High risk, low access: Illicit drug use and treatment needs among California’s homeless population
The most recent representative study on Illicit substance use among those experiencing homelessness in the United States was conducted over 25 years ago. Since then, substance use trends have changed and the number of people experiencing homelessness has increased dramatically. To help address this knowledge gap this study examined patterns of substance use and treatment needs among adults experiencing homelessness in California.
Illicit substance use is a significant challenge for those experiencing homelessness in the US while drug overdose is one of the leading causes of death among people experiencing homelessness. Concurrently, substance use can interfere with a person’s economic and social functioning making it challenging to find stable housing. In addition, some programs for the homeless (e.g., shelters) have strict abstinence policies which create a barrier for those with current substance use disorders to find shelter. There is also evidence that for some substance use initiation occurs after becoming homeless, suggesting that homelessness is a risk factor for problematic substance use and substance use disorders. Given these overlapping challenges, it is critically important to understand the scope of illicit substance use among people experiencing homelessness. Unfortunately, there has been a lack of research on this topic, with the most recent representative study being published in 1999. To address this knowledge gap, the current study utilized representative survey data to estimate patterns of illicit drug use and substance use treatment access among people experiencing homelessness in California.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the California Statewide Study of People Experiencing Homelessness project. This project, conducted by The University of California, San Francisco Benioff Homelessness and Housing Initiative, is the largest representative study of homelessness in the US in over 25 years. The goal of this project was to collect representative data on the scope of social and health issues for those experiencing homelessness to inform policies and programs to end adult homelessness in California. This project used a mixed methods design – both quantitative (surveys) and qualitative (in-depth interviews) data were collected, but only the survey data were analyzed for the present study. Data were collected between October 2021 and November 2022. Project staff conducted interviews in English or Spanish, or via interpreters (i.e., for other languages).
The California Statewide Study of People Experiencing Homelessness project authors utilized multiple approaches to recruit a diverse and representative sample. First, the authors divided the state into 8 distinct regions then selected 1 county per region in which to focus recruitment efforts. Counties were selected based on demographic makeup (i.e., were most representative of the overall population of California). The authors then compiled a list of venues within each county in which homeless populations were known to congregate (e.g., homeless shelters, non-shelter service providers, encampments, etc.). The project authors then sent interviewers to each venue to collect participant data. Interviewers were provided with a target number of interviews to complete per venue based on estimated venue size (e.g., 5 interviews for venues with 5-25 people experiencing homelessness). In addition, the project authors used respondent-driven sampling, a peer-referral based sampling strategy to recruit difficult to reach populations (e.g., LGBTQ individuals) and those that may have been missed in the venue-based sampling.
The main outcomes of the present study were lifetime and past 6-month illicit substance use and drug type (i.e., methamphetamine, nonprescription opioids [heroin, fentanyl,
or other opioid], and cocaine [cocaine/crack cocaine]). These outcomes were measured via a modified version of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test. The authors categorized Illicit drug use as regular (i.e., ≥3 times per week), occasional (i.e., >2 times per month and < 3 times per week, once or twice a month, or less than monthly), or no use (i.e., no self-reported illicit drug use). Participants who reported regular lifetime use of any substance were also asked when they had initiated use (i.e., before or after experiencing homelessness). In addition, the authors assessed unmet substance use treatment needs by asking participants if they wanted treatment but were unable to obtain it.
This study had a sample of 3,200 people experiencing homelessness (3,042 from venue-based recruitment and 158 from respondent-driven sampling). The sample mostly consisted of cisgender men (67.3%) followed by cisgender women (31.2%) and gender minorities (e.g., transgender) people (1.6%). The average age of participants was 46 years old. The study sample was racially and ethnically diverse – most participants identified as either White (27.9%), Hispanic/Latine (26.4%), or Black/African American (26.3%), with the remaining participants identifying as Multiracial and Multiethnic (14.3%), American Indian/Alaskan Native (2.9%), Asian/Pacific Islander (1.7%), or another race not listed (0.5%). Most participants reported being homeless for less than 3 years (64.3%) and were unsheltered (i.e., they slept in places not meant for human habitation, excluding vehicles, such as on the streets).
WHAT DID THIS STUDY FIND?
Illicit substance use was common among participants
Over 75% of participants reported using illicit drugs at least once during their lifetime, with 65% reporting lifetime regular use. Approximately 50% and 37% reported any and regular drug use in the last 6 months, respectively. Nearly a quarter reported using illicit substances regularly after becoming homeless.
