WHAT PROBLEM DOES THIS STUDY ADDRESS?
Kratom is an herbal substance that is extracted from a plant native to Asian countries. At lower doses, it produces stimulant-like effects; at higher doses, it produces opioid-like effects. This substance has recently grown in popularity for its sedating, pain-relieving, and pleasurable effects, in addition to its potential in treating substance use disorder, particularly opioid use disorder. However, in the United States, kratom products have become widely and easily available in a variety of forms, such as powders, gummies, and energy shots. Higher potency products found in kratom, such as 7-hydroxymitragynine (7-OH), are also being developed synthetically and have become widely available, Consumption of these more potent kratom-related products can increase the risk of experiencing adverse reactions – including cardiovascular, gastrointestinal, neurological, and psychiatric harms – that can lead to hospitalizations or even death. Reports to poison centers involving kratom exposures offer a way to monitor trends in population-wide public health consequences of kratom use. This study examined trends in kratom-related poison reports over the last 11 years, which corresponds to the time frame it evolved into higher potency products.
HOW WAS THIS STUDY CONDUCTED?
The researchers in this study analyzed trends in kratom-related reports to the National Poison Data System, the data repository for 53 US poison centers, from January 1, 2015 and December 31, 2025. Trends by exposure report type (single vs. multiple substances), demographics, and medical outcomes were analyzed. The Data System defines an exposure report as “actual or suspected contact with a substance that prompted a consultation with a poison center.” Variables of interest included demographic information (age and sex), the substance the person was exposed to, reported reason for use, level of care received, and medical outcome. Medical outcomes were defined as serious if they resulted in death; life threatening effects, disability, or disfigurement (major effects); or the need for treatment (moderate effects). Hospitalization included admissions to critical care, noncritical care, and psychiatric units. Data for people who were at least 12 years old or older were included and were grouped as follows: 12-19, 20-39, 40-59, and 60 years old or older. The analyses examined changes in exposure report rates (per 1 million reports) for each year in the study period and were stratified by exposure report type, sex, and age.
Of note, this study included both actual and suspected contact with kratom and other substances and relied on self-reports. Thus, whether the person was actually exposed cannot be verified, some substances may have been misclassified, the formulation of kratom is unknown (i.e., traditional whole leaf products or higher potency products like 7-OH), and when multiple substances were involved, it is difficult to determine which substance was most responsible for adverse reaction. Also, kratom-related exposures that resulted in milder reactions that did not require contact with a poison center were not captured in this study, which may underestimate the totality of kratom’s adverse effects.
