“Modest but Mighty”: Rural recovery community center’s characteristics, barriers, and solutions
Nearly 20% of the US population, about 65 million people, live in rural areas. People with substance use disorder in these communities face distinct challenges and often rely on creative, community-based solutions. Despite this, the structure, reach, and functioning of rural recovery community organizations remain largely unexamined. This study addresses that gap by surveying and interviewing directors of 12 rural recovery community centers in Georgia, offering insights into their strengths, challenges, and roles in supporting recovery.
Under the Federal Office of Rural Health Policy’s definition of rurality, 19% of the US population, or about 65 million people, live in rural areas (i.e., defined as non-metro counties, or areas within metro counties of a certain size that have low population density, or areas where the commuting flow is not to an urban core, etc.). Individuals in or seeking substance use disorder recovery in these communities face distinct challenges related to geography, service access, and social determinants of health, often requiring creative, community-based solutions. Understanding how recovery support systems respond to urban–rural differences remains critical. Recovery community centers are a growing component of recovery support services, yet little is known about how these organizations operate in rural contexts or how they address the unique needs of rural communities.
Recovery community centers are locally embedded, nonprofit organizations that support people working toward or maintaining recovery outside of formal treatment settings. Rather than providing clinical care, these “hubs” emphasize connection, peer leadership, and practical problem-solving. Many are organized and staffed by people with lived experience and serve as gathering places where individuals can access peer support, attend recovery meetings, participate in social activities, and get linkages to available community resources. Beyond emotional and social support, recovery community centers often help participants navigate everyday barriers to stability, including job searches, paperwork, and access to health coverage. Evidence from administrative data suggests that deeper involvement with these centers is linked to stronger recovery-related resources (i.e., recovery capital). Despite their growing presence, research has rarely examined how these organizations function across different geographic contexts, particularly in rural areas. The current study addresses this gap by examining rural recovery community centers in Georgia.
HOW WAS THIS STUDY CONDUCTED?
Working in partnership with the Georgia Council for Recovery, the study team identified 13 rural recovery community centers actively operating in Georgia. Directors from each center were invited to complete a brief survey about their backgrounds and organizational characteristics, as well as participate in a virtual interview exploring how their centers support individuals with substance use disorders broadly and those receiving medications for opioid use disorder specifically.