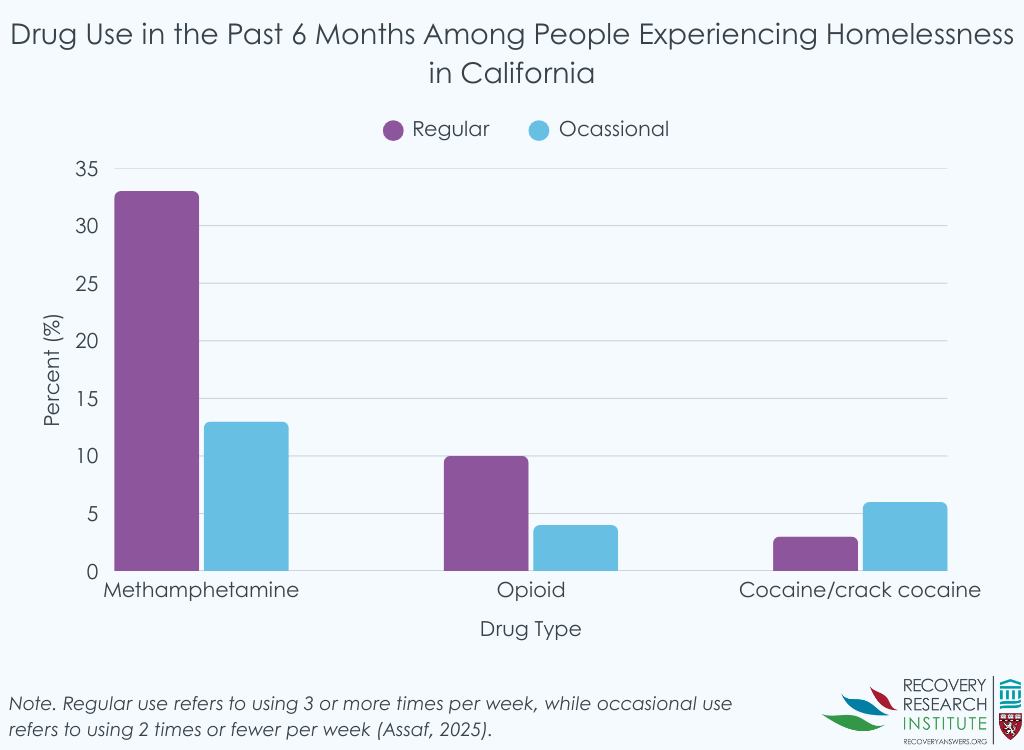
Methamphetamine was the most used illicit substance
Approximately 65% of participants reported any lifetime methamphetamine use and 55% reported regular lifetime use. As shown in the graph below, recent (past 6 month) methamphetamine use was reported by 46% of participants, with 33% reporting regular use.
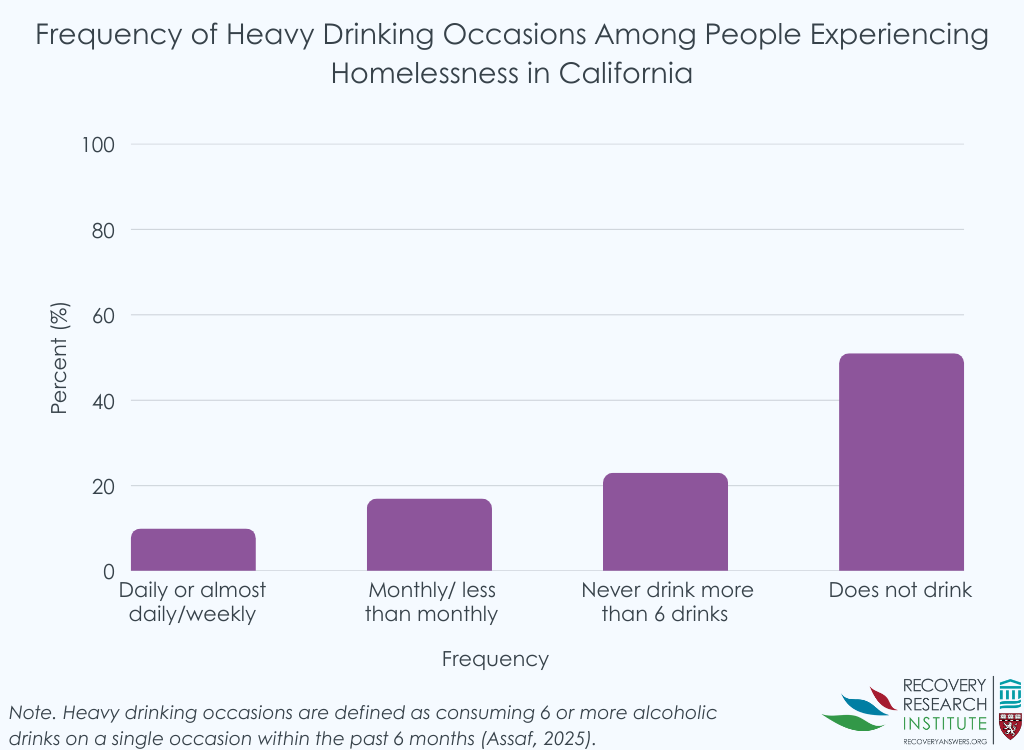
As shown in the graph below, 1/4 reported heavy drinking – 6 or more drinks on a single occasion. Half did not use any alcohol in the past 6 months.