WHAT DID THIS STUDY FIND?
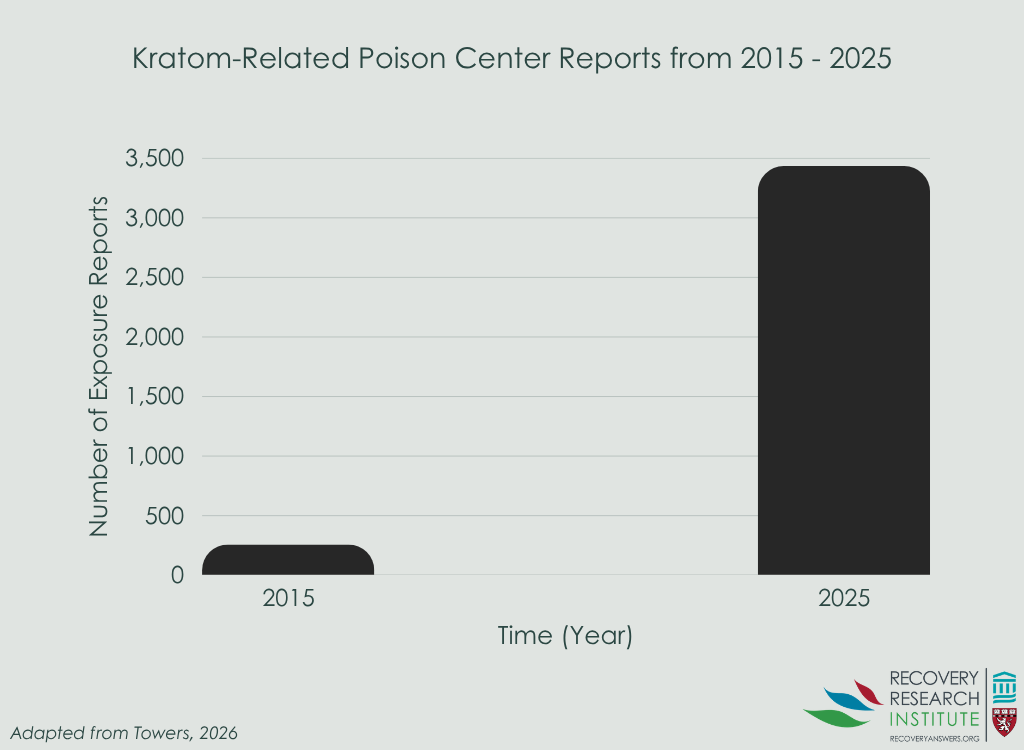
Between 2015 and 2025, there were a total of 14,449 kratom-related reports made to a poison center. In 2015, there were 258 kratom-related reports, while in 2025 there was a sharp increase with 3,434 reports, which represents an increase of approximately 1,200% (see graph below). Of these, the majority involved exposure to a single substance (62%) and the remaining 38% involved multiple substances. Despite this higher number of single-substance reports, reports involving multiple substances occurred at higher rates, with a range of 467 – 5,442 per 1 million reports versus a range of 388-4,045 per 1 million single-substance reports.
Trends by sex showed that the majority of reports were from men, who accounted for 65%-71% of single-substance reports and 67%-76% of multiple-substance reports. Although reports from men were higher overall, there were sharp increases for both men and women between 2015 and 2025. Single- and multiple-substance reports from men were 10 and 11 times higher in 2025 than those in 2015, respectively. For women, single- and multiple-substance reports were 9 and 10 times higher in 2025 than in 2015, respectively.
Trends by age showed that the majority of reports were among young adults between the ages of 20 and 39 for both single- and multiple-substance reports. However, the sharpest increase was observed among adults between the ages of 40 and 59.
Trends by level of care showed that hospitalizations for single- and multiple-substance exposure reports similarly increased by 1,200% and 1,300%, respectively, between 2015 and 2025. In 2015, there were 43 single-substance reports and 40 multiple-substance reports that resulted in hospitalization, while in 2025, there were 538 single-substance reports and 549 multiple-substance reports that resulted in hospitalization. Across the study period, hospitalizations were consistently higher for people with multiple-substance reports (44%-56%) than single-substance reports (24%-29%).
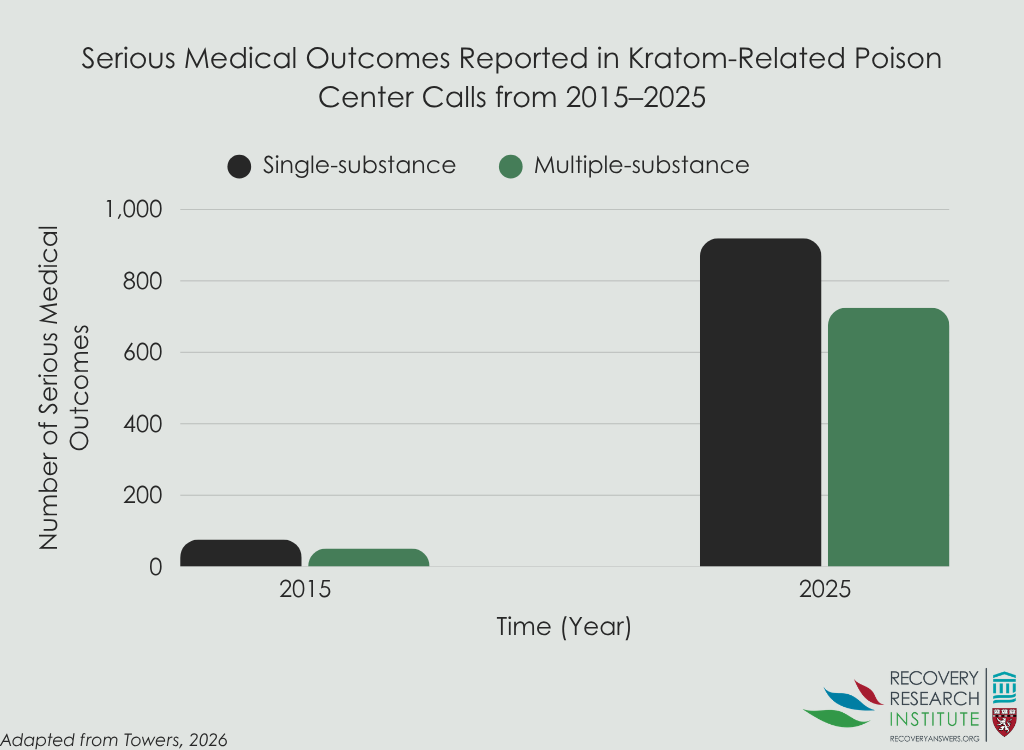
Trends by medical outcomes showed that serious outcomes also increased sharply (see graph below). Serious outcomes for single- and multiple-substance reports increased by 1,100% and 1,300%, respectively, between 2015 and 2025. In 2015, there were 76 single-substance reports and 51 multiple-substance reports that resulted in a serious outcome, while in 2025, there were 919 single-substance reports and 725 multiple-substance reports that resulted in a serious outcome. Across the study period, serious outcomes were consistently higher for people with multiple-substance reports (57%-66%) than single-substance reports (41%-49%).