There were 12 directors that participated, although 1 left more than 50% of their survey blank, which resulted in their survey being excluded from descriptive analyses. Most directors identified as White and had lived experience of recovery, though a minority represented other racial backgrounds or did not have personal recovery experience. The sample included 8 women and 4 men, with an average age of 42 and approximately 6 years of professional experience in the addiction field. Half of the directors were raised in rural communities, one quarter held at least a bachelor’s degree, and three quarters identified as Christian.
WHAT DID THIS STUDY FIND?
“Modest but Mighty”: Rural recovery community centers were modest but mighty resource hubs
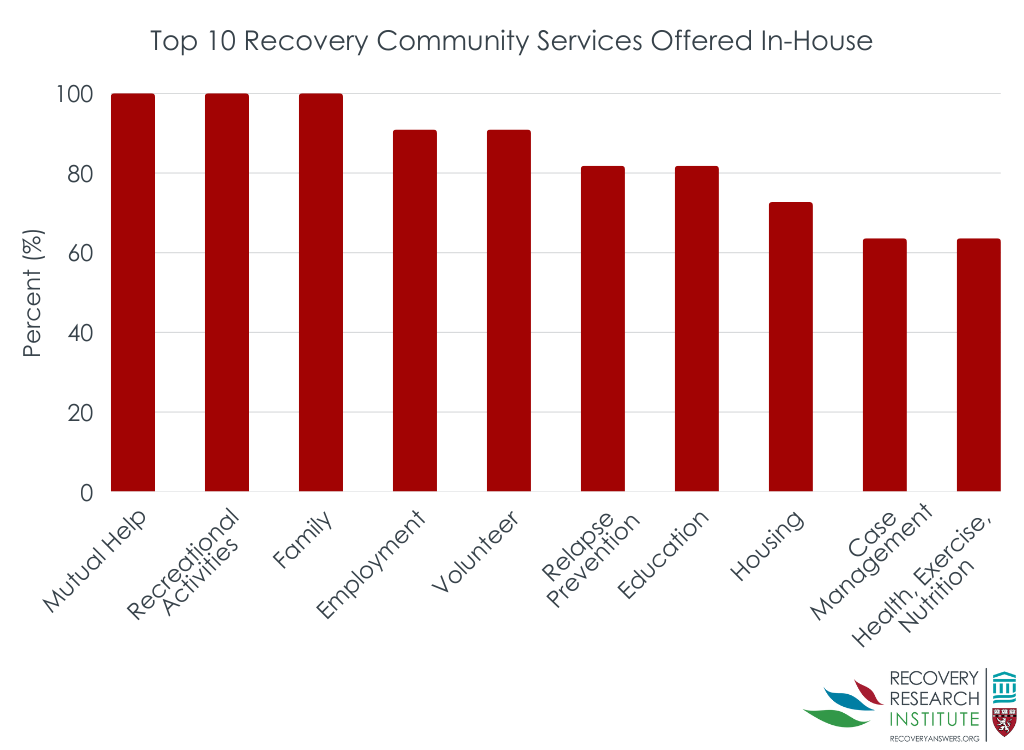
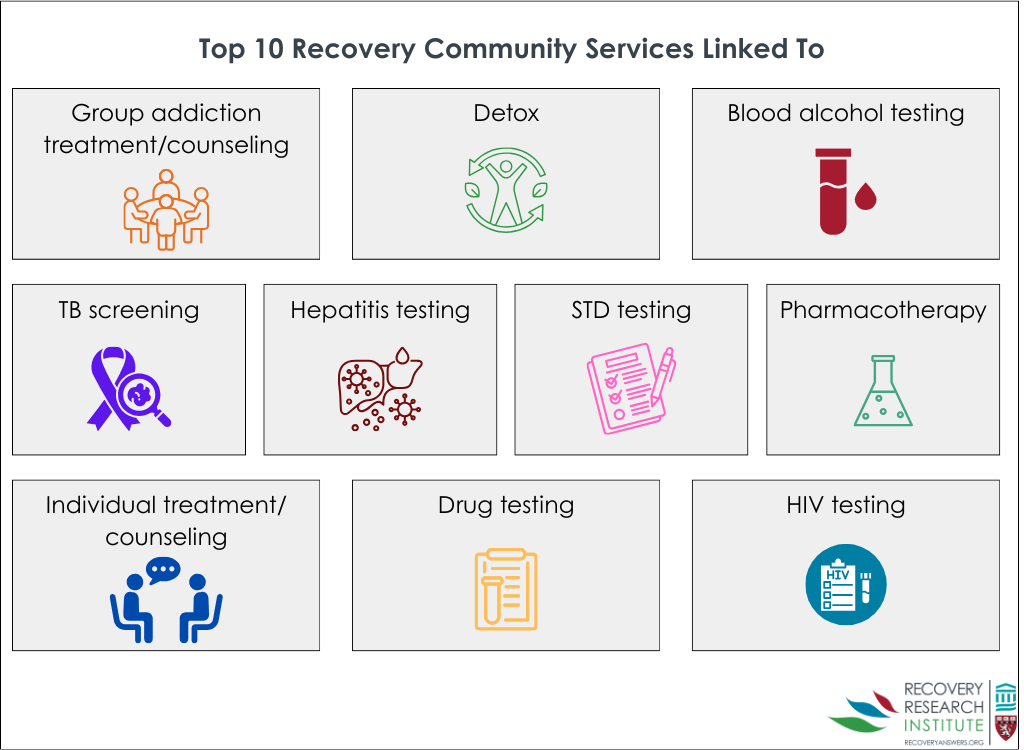
These centers had a modest annual average budget of $225,407. They served, on average, 468 people each month, with 41 of them being new. They had an average of 5 paid staff, but that ranged from 1-9. There were also about 7 volunteer staff on average. The directors also reported the in-house services their center provides (see graph below) and the services they link to (see graphic below).
Rural recovery community center participants had a range of backgrounds and identities
According to directors’ estimates, individuals served by rural recovery community centers entered services through multiple pathways, most commonly from formal treatment programs (34%), followed by self-referral (28%), and referrals from the legal system (25%). Most participants were adults between the ages of 25 and 59 (68%), with very few under the age of 18 (3%). Participants were more often male (56%), and a substantial proportion were currently involved in the legal system (61%). Educational attainment was generally low, with 39% of participants lacking a high school diploma, though nearly half were employed full time (44%). Racially, most participants were White (60%), while more than one quarter were Black (27%). In terms of recovery status, over half of participants were within their first year of recovery (58%), and a smaller subset were actively using substances (7%). Amphetamines were the most cited primary substance of choice (28%), followed by alcohol (24%), opioids (21%), cannabis (10%), cocaine (7%), and benzodiazepines (5%).
Transportation and housing were common challenges
Most rural recovery community center directors reported transportation as their single greatest challenge. One director shared:
“We have recovery options and can help people get to them, but with rural areas, everything is so spread out. There may be resources in our region, but the region is so large that people can’t necessarily access them…Without us providing transportation, people wouldn’t be able to get there.”
The directors reported a range of strategies that they use to address challenges. For transportation, some recovery community centers owned their own vehicles, and others dedicated volunteer and staff hours, along with their personal vehicles, to transportation. Some centers developed partnerships to help facilitate transportation and rideshare options.
Housing was the second most reported challenge. Affordable housing, recovery housing, and shelters for people experiencing homeless were all noted to be lacking. Directors also mentioned unique housing barriers related to people with substance use histories such as upfront costs (e.g., rent deposits), poor credit scores, and criminal backgrounds. To address some of the housing challenges, directors developed partnerships with local property owners to identify available housing, and some directors used center funds to cover the upfront financial costs of some housing options.