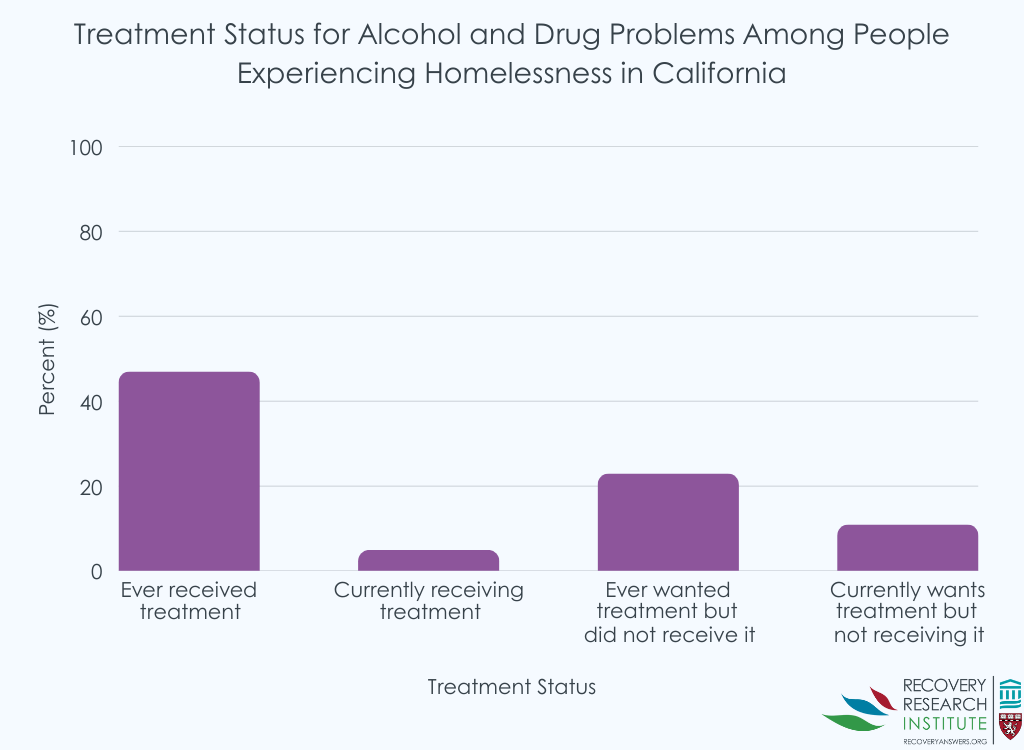
Participants reported unmet substance use treatment needs
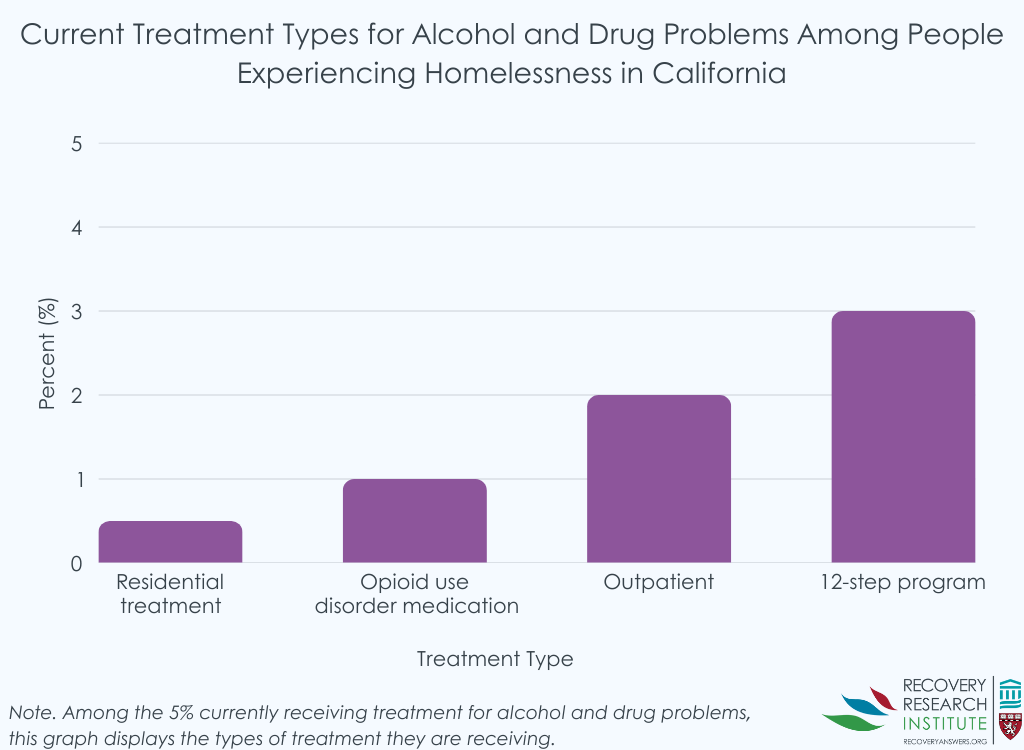
The graphs below depict participants’ treatment histories. While only 5% were currently in treatment or attending a 12-step mutual-help group, half had been to substance use treatment in their lifetime. Moreover, 23% reported being unable to receive substance use treatment despite wanting it at some point in their lives while 11% currently wanted treatment but were unable to receive it. For those currently wanting treatment but unable to receive it, this figure was even higher – 21% – for those with regular illicit drug use in the last 6 months.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study show that illicit drug use (particularly methamphetamine) is commonplace among people experiencing homelessness in California. The data also shows that those experiencing homelessness have unmet substance use treatment needs and that many participants began regular drug use after becoming homeless. While important, the present study can only tell us about the prevalence of illicit drug use – not drug use disorder – while giving some clues about potential unmet treatment needs among those experiencing homelessness. That is, these data cannot explain why this population may engage in illicit substance use nor offer clues on how to address illicit substance use. It is likely that a substantial proportion of this population suffer from severe mental illnesses including psychosis or bipolar disorders. It is possible that some use illicit substances to cope with trauma and therefore addressing the mental health needs of those experiencing homelessness may be one strategy to address