
Network Support: Effectiveness of Treatment that Connects Patients to Recovery Social Supports
Prior research has shown Network Support, a treatment designed to increase individuals’ support for recovery and decrease their support for drinking, provides recovery benefit.
How did it fare against a well-known, evidence-based cognitive-behavioral treatment?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
An individual’s social circle, also called a social network, can serve as a major foundation to help reduce relapse risk for those that are in, or are seeking, recovery from alcohol and other drug use disorder.
For example, if these social network members are in recovery themselves, they may be able to serve as recovery role models helping individuals cope with increased stress, instilling confidence that challenging situations can be handled effectively (i.e., self-efficacy), and increasing one’s recovery motivation by responding positively to recovery-related actions.
In line with this, Litt and colleagues showed that an intervention called Network Support, which is designed to increase recovery supportive people in one’s network and decrease drinking-supportive individuals, led to 20% more percent days abstinent across 2 years compared to a case management intervention which helped participants set goals and provided information regarding professional and community resources to meet those goals.
In the current study, the authors compared recovery benefits of this Network Support intervention to a cognitive behavioral therapy (CBT) intervention, a more active intervention than case management that has a strong scientific evidence base and is commonly delivered in treatment settings.
HOW WAS THIS STUDY CONDUCTED?
It is important to first outline the content of both treatments:
1.NETWORK SUPPORT
Therapists leveraged the existing recovery-supportive communities within Alcoholics Anonymous (AA) to help participants increase the recovery support in their network. In this study, the treatment emphasized the social aspects of AA and recognized, but downplayed its spiritual content.
In addition, Network Support also highlighted other ways by which participants could increase recovery support and decrease drinking support in their network because their prior work showed that many individuals were very resistant or unwilling to attend AA. These additional strategies included social and recreational activities that would expose them to individuals that were either recovery supportive, or at a minimum not drinking-supportive. One major difference between this version of Network Support compared to the one from the original study was the inclusion of a social skills training module to help individuals engage in these new social activities.
2.COGNITIVE BEHAVIORAL THERAPY (CBT)
Cognitive behavioral therapy (CBT) in this study was based on other CBT approaches that had been vetted in prior studies. These CBT approaches are intended to help individuals identify and avoid high-risk situations, as well as to increase their coping skills to manage cravings that might result from exposure to these high risk situations if they cannot or will not avoid them. Both Network Support and CBT consisted of 12 weekly outpatient sessions that lasted 60 minutes each.
Regarding study design, authors randomly assigned 96 adults with alcohol use disorder to Network Support and 97 to cognitive behavioral therapy (CBT), assessing participants after the treatments were delivered (post-treatment), and every 3 months thereafter up through 24-month follow-up (i.e., 27 months after they entered the study). Those with other drug use disorders apart from marijuana and those with more extensive AA experience (attending 4 or more meetings in the month before entering the study) were excluded from participating.
The treatments were compared on percent days abstinent from alcohol, as well as percent days with heavy drinking (four or more drinks for a woman and five or more for a man in one day), number of drinks per drinking day, complete abstinence, and drinking-related consequences (i.e., effects on one’s social life, employment, and health). Authors also investigated what processes during treatment explained any differences between Network Support and cognitive behavioral therapy (CBT) over time.
- PARTICIPANT DEMOGRAPHICS
-
- Participants were 46 years old, on average, and 66% were Male while 93% were White.
- The average participant had one prior episode of alcohol use disorder treatment in their lifetime, had been to one AA meeting in the past 90 days, and drank on 69 of the past 90 days with about 9 drinks each day.
- Controlled or moderate drinking was the goal for 30%, while abstinence the goal for 70%.
- Participants in Network Support and cognitive behavioral therapy (CBT) were essentially equivalent on all measured demographic and drinking-related characteristics when entering the study.
WHAT DID THIS STUDY FIND?
The two treatments had similar rates of attendance with each group attending about 7 sessions on average.
As the authors predicted, Network Support participants had more percent days abstinent over time than cognitive behavioral therapy (CBT).
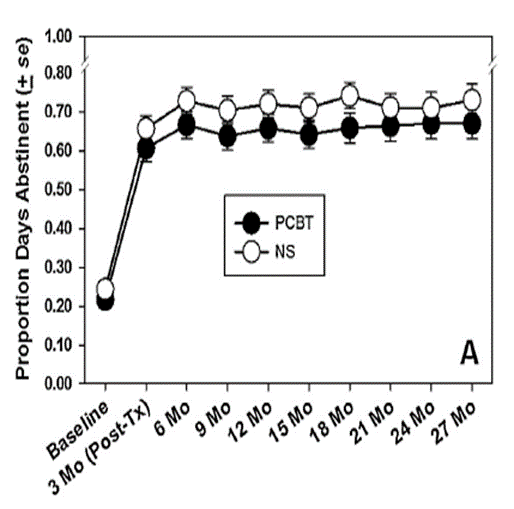
Adapted from McCutcheon et al. (2016).
Participants increased their percent days abstinent in the past 90 days from about 20% in both groups upon entering the study, to about 70% in Network Support vs. 65% in cognitive behavioral therapy (CBT) across 2 years after receiving the treatment. The Network Support participants also had fewer drinking consequences, on average, while percent days heavy drinking and number drinks per drinking day were similar. Complete abstinence overall was statistically similar for the groups (i.e., there was not a statistically reliable difference over time).