Directors also brought up other challenges their centers and participants faced such as limited resources, lack of gainful employment, health insurance access (Georgia did not expand Medicaid to cover those with low income), lack of affordable childcare, unmet basic needs, and community stigma.
Here directors highlighted partnerships with recovery-friendly employers as well as employment support, which included resume building services, physical space to apply for jobs and conduct virtual interviews, and a clothing closet for job interviews. Connections to GED programs and in-house access to computers were also mentioned in response to the education barriers. Some centers made food and hygiene products available in house, and a few even provided funds to participants for groceries and utility bills.
Community collaborations were key for rural recovery community centers
All of the center directors focused on community collaborations and engagement to enhance their services and address the barriers their participants face. One directed even noted, “My theme has been putting the ‘C’ back in [Recovery Community Organization].”
The intentional and coordinated community collaborations featured a variety of other organizations. All of the directors collaborated with local substance use disorder treatment services, including detox facilities, and office-based buprenorphine treatment providers. They all also noted their connections with social services (e.g., child welfare, shelters, local nonprofits). Several directors even mentioned that they sit on the board of directors for other nonprofit organizations. Most of the directors discussed how they worked with the criminal legal system.
That said, connections to opioid use disorder medication providers was minimal. Rural recovery community centers provide critical linkages and services
Rural recovery community centers were instrumental helping people access treatment.
Through their community partners, local embeddedness, and unique skills, recovery community center staff were able to help participants enroll in Medicaid and identify opening at state-funded treatment services:
In addition to connections to treatment and recovery services, rural community centers were often the primary or only naloxone distributor. Naloxone is an opioid antagonist that works by blocking opioid receptors in the brain, which can reverse an opioid overdose, and is often known by its brand name, Narcan. One director underscored how availability of naloxone would drop without them by sharing, “Many organizations, schools, police departments, and others rely on us to provide [naloxone].”
Rural recovery community centers also helped increase the variety and access of mutual-help organizations. This included recovery pathways not as common in rural areas such as Celebrate Recovery, All Recovery, SMART Recovery, and Yoga Recovery. In addition to 12-step meetings (e.g., Alcoholics Anonymous), they featured meetings for identity groups such as sexual and gender minorities, veterans, family members of people with substance use disorder, people receiving medications for opioid use disorder, and those with co-occurring mental health conditions.
Rural recovery community center directors highlighted that mutual-help organization meetings and one-on-one peer support as the most important services provided in-house. One-on-one peer support (i.e., recovery coaching) featured structured sessions and regular check-ins. One director described it as:
“The peer walks us through their life and identifies what they need to improve. We then set goals to help them get there…we lift the peer’s voice and focus on what’s going right in their life. We create a safe space where they can celebrate their strengths and build on them.”
Another shared:
“We take a strengths-based approach, talking about what’s going well in their life. It’s all about starting with a positive focus, and that’s how we engage with everyone who comes through.”
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Recovery community centers serve as hubs for recovery support and as important connectors to health and social services within their communities, with prior research demonstrating their potential to enhance recovery capital among participants. However, much of the existing literature has focused almost exclusively on urban and suburban centers. Given the distinct challenges and strengths of rural communities, understanding how rural recovery community centers both align with and diverge from their urban counterparts is critical. Although this study did not directly compare the two types of geographies, this study features several points of convergence and divergence between 12 rural recovery community centers and previously studied urban and suburban models.
Rural recovery community centers operate in resource-constrained environments and, according to director surveys and interviews, primarily serve individuals in early recovery while assuming an expanded role in treatment linkage as well as reducing the harms of substance use. Many of the rural centers described in this study functioned as the primary naloxone provider in their communities, with one director noting distribution to schools, police departments, and other local organizations. At the same time, these centers face challenges tied to rural geography. Transportation and housing were consistently identified as major barriers, and while some centers collaborated with community partners to arrange rides or identify housing options, directors reported ongoing difficulty addressing these and other social determinants of health. Directors also noted limited collaboration with providers of medications for opioid use disorder, despite repeated efforts to establish these partnerships. Rural recovery community centers may be addressing significant gaps in the continuum of care beyond supporting individuals already in or pursing their recovery. More research is needed to identify how rural recovery community centers may leverage their strengths to address their unique challenges.
This study included rural recovery community centers from one southeastern state, Georgia. Thus, the findings may be a result of contextual factors (e.g., health insurance provision, social and cultural norms, state-specific funding allocations) that may differ in other states.
Directors reported their participants’ demographics. It is possible that directors do not recall or track their participant demographics accurately.