emerging problematic substance use and substance use disorders. However, this is speculative and beyond the scope of the current study. Given the ongoing homelessness crisis, there is a desperate need to understand what contributes to the high rates of illicit substance use among those experiencing homelessness. Such knowledge can lead to the development of interventions to address the needs of those experiencing homelessness.
Irrespective of the underlying reasons, results of this study underscore how illicit drug use may both precede and perpetuate the cycle of homelessness. Although many participants (41.6%) reported initiating regular illicit drug use before first experiencing homelessness, a sizeable number (23.2%) began using regularly only after becoming homeless. This suggests that, for some, regular use may have been an effect of the psychosocial consequences of becoming homeless rather than a cause. The initiation of regular substance use after becoming homeless could be a means of seeking some kind of pleasure, psychological escape, or relief including coping with trauma (e.g., of losing shelter). That 1/5 of participants with regular drug use in the past 6 months wanted, but could not obtain, treatment is noteworthy – this is substantially higher than the general population, where only 4% of those with substance use disorder thought they needed treatment but could not obtain it (e.g., due to health insurance limitations). This observed unmet substance use treatment need among participants demonstrates the difficulty those experiencing homelessness face in overcoming problematic substance use. That is, without treatment those suffering from addiction will experience more obstacles to finding stable housing.