There were also a total 233 kratom-related deaths reported during the study period, of which the majority were accounted for by multiple-substance reports (79%). Among these deaths involving multiple substances, 62% involved opioids (e.g., hydrocodone, codeine, methadone), 20% involved benzodiazepines (i.e., depressants such as Valium and Xanax), 20% involved stimulants (e.g., cocaine, Adderall), and 19% involved alcohol.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study demonstrated a sharp increase in kratom-related reports to poison centers, hospitalizations, serious outcomes, and deaths from 2015 to 2025. Further, reports involving multiple substances were associated more frequently with hospitalizations, serious outcomes, and deaths. Although there were several limitations from the study relying on self-reports made to poison centers that involved confirmation of an exposure, the specific type of substance, and formulation, these findings highlight concerning trends in adverse reactions from kratom use. The dramatic rise in adverse reactions and deaths, coupled with the frequency of reports involving multiple substances, point to the need for regulations on kratom and related products and efforts to prevent high risk use (i.e., in combination with other substances, use of high potency products). Treatment programs may have difficulty testing for kratom as its assessment is not part of standard urine drug screen panels, though some laboratories may offer specific testing. Future research is also needed to continue to monitor trends in emerging public health threats involving kratom, to examine long-term health consequences of kratom use, and to investigate what regulatory and preventive efforts are most helpful.
BOTTOM LINE
Between 2015 and 2025, sharp increases were observed in kratom-related reports to poison centers, hospitalizations, serious outcomes, and deaths, especially when multiple substances were involved. These findings point to the need for regulations on kratom and related products and efforts to prevent high risk use.
- For individuals and families seeking recovery: Increasing reports of adverse reactions involving kratom, particularly when used with other substances, highlight the importance of understanding potential risks associated with high potency products and polysubstance use. Individuals and families may benefit from discussing kratom use openly with healthcare providers and seeking support early if concerning symptoms or substance use patterns emerge.
- For treatment professionals and treatment systems: These findings reinforce the importance of screening for the use of kratom and other emerging substances, which may have to be conducted through specific laboratories. Providing education about potential risks associated with combining kratom with other substances and monitoring for adverse reactions may help prevent serious outcomes and save lives.
- For scientists: Because the study relied on self-reports to poison centers and could not confirm exposures, substance type, or product formulation, future research using more objective measures would help clarify the extent and causes of kratom-related harms. Additional research examining long-term health consequences would shed light on how kratom use affects health over time. Finally, research investigating different regulatory and preventive approaches would help identify the most useful public health strategies.
- For policy makers: These findings point to the importance of monitoring emerging public health threats involving kratom, given the recent sharp increases in poison reports, hospitalizations, and deaths. Policies focused on product regulation, labeling, surveillance, and prevention of high-risk use, such as in combination with other substances and use of high potency products, may help reduce serious adverse outcomes and save lives.
CITATIONS
Towers, E. B., Thomas, Y. T., Holstege, C. P., & Farah, R. (2026). Increases in kratom-related reports to poison centers—National Poison Data System, United States, 2015–2025. Morbidity and Mortality Weekly Report (MMWR), 75(11), 139-145.