BOTTOM LINE
Recovery community centers serve as important resource hubs for individuals in recovery, particularly those with low levels of recovery capital and few resources and who also have severe, complex, and chronic clinical histories. Findings from this study suggest that rural recovery community centers may play an even broader role, extending support beyond those in recovery by providing critical services that reduce the harms of substance use and facilitating linkage to treatment. In rural settings, these centers may also represent one of the few accessible entry points for historically marginalized groups, such as sexual and gender minorities, and for individuals pursuing non–12-step recovery pathways to engage in mutual-help meetings and peer-to-peer support. Given the range of services they offer, rural recovery community centers may be a key component of a national comprehensive response to the needs of people who use substances and those pursuing recovery. Additional research is needed to better understand how to strengthen and sustain these centers, particularly in rural communities.
For individuals and families seeking recovery: If you or a loved one is interested in changing your substance use, pursuing treatment, or exploring different recovery pathways, it could be very helpful to connect with a local recovery community center. Experts at these centers may be able to help you meet your goals and connect you with important services in your community including mental health counseling, job skills training, transportation supports, and many more.
For treatment professionals and treatment systems: Connecting individuals to community-based supports and resources is essential for building recovery capital and supporting goal attainment. Treatment professionals and systems should not only be aware of recovery community centers in their area, but also actively facilitate referrals to and collaborations with these centers. At the same time, it is important to recognize individual differences in needs and recovery goals, as not all patients will benefit from the same types of programming or center offerings.
For scientists: Additional research is needed to better understand the diverse ways recovery community centers support their communities and navigate structural and contextual challenges. This study drew on surveys and interviews with directors from 12 rural recovery community centers in Georgia; future work could expand the sample to include both rural and urban centers, enabling more direct comparisons across geographic contexts. Further research would also benefit from incorporating the perspectives and self-identified characteristics of center participants. Finally, supporting centers in the collection of non-intrusive, ethically appropriate data would help advance understanding of the individual- and community-level impacts of recovery community centers.
For policy makers: Comprehensive, systematic, and longitudinal research is needed to better understand how recovery community centers influence both individual participants and the broader communities they serve. This study highlights the distinct barriers rural recovery community centers face, as well as the strategies they employ to address them. Continued investment in research and funding will be essential to sustain these centers and deepen understanding of their role within recovery-oriented systems of care.
Under the Federal Office of Rural Health Policy’s definition of rurality, 19% of the US population, or about 65 million people, live in rural areas (i.e., defined as non-metro counties, or areas within metro counties of a certain size that have low population density, or areas where the commuting flow is not to an urban core, etc.). Individuals in or seeking substance use disorder recovery in these communities face distinct challenges related to geography, service access, and social determinants of health, often requiring creative, community-based solutions. Understanding how recovery support systems respond to urban–rural differences remains critical. Recovery community centers are a growing component of recovery support services, yet little is known about how these organizations operate in rural contexts or how they address the unique needs of rural communities.
Recovery community centers are locally embedded, nonprofit organizations that support people working toward or maintaining recovery outside of formal treatment settings. Rather than providing clinical care, these “hubs” emphasize connection, peer leadership, and practical problem-solving. Many are organized and staffed by people with lived experience and serve as gathering places where individuals can access peer support, attend recovery meetings, participate in social activities, and get linkages to available community resources. Beyond emotional and social support, recovery community centers often help participants navigate everyday barriers to stability, including job searches, paperwork, and access to health coverage. Evidence from administrative data suggests that deeper involvement with these centers is linked to stronger recovery-related resources (i.e., recovery capital). Despite their growing presence, research has rarely examined how these organizations function across different geographic contexts, particularly in rural areas. The current study addresses this gap by examining rural recovery community centers in Georgia.
HOW WAS THIS STUDY CONDUCTED?
Working in partnership with the Georgia Council for Recovery, the study team identified 13 rural recovery community centers actively operating in Georgia. Directors from each center were invited to complete a brief survey about their backgrounds and organizational characteristics, as well as participate in a virtual interview exploring how their centers support individuals with substance use disorders broadly and those receiving medications for opioid use disorder specifically.
There were 12 directors that participated, although 1 left more than 50% of their survey blank, which resulted in their survey being excluded from descriptive analyses. Most directors identified as White and had lived experience of recovery, though a minority represented other racial backgrounds or did not have personal recovery experience. The sample included 8 women and 4 men, with an average age of 42 and approximately 6 years of professional experience in the addiction field. Half of the directors were raised in rural communities, one quarter held at least a bachelor’s degree, and three quarters identified as Christian.
WHAT DID THIS STUDY FIND?
“Modest but Mighty”: Rural recovery community centers were modest but mighty resource hubs
These centers had a modest annual average budget of $225,407. They served, on average, 468 people each month, with 41 of them being new. They had an average of 5 paid staff, but that ranged from 1-9. There were also about 7 volunteer staff on average. The directors also reported the in-house services their center provides (see graph below) and the services they link to (see graphic below).