The present study was restricted to California and therefore has limited generalizability to the rest of the US. Evidence shows that the homeless population in California may differ from those experiencing homelessness elsewhere. For example, older adults (i.e., those 50+ years of age) comprise 40% of the homeless population in California, compared to 20% nationally. Furthermore, evidence shows that those experiencing homelessness in California are more likely to be unsheltered compared to those experiencing homelessness in other states. The reasons for these differences are unknown but are likely due to a combination of economic and environmental factors unique to California.
Utilizing a venue-based sampling strategy may have impacted the results. This strategy may have failed to recruit participants experiencing homelessness who would not be present at identified venues (e.g., shelters), such as those staying with friends/family or living in their vehicles (a common phenomenon in California). Such individuals may engage in illicit substance use at different rates compared to the predominantly unsheltered participants recruited for the study.
The use of interviewer administered questionnaires may have impacted the study findings. For example, participants may have underreported their substance use due to desirability bias or interviewer characteristics (e.g., gender).
This representative study shows that illicit substance use (especially methamphetamine) is highly prevalent among individuals experiencing homelessness in California. The results of the study also show that a substantial number of participants began using illicit substances regularly only after experiencing homelessness and had unmet substance use treatment needs. Taken together, these results suggest that illicit substance use may be both a cause and effect of homelessness. However, it is beyond the scope of these data to show why this may be the case, nor can the data provide clues on how to address this ongoing crisis. Future research to understand the underlying reasons for illicit substance use among those experiencing homelessness is critical for developing public health interventions.
For individuals and families seeking recovery: The present study suggests that at least some of those experiencing homelessness have unmet substance use treatment needs. Therefore, it may be important for those seeking recovery for themselves or their loved ones to look for low-barrier treatment programs that allow for person-centered goals. These may include low- or no-cost services (e.g., Salvation Army) or those that may not require abstinence for entry (e.g., Housing First style programs or syringe exchange programs). Such programs may be more accessible for those seeking treatment but are unable or not desiring to abstain from use. In addition, it may be beneficial to seek out care that is paired with stable housing, mental health support, and social services. Seek out providers that offer wraparound services or can refer you to programs that connect health care with housing and employment support.
For treatment professionals and treatment systems: The present study suggests that treatment professionals and those working in treatment systems that service those experiencing homelessness may do well to prioritize offering low-barrier substance use treatment, such as services on a sliding scale to facilitate their use by those with limited resources. In addition, implementing approaches to care that meet people “where they’re at” in the stages of therapeutic change may be effective in reducing unmet treatment needs among those experiencing homelessness, for example by offering medication-assisted treatment and overdose prevention tools (e.g., naloxone) for those using opioids. Outreach and mobile treatment services can help engage individuals who do not access traditional clinical settings.
For scientists: The present study underscores the need for scientists to investigate potential drivers of illicit substance use among those experiencing homelessness. Such drivers may include using illicit substances to cope with trauma and/or relapses precipitated by the stress of becoming homeless. Qualitative methodologies could offer valuable insight into the motivations for illicit substance use among this population. In addition, there is a need for scientists to investigate the barriers preventing those experiencing homelessness from seeking substance use treatment. It is likely that a combination of lack of health insurance, treatment affordability, and available providers contribute to unmet treatment needs. Empirical evidence is needed to better understand the specific reason why homeless individuals may be unable to access needed care, but from a hierarchy of needs perspective, it may be that housing that includes mental health and substance use treatment could be the ideal combination.
For policy makers: The present study suggests that policymakers may do well to consider strategies to expand services – especially addressing substance use – for those experiencing homelessness. Such efforts could include expanding outreach and mobile treatment services to engage individuals who cannot access traditional clinical settings. Additionally, there is a need for policy makers to expand wraparound services which can help provide affordable housing, metal health services and job assistance to those experiencing homelessness. Such programs may be critical for stopping the cycle of homelessness and addiction as they address the myriad challenges experienced by those experiencing homelessness simultaneously.