The proportion of Network Support participants that were completely abstinent during an assessment period lasting 90 days was consistently higher in Network Support than cognitive behavioral therapy (CBT) with the lone exception of immediately following treatment.
For example, 35% of participants in Network Support were completely abstinent for 90 days compared to only 20% for cognitive behavioral therapy (CBT) at the 12-month follow-up. Also as the authors predicted, the small but statistically reliable advantage for Network Support was explained, in part, by an increase in the number of abstinent individuals in one’s close social circle, AA meeting attendance, and abstinence self-efficacy.
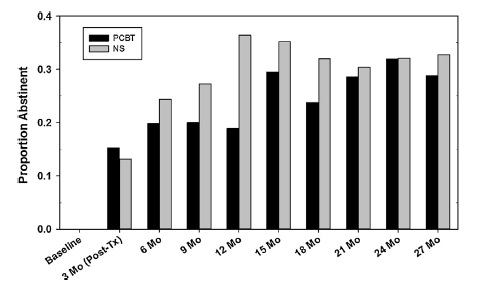
NOTE*** NS = Network Support; PCBT = Cognitive Behavioral Therapy; Post-Tx = Post-Treatment
It is important to note that adopting abstinent individuals into their network through AA, specifically, did not provide additional recovery benefit in comparison to adopting abstinent individuals into their network by other strategies.
Also, about half of the Network Support group, and 60% of the cognitive behavioral therapy (CBT) group never attended AA during the entire 27-month study period (3-month treatment and 2-year follow-up). Put another way, this also demonstrates that despite not being explicitly encouraged to attend AA in the CBT condition, almost as many patients in the CBT condition (40%) as the Network Support condition (50%) chose to attend AA during the follow-up period.
WHY IS THIS STUDY IMPORTANT?
This study shows that specific treatments like Network Support can help individuals make changes to their social network, changes important to initiating & sustaining abstinence, by growing that network of abstinent individuals.
In other studies, like this one by Kelly and colleagues, it has been shown that decreasing the number of individuals that are heavy drinkers or who support someone’s drinking also provides benefit. Network Support and cognitive behavioral therapy (CBT) provided similar benefit in this area.
Another important finding was the lower drinking consequences for those in Network Support despite similar rates of heavy drinking and number of drinks on each drinking day.
It could be that on days where individuals drink, networks that strongly support abstinence and recovery can help buffer against consequences, serving as a base to use coping skills and providing individuals with the support and confidence needed to get back on track after a heavy drinking episode.
One critical finding was that half of the Network Support group did not attend AA at all during the study period, despite specific encouragement and support to do so.
This may have been because of the lower severity of the group’s alcohol problems compared to those who attend residential treatment. Only 70% were interested in an abstinence goal, which may have turned them off to AA, which explicitly encourages abstinence as a solution to alcohol use disorder.
Dozens of studies following individuals in treatment over time have shown that those who are more severe, and have more psychosocial difficulties, are more likely to attend AA and other 12-step mutual-help organizations.
It is encouraging that increasing abstinent individuals in one’s network by any means, including but not limited to AA, provided recovery benefit, and that such changes can be facilitated in treatment.
- LIMITATIONS
-
- The focus on the study was individuals whose primary problem was alcohol. People with drug use disorders apart from alcohol and marijuana were excluded. So it is unclear if these findings also apply to individuals that have opioid, cocaine, and amphetamine use disorders, for example.
NEXT STEPS
One possible next step is to implement this treatment with a broader patient population in real-world treatment settings. For example, it will be important to see whether Network Support is effective for individuals with primary alcohol problems that also have opioid, cocaine, and/or amphetamine use disorders, as these individuals were excluded from the current study.
In addition, it will also be important to see if an adapted version of Network Support is effective for those whose primary substance is an illicit drug, such as opioids. This version of Network Support could aim to leverage the recovery-supportive social networks present in the related 12-step mutual-help group Narcotics Anonymous rather than AA, given its broader focus on all drugs.
BOTTOM LINE
- For individuals & families seeking recovery: Making changes to one’s social circle – especially adding individuals who are abstinent or in recovery themselves – is likely to increase one’s chances of initiating and sustaining abstinence over time. Therefore, treatments that help individuals do this, like Network Support, are likely to offer greater recovery benefit.
- For Scientists: This study used a rigorous design to show that Network Support provides similar or greater recovery benefit than cognitive behavioral therapy (CBT) across a range of outcomes. Their mediation analyses offer a nice example for other clinical research, as authors also showed that Network Support worked, in part, through processes they predicted a priori (e.g., increasing number of abstinent individuals in one’s network, AA meetings, and abstinence self-efficacy).
- For Policy makers: This is the second controlled study showing that Network Support provides benefit for abstinence and other recovery outcomes. Strongly consider funding for research to test its recovery benefit in real world settings.
- For Treatment professionals and treatment systems: Interventions that target social network changes are likely to help your patients. Although research in real world treatment settings is needed before a recommendation to roll Network Support out on a large scale can be made, results to this point are positive, and suggest it is likely to provide an advantage relative to case management and cognitive behavioral therapy (CBT).
CITATIONS
Litt, M. D., Kadden, R. M., Tennen, H., & Kabela-Cormier, E. (2016). Network Support II: Randomized controlled trial of Network Support treatment and cognitive behavioral therapy for alcohol use disorder. Drug Alcohol Depend. doi:10.1016/j.drugalcdep.2016.06.010