Rural recovery community center participants had a range of backgrounds and identities
According to directors’ estimates, individuals served by rural recovery community centers entered services through multiple pathways, most commonly from formal treatment programs (34%), followed by self-referral (28%), and referrals from the legal system (25%). Most participants were adults between the ages of 25 and 59 (68%), with very few under the age of 18 (3%). Participants were more often male (56%), and a substantial proportion were currently involved in the legal system (61%). Educational attainment was generally low, with 39% of participants lacking a high school diploma, though nearly half were employed full time (44%). Racially, most participants were White (60%), while more than one quarter were Black (27%). In terms of recovery status, over half of participants were within their first year of recovery (58%), and a smaller subset were actively using substances (7%). Amphetamines were the most cited primary substance of choice (28%), followed by alcohol (24%), opioids (21%), cannabis (10%), cocaine (7%), and benzodiazepines (5%).
Transportation and housing were common challenges
Most rural recovery community center directors reported transportation as their single greatest challenge. One director shared:
“We have recovery options and can help people get to them, but with rural areas, everything is so spread out. There may be resources in our region, but the region is so large that people can’t necessarily access them…Without us providing transportation, people wouldn’t be able to get there.”
The directors reported a range of strategies that they use to address challenges. For transportation, some recovery community centers owned their own vehicles, and others dedicated volunteer and staff hours, along with their personal vehicles, to transportation. Some centers developed partnerships to help facilitate transportation and rideshare options.
Housing was the second most reported challenge. Affordable housing, recovery housing, and shelters for people experiencing homeless were all noted to be lacking. Directors also mentioned unique housing barriers related to people with substance use histories such as upfront costs (e.g., rent deposits), poor credit scores, and criminal backgrounds. To address some of the housing challenges, directors developed partnerships with local property owners to identify available housing, and some directors used center funds to cover the upfront financial costs of some housing options.
Directors also brought up other challenges their centers and participants faced such as limited resources, lack of gainful employment, health insurance access (Georgia did not expand Medicaid to cover those with low income), lack of affordable childcare, unmet basic needs, and community stigma.
Here directors highlighted partnerships with recovery-friendly employers as well as employment support, which included resume building services, physical space to apply for jobs and conduct virtual interviews, and a clothing closet for job interviews. Connections to GED programs and in-house access to computers were also mentioned in response to the education barriers. Some centers made food and hygiene products available in house, and a few even provided funds to participants for groceries and utility bills.
Community collaborations were key for rural recovery community centers
All of the center directors focused on community collaborations and engagement to enhance their services and address the barriers their participants face. One directed even noted, “My theme has been putting the ‘C’ back in [Recovery Community Organization].”
The intentional and coordinated community collaborations featured a variety of other organizations. All of the directors collaborated with local substance use disorder treatment services, including detox facilities, and office-based buprenorphine treatment providers. They all also noted their connections with social services (e.g., child welfare, shelters, local nonprofits). Several directors even mentioned that they sit on the board of directors for other nonprofit organizations. Most of the directors discussed how they worked with the criminal legal system.
That said, connections to opioid use disorder medication providers was minimal. Rural recovery community centers provide critical linkages and services
Rural recovery community centers were instrumental helping people access treatment.
Through their community partners, local embeddedness, and unique skills, recovery community center staff were able to help participants enroll in Medicaid and identify opening at state-funded treatment services:
In addition to connections to treatment and recovery services, rural community centers were often the primary or only naloxone distributor. Naloxone is an opioid antagonist that works by blocking opioid receptors in the brain, which can reverse an opioid overdose, and is often known by its brand name, Narcan. One director underscored how availability of naloxone would drop without them by sharing, “Many organizations, schools, police departments, and others rely on us to provide [naloxone].”
Rural recovery community centers also helped increase the variety and access of mutual-help organizations. This included recovery pathways not as common in rural areas such as Celebrate Recovery, All Recovery, SMART Recovery, and Yoga Recovery. In addition to 12-step meetings (e.g., Alcoholics Anonymous), they featured meetings for identity groups such as sexual and gender minorities, veterans, family members of people with substance use disorder, people receiving medications for opioid use disorder, and those with co-occurring mental health conditions.
Rural recovery community center directors highlighted that mutual-help organization meetings and one-on-one peer support as the most important services provided in-house. One-on-one peer support (i.e., recovery coaching) featured structured sessions and regular check-ins. One director described it as:
“The peer walks us through their life and identifies what they need to improve. We then set goals to help them get there…we lift the peer’s voice and focus on what’s going right in their life. We create a safe space where they can celebrate their strengths and build on them.”
Another shared:
“We take a strengths-based approach, talking about what’s going well in their life. It’s all about starting with a positive focus, and that’s how we engage with everyone who comes through.”
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Recovery community centers serve as hubs for recovery support and as important connectors to health and social services within their communities, with prior research demonstrating their potential to enhance recovery capital among participants. However, much of the existing literature has focused almost exclusively on urban and suburban centers. Given the distinct challenges and strengths of rural communities, understanding how rural recovery community centers both align with and diverge from their urban counterparts is critical. Although this study did not directly compare the two types of geographies, this study features several points of convergence and divergence between 12 rural recovery community centers and previously studied urban and suburban models.