Illicit substance use is a significant challenge for those experiencing homelessness in the US while drug overdose is one of the leading causes of death among people experiencing homelessness. Concurrently, substance use can interfere with a person’s economic and social functioning making it challenging to find stable housing. In addition, some programs for the homeless (e.g., shelters) have strict abstinence policies which create a barrier for those with current substance use disorders to find shelter. There is also evidence that for some substance use initiation occurs after becoming homeless, suggesting that homelessness is a risk factor for problematic substance use and substance use disorders. Given these overlapping challenges, it is critically important to understand the scope of illicit substance use among people experiencing homelessness. Unfortunately, there has been a lack of research on this topic, with the most recent representative study being published in 1999. To address this knowledge gap, the current study utilized representative survey data to estimate patterns of illicit drug use and substance use treatment access among people experiencing homelessness in California.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the California Statewide Study of People Experiencing Homelessness project. This project, conducted by The University of California, San Francisco Benioff Homelessness and Housing Initiative, is the largest representative study of homelessness in the US in over 25 years. The goal of this project was to collect representative data on the scope of social and health issues for those experiencing homelessness to inform policies and programs to end adult homelessness in California. This project used a mixed methods design – both quantitative (surveys) and qualitative (in-depth interviews) data were collected, but only the survey data were analyzed for the present study. Data were collected between October 2021 and November 2022. Project staff conducted interviews in English or Spanish, or via interpreters (i.e., for other languages).
The California Statewide Study of People Experiencing Homelessness project authors utilized multiple approaches to recruit a diverse and representative sample. First, the authors divided the state into 8 distinct regions then selected 1 county per region in which to focus recruitment efforts. Counties were selected based on demographic makeup (i.e., were most representative of the overall population of California). The authors then compiled a list of venues within each county in which homeless populations were known to congregate (e.g., homeless shelters, non-shelter service providers, encampments, etc.). The project authors then sent interviewers to each venue to collect participant data. Interviewers were provided with a target number of interviews to complete per venue based on estimated venue size (e.g., 5 interviews for venues with 5-25 people experiencing homelessness). In addition, the project authors used respondent-driven sampling, a peer-referral based sampling strategy to recruit difficult to reach populations (e.g., LGBTQ individuals) and those that may have been missed in the venue-based sampling.
The main outcomes of the present study were lifetime and past 6-month illicit substance use and drug type (i.e., methamphetamine, nonprescription opioids [heroin, fentanyl,
or other opioid], and cocaine [cocaine/crack cocaine]). These outcomes were measured via a modified version of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test. The authors categorized Illicit drug use as regular (i.e., ≥3 times per week), occasional (i.e., >2 times per month and < 3 times per week, once or twice a month, or less than monthly), or no use (i.e., no self-reported illicit drug use). Participants who reported regular lifetime use of any substance were also asked when they had initiated use (i.e., before or after experiencing homelessness). In addition, the authors assessed unmet substance use treatment needs by asking participants if they wanted treatment but were unable to obtain it.
This study had a sample of 3,200 people experiencing homelessness (3,042 from venue-based recruitment and 158 from respondent-driven sampling). The sample mostly consisted of cisgender men (67.3%) followed by cisgender women (31.2%) and gender minorities (e.g., transgender) people (1.6%). The average age of participants was 46 years old. The study sample was racially and ethnically diverse – most participants identified as either White (27.9%), Hispanic/Latine (26.4%), or Black/African American (26.3%), with the remaining participants identifying as Multiracial and Multiethnic (14.3%), American Indian/Alaskan Native (2.9%), Asian/Pacific Islander (1.7%), or another race not listed (0.5%). Most participants reported being homeless for less than 3 years (64.3%) and were unsheltered (i.e., they slept in places not meant for human habitation, excluding vehicles, such as on the streets).
WHAT DID THIS STUDY FIND?
Illicit substance use was common among participants
Over 75% of participants reported using illicit drugs at least once during their lifetime, with 65% reporting lifetime regular use. Approximately 50% and 37% reported any and regular drug use in the last 6 months, respectively. Nearly a quarter reported using illicit substances regularly after becoming homeless.
Methamphetamine was the most used illicit substance
Approximately 65% of participants reported any lifetime methamphetamine use and 55% reported regular lifetime use. As shown in the graph below, recent (past 6 month) methamphetamine use was reported by 46% of participants, with 33% reporting regular use.
As shown in the graph below, 1/4 reported heavy drinking – 6 or more drinks on a single occasion. Half did not use any alcohol in the past 6 months.
