclear whether Black patients respond differently somewhat limiting one’s ability to make recommendations for this understudied population of individuals with substance use disorder.
While contingency management was associated with decreases in cocaine, opioid, and overall substance use severity from baseline to the end of treatment, both cocaine use and overall substance use returned to pre-treatment levels. This suggests that contingency management did not have lasting effects for Black participants in these studies. Presumably, contingency management treatment effects were driven by the incentives used in this treatment approach which are removed after the course of treatment. As such, contingency management may be a useful approach for helping to reduce substance use initially, but additional approaches may be necessary to ensure such changes in substances remain beyond treatment.
Although opioid use decreased for all treatment groups, from baseline to end of treatment and through the 12-month follow up, there were no differences between treatment groups. Research has demonstrated that medications for opioid use disorder are consistently effective approaches for reducing opioid use disorder in the general population – with one exception, the treatment as usual conditions did not include medications for opioid use disorder. Importantly, other research shows Black individuals may be skeptical of opioid use disorder medications, due to past negative experiences with them and mistrust toward professional-medical approaches. As the study authors note, work may be necessary to culturally tailor psychosocial interventions to target unique issues facing black individuals (e.g., racial discrimination, etc.) in order to increase efficacy beyond treatment as usual.
The study did not compare outcomes to other racial groups, so it remains unclear whether Black participants response is better or worse than other racial groups. Also, there is no operational definition of treatment “benefit”, thus it remains unclear whether the magnitude of observed improvements in this study signify that Black patients actually “benefit” from treatment.
This study combined different treatments and compared against different control groups. Control conditions ranged from an informational pamphlet to assessment and referral to treatment, to group/individual offerings, ranging from 1-6 sessions. The relative difference between treatment as usual and the various active treatment conditions may differ depending on the comparison condition. However, this was not examined in the study.
BOTTOM LINE
For Black individuals, social-contextual interventions that target factors underlying substance use disorder and recovery (e.g., family relationships, social support, etc.) have a modest benefit over treatment as usual in reducing cocaine and general substance use, and the benefits persist after the end of treatment. Contingency management is associated with decreases in cocaine and general substance use during treatment, but these benefits are short-lived as substance use returns to pre-treatment levels after the treatment ends.
For individuals and families seeking recovery: If you are a person self-identifying as Black and you are seeking treatment for substance use disorder, you may be more likely to benefit from treatments that target both substances and other important factors such as trauma, family, or other conditions that commonly co-occur with substance use. Importantly, while contingency management may be beneficial during the treatment, it may be important to identify additional resources to maintain reductions after the treatment ends.
For treatment professionals and treatment systems: If you are a treatment provider, it may be important to use interventions that target social-contextual factors, such as family, trauma, or other co-occurring conditions, in addition to substance use when working with patients who are Black.
For scientists: There was some evidence that social-contextual treatments were more effective than control interventions at reducing cocaine use and overall substance use among Black participants. However, the benefits were modest. More research is needed to determine whether other treatments might be more effective for Black populations. Further, there have been recent calls for more culturally tailored interventions, which may be able to increase efficacy beyond that of interventions that are not culturally tailored. Finally, alternative approaches beyond traditional psychotherapy, such as mutual support groups or other recovery support services, are additional potential options that should be tested within Black populations to determine efficacy.
For policy makers: The current study was based on randomized clinical trials that tested interventions in Black populations; however, only nine trials met inclusion criteria. Policy that increases funding for clinical trials in diverse populations may increase the number of clinical trials available for this type of work and may ultimately improve our ability to answer questions about the efficacy of specific trials in specific populations.