Rural recovery community centers operate in resource-constrained environments and, according to director surveys and interviews, primarily serve individuals in early recovery while assuming an expanded role in treatment linkage as well as reducing the harms of substance use. Many of the rural centers described in this study functioned as the primary naloxone provider in their communities, with one director noting distribution to schools, police departments, and other local organizations. At the same time, these centers face challenges tied to rural geography. Transportation and housing were consistently identified as major barriers, and while some centers collaborated with community partners to arrange rides or identify housing options, directors reported ongoing difficulty addressing these and other social determinants of health. Directors also noted limited collaboration with providers of medications for opioid use disorder, despite repeated efforts to establish these partnerships. Rural recovery community centers may be addressing significant gaps in the continuum of care beyond supporting individuals already in or pursing their recovery. More research is needed to identify how rural recovery community centers may leverage their strengths to address their unique challenges.
This study included rural recovery community centers from one southeastern state, Georgia. Thus, the findings may be a result of contextual factors (e.g., health insurance provision, social and cultural norms, state-specific funding allocations) that may differ in other states.
Directors reported their participants’ demographics. It is possible that directors do not recall or track their participant demographics accurately.
BOTTOM LINE
Recovery community centers serve as important resource hubs for individuals in recovery, particularly those with low levels of recovery capital and few resources and who also have severe, complex, and chronic clinical histories. Findings from this study suggest that rural recovery community centers may play an even broader role, extending support beyond those in recovery by providing critical services that reduce the harms of substance use and facilitating linkage to treatment. In rural settings, these centers may also represent one of the few accessible entry points for historically marginalized groups, such as sexual and gender minorities, and for individuals pursuing non–12-step recovery pathways to engage in mutual-help meetings and peer-to-peer support. Given the range of services they offer, rural recovery community centers may be a key component of a national comprehensive response to the needs of people who use substances and those pursuing recovery. Additional research is needed to better understand how to strengthen and sustain these centers, particularly in rural communities.
For individuals and families seeking recovery: If you or a loved one is interested in changing your substance use, pursuing treatment, or exploring different recovery pathways, it could be very helpful to connect with a local recovery community center. Experts at these centers may be able to help you meet your goals and connect you with important services in your community including mental health counseling, job skills training, transportation supports, and many more.
For treatment professionals and treatment systems: Connecting individuals to community-based supports and resources is essential for building recovery capital and supporting goal attainment. Treatment professionals and systems should not only be aware of recovery community centers in their area, but also actively facilitate referrals to and collaborations with these centers. At the same time, it is important to recognize individual differences in needs and recovery goals, as not all patients will benefit from the same types of programming or center offerings.
For scientists: Additional research is needed to better understand the diverse ways recovery community centers support their communities and navigate structural and contextual challenges. This study drew on surveys and interviews with directors from 12 rural recovery community centers in Georgia; future work could expand the sample to include both rural and urban centers, enabling more direct comparisons across geographic contexts. Further research would also benefit from incorporating the perspectives and self-identified characteristics of center participants. Finally, supporting centers in the collection of non-intrusive, ethically appropriate data would help advance understanding of the individual- and community-level impacts of recovery community centers.
For policy makers: Comprehensive, systematic, and longitudinal research is needed to better understand how recovery community centers influence both individual participants and the broader communities they serve. This study highlights the distinct barriers rural recovery community centers face, as well as the strategies they employ to address them. Continued investment in research and funding will be essential to sustain these centers and deepen understanding of their role within recovery-oriented systems of care.
Under the Federal Office of Rural Health Policy’s definition of rurality, 19% of the US population, or about 65 million people, live in rural areas (i.e., defined as non-metro counties, or areas within metro counties of a certain size that have low population density, or areas where the commuting flow is not to an urban core, etc.). Individuals in or seeking substance use disorder recovery in these communities face distinct challenges related to geography, service access, and social determinants of health, often requiring creative, community-based solutions. Understanding how recovery support systems respond to urban–rural differences remains critical. Recovery community centers are a growing component of recovery support services, yet little is known about how these organizations operate in rural contexts or how they address the unique needs of rural communities.
Recovery community centers are locally embedded, nonprofit organizations that support people working toward or maintaining recovery outside of formal treatment settings. Rather than providing clinical care, these “hubs” emphasize connection, peer leadership, and practical problem-solving. Many are organized and staffed by people with lived experience and serve as gathering places where individuals can access peer support, attend recovery meetings, participate in social activities, and get linkages to available community resources. Beyond emotional and social support, recovery community centers often help participants navigate everyday barriers to stability, including job searches, paperwork, and access to health coverage. Evidence from administrative data suggests that deeper involvement with these centers is linked to stronger recovery-related resources (i.e., recovery capital). Despite their growing presence, research has rarely examined how these organizations function across different geographic contexts, particularly in rural areas. The current study addresses this gap by examining rural recovery community centers in Georgia.
HOW WAS THIS STUDY CONDUCTED?
Working in partnership with the Georgia Council for Recovery, the study team identified 13 rural recovery community centers actively operating in Georgia. Directors from each center were invited to complete a brief survey about their backgrounds and organizational characteristics, as well as participate in a virtual interview exploring how their centers support individuals with substance use disorders broadly and those receiving medications for opioid use disorder specifically.
There were 12 directors that participated, although 1 left more than 50% of their survey blank, which resulted in their survey being excluded from descriptive analyses. Most directors identified as White and had lived experience of recovery, though a minority represented other racial backgrounds or did not have personal recovery experience. The sample included 8 women and 4 men, with an average age of 42 and approximately 6 years of professional experience in the addiction field. Half of the directors were raised in rural communities, one quarter held at least a bachelor’s degree, and three quarters identified as Christian.
WHAT DID THIS STUDY FIND?
“Modest but Mighty”: Rural recovery community centers were modest but mighty resource hubs
These centers had a modest annual average budget of $225,407. They served, on average, 468 people each month, with 41 of them being new. They had an average of 5 paid staff, but that ranged from 1-9. There were also about 7 volunteer staff on average. The directors also reported the in-house services their center provides (see graph below) and the services they link to (see graphic below).
Rural recovery community center participants had a range of backgrounds and identities
According to directors’ estimates, individuals served by rural recovery community centers entered services through multiple pathways, most commonly from formal treatment programs (34%), followed by self-referral (28%), and referrals from the legal system (25%). Most participants were adults between the ages of 25 and 59 (68%), with very few under the age of 18 (3%). Participants were more often male (56%), and a substantial proportion were currently involved in the legal system (61%). Educational attainment was generally low, with 39% of participants lacking a high school diploma, though nearly half were employed full time (44%). Racially, most participants were White (60%), while more than one quarter were Black (27%). In terms of recovery status, over half of participants were within their first year of recovery (58%), and a smaller subset were actively using substances (7%). Amphetamines were the most cited primary substance of choice (28%), followed by alcohol (24%), opioids (21%), cannabis (10%), cocaine (7%), and benzodiazepines (5%).
Transportation and housing were common challenges
Most rural recovery community center directors reported transportation as their single greatest challenge. One director shared:
“We have recovery options and can help people get to them, but with rural areas, everything is so spread out. There may be resources in our region, but the region is so large that people can’t necessarily access them…Without us providing transportation, people wouldn’t be able to get there.”
The directors reported a range of strategies that they use to address challenges. For transportation, some recovery community centers owned their own vehicles, and others dedicated volunteer and staff hours, along with their personal vehicles, to transportation. Some centers developed partnerships to help facilitate transportation and rideshare options.
Housing was the second most reported challenge. Affordable housing, recovery housing, and shelters for people experiencing homeless were all noted to be lacking. Directors also mentioned unique housing barriers related to people with substance use histories such as upfront costs (e.g., rent deposits), poor credit scores, and criminal backgrounds. To address some of the housing challenges, directors developed partnerships with local property owners to identify available housing, and some directors used center funds to cover the upfront financial costs of some housing options.
Directors also brought up other challenges their centers and participants faced such as limited resources, lack of gainful employment, health insurance access (Georgia did not expand Medicaid to cover those with low income), lack of affordable childcare, unmet basic needs, and community stigma.
Here directors highlighted partnerships with recovery-friendly employers as well as employment support, which included resume building services, physical space to apply for jobs and conduct virtual interviews, and a clothing closet for job interviews. Connections to GED programs and in-house access to computers were also mentioned in response to the education barriers. Some centers made food and hygiene products available in house, and a few even provided funds to participants for groceries and utility bills.
Community collaborations were key for rural recovery community centers
All of the center directors focused on community collaborations and engagement to enhance their services and address the barriers their participants face. One directed even noted, “My theme has been putting the ‘C’ back in [Recovery Community Organization].”
The intentional and coordinated community collaborations featured a variety of other organizations. All of the directors collaborated with local substance use disorder treatment services, including detox facilities, and office-based buprenorphine treatment providers. They all also noted their connections with social services (e.g., child welfare, shelters, local nonprofits). Several directors even mentioned that they sit on the board of directors for other nonprofit organizations. Most of the directors discussed how they worked with the criminal legal system.
That said, connections to opioid use disorder medication providers was minimal. Rural recovery community centers provide critical linkages and services
Rural recovery community centers were instrumental helping people access treatment.
Through their community partners, local embeddedness, and unique skills, recovery community center staff were able to help participants enroll in Medicaid and identify opening at state-funded treatment services:
In addition to connections to treatment and recovery services, rural community centers were often the primary or only naloxone distributor. Naloxone is an opioid antagonist that works by blocking opioid receptors in the brain, which can reverse an opioid overdose, and is often known by its brand name, Narcan. One director underscored how availability of naloxone would drop without them by sharing, “Many organizations, schools, police departments, and others rely on us to provide [naloxone].”
Rural recovery community centers also helped increase the variety and access of mutual-help organizations. This included recovery pathways not as common in rural areas such as Celebrate Recovery, All Recovery, SMART Recovery, and Yoga Recovery. In addition to 12-step meetings (e.g., Alcoholics Anonymous), they featured meetings for identity groups such as sexual and gender minorities, veterans, family members of people with substance use disorder, people receiving medications for opioid use disorder, and those with co-occurring mental health conditions.
Rural recovery community center directors highlighted that mutual-help organization meetings and one-on-one peer support as the most important services provided in-house. One-on-one peer support (i.e., recovery coaching) featured structured sessions and regular check-ins. One director described it as:
“The peer walks us through their life and identifies what they need to improve. We then set goals to help them get there…we lift the peer’s voice and focus on what’s going right in their life. We create a safe space where they can celebrate their strengths and build on them.”
Another shared:
“We take a strengths-based approach, talking about what’s going well in their life. It’s all about starting with a positive focus, and that’s how we engage with everyone who comes through.”
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Recovery community centers serve as hubs for recovery support and as important connectors to health and social services within their communities, with prior research demonstrating their potential to enhance recovery capital among participants. However, much of the existing literature has focused almost exclusively on urban and suburban centers. Given the distinct challenges and strengths of rural communities, understanding how rural recovery community centers both align with and diverge from their urban counterparts is critical. Although this study did not directly compare the two types of geographies, this study features several points of convergence and divergence between 12 rural recovery community centers and previously studied urban and suburban models.
Rural recovery community centers operate in resource-constrained environments and, according to director surveys and interviews, primarily serve individuals in early recovery while assuming an expanded role in treatment linkage as well as reducing the harms of substance use. Many of the rural centers described in this study functioned as the primary naloxone provider in their communities, with one director noting distribution to schools, police departments, and other local organizations. At the same time, these centers face challenges tied to rural geography. Transportation and housing were consistently identified as major barriers, and while some centers collaborated with community partners to arrange rides or identify housing options, directors reported ongoing difficulty addressing these and other social determinants of health. Directors also noted limited collaboration with providers of medications for opioid use disorder, despite repeated efforts to establish these partnerships. Rural recovery community centers may be addressing significant gaps in the continuum of care beyond supporting individuals already in or pursing their recovery. More research is needed to identify how rural recovery community centers may leverage their strengths to address their unique challenges.
This study included rural recovery community centers from one southeastern state, Georgia. Thus, the findings may be a result of contextual factors (e.g., health insurance provision, social and cultural norms, state-specific funding allocations) that may differ in other states.
Directors reported their participants’ demographics. It is possible that directors do not recall or track their participant demographics accurately.
BOTTOM LINE
Recovery community centers serve as important resource hubs for individuals in recovery, particularly those with low levels of recovery capital and few resources and who also have severe, complex, and chronic clinical histories. Findings from this study suggest that rural recovery community centers may play an even broader role, extending support beyond those in recovery by providing critical services that reduce the harms of substance use and facilitating linkage to treatment. In rural settings, these centers may also represent one of the few accessible entry points for historically marginalized groups, such as sexual and gender minorities, and for individuals pursuing non–12-step recovery pathways to engage in mutual-help meetings and peer-to-peer support. Given the range of services they offer, rural recovery community centers may be a key component of a national comprehensive response to the needs of people who use substances and those pursuing recovery. Additional research is needed to better understand how to strengthen and sustain these centers, particularly in rural communities.
For individuals and families seeking recovery: If you or a loved one is interested in changing your substance use, pursuing treatment, or exploring different recovery pathways, it could be very helpful to connect with a local recovery community center. Experts at these centers may be able to help you meet your goals and connect you with important services in your community including mental health counseling, job skills training, transportation supports, and many more.
For treatment professionals and treatment systems: Connecting individuals to community-based supports and resources is essential for building recovery capital and supporting goal attainment. Treatment professionals and systems should not only be aware of recovery community centers in their area, but also actively facilitate referrals to and collaborations with these centers. At the same time, it is important to recognize individual differences in needs and recovery goals, as not all patients will benefit from the same types of programming or center offerings.
For scientists: Additional research is needed to better understand the diverse ways recovery community centers support their communities and navigate structural and contextual challenges. This study drew on surveys and interviews with directors from 12 rural recovery community centers in Georgia; future work could expand the sample to include both rural and urban centers, enabling more direct comparisons across geographic contexts. Further research would also benefit from incorporating the perspectives and self-identified characteristics of center participants. Finally, supporting centers in the collection of non-intrusive, ethically appropriate data would help advance understanding of the individual- and community-level impacts of recovery community centers.
For policy makers: Comprehensive, systematic, and longitudinal research is needed to better understand how recovery community centers influence both individual participants and the broader communities they serve. This study highlights the distinct barriers rural recovery community centers face, as well as the strategies they employ to address them. Continued investment in research and funding will be essential to sustain these centers and deepen understanding of their role within recovery-oriented systems of care.