Participants reported unmet substance use treatment needs
The graphs below depict participants’ treatment histories. While only 5% were currently in treatment or attending a 12-step mutual-help group, half had been to substance use treatment in their lifetime. Moreover, 23% reported being unable to receive substance use treatment despite wanting it at some point in their lives while 11% currently wanted treatment but were unable to receive it. For those currently wanting treatment but unable to receive it, this figure was even higher – 21% – for those with regular illicit drug use in the last 6 months.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study show that illicit drug use (particularly methamphetamine) is commonplace among people experiencing homelessness in California. The data also shows that those experiencing homelessness have unmet substance use treatment needs and that many participants began regular drug use after becoming homeless. While important, the present study can only tell us about the prevalence of illicit drug use – not drug use disorder – while giving some clues about potential unmet treatment needs among those experiencing homelessness. That is, these data cannot explain why this population may engage in illicit substance use nor offer clues on how to address illicit substance use. It is likely that a substantial proportion of this population suffer from severe mental illnesses including psychosis or bipolar disorders. It is possible that some use illicit substances to cope with trauma and therefore addressing the mental health needs of those experiencing homelessness may be one strategy to address emerging problematic substance use and substance use disorders. However, this is speculative and beyond the scope of the current study. Given the ongoing homelessness crisis, there is a desperate need to understand what contributes to the high rates of illicit substance use among those experiencing homelessness. Such knowledge can lead to the development of interventions to address the needs of those experiencing homelessness.
Irrespective of the underlying reasons, results of this study underscore how illicit drug use may both precede and perpetuate the cycle of homelessness. Although many participants (41.6%) reported initiating regular illicit drug use before first experiencing homelessness, a sizeable number (23.2%) began using regularly only after becoming homeless. This suggests that, for some, regular use may have been an effect of the psychosocial consequences of becoming homeless rather than a cause. The initiation of regular substance use after becoming homeless could be a means of seeking some kind of pleasure, psychological escape, or relief including coping with trauma (e.g., of losing shelter). That 1/5 of participants with regular drug use in the past 6 months wanted, but could not obtain, treatment is noteworthy – this is substantially higher than the general population, where only 4% of those with substance use disorder thought they needed treatment but could not obtain it (e.g., due to health insurance limitations). This observed unmet substance use treatment need among participants demonstrates the difficulty those experiencing homelessness face in overcoming problematic substance use. That is, without treatment those suffering from addiction will experience more obstacles to finding stable housing.
The present study was restricted to California and therefore has limited generalizability to the rest of the US. Evidence shows that the homeless population in California may differ from those experiencing homelessness elsewhere. For example, older adults (i.e., those 50+ years of age) comprise 40% of the homeless population in California, compared to 20% nationally. Furthermore, evidence shows that those experiencing homelessness in California are more likely to be unsheltered compared to those experiencing homelessness in other states. The reasons for these differences are unknown but are likely due to a combination of economic and environmental factors unique to California.
Utilizing a venue-based sampling strategy may have impacted the results. This strategy may have failed to recruit participants experiencing homelessness who would not be present at identified venues (e.g., shelters), such as those staying with friends/family or living in their vehicles (a common phenomenon in California). Such individuals may engage in illicit substance use at different rates compared to the predominantly unsheltered participants recruited for the study.
The use of interviewer administered questionnaires may have impacted the study findings. For example, participants may have underreported their substance use due to desirability bias or interviewer characteristics (e.g., gender).
This representative study shows that illicit substance use (especially methamphetamine) is highly prevalent among individuals experiencing homelessness in California. The results of the study also show that a substantial number of participants began using illicit substances regularly only after experiencing homelessness and had unmet substance use treatment needs. Taken together, these results suggest that illicit substance use may be both a cause and effect of homelessness. However, it is beyond the scope of these data to show why this may be the case, nor can the data provide clues on how to address this ongoing crisis. Future research to understand the underlying reasons for illicit substance use among those experiencing homelessness is critical for developing public health interventions.
For individuals and families seeking recovery: The present study suggests that at least some of those experiencing homelessness have unmet substance use treatment needs. Therefore, it may be important for those seeking recovery for themselves or their loved ones to look for low-barrier treatment programs that allow for person-centered goals. These may include low- or no-cost services (e.g., Salvation Army) or those that may not require abstinence for entry (e.g., Housing First style programs or syringe exchange programs). Such programs may be more accessible for those seeking treatment but are unable or not desiring to abstain from use. In addition, it may be beneficial to seek out care that is paired with stable housing, mental health support, and social services. Seek out providers that offer wraparound services or can refer you to programs that connect health care with housing and employment support.
For treatment professionals and treatment systems: The present study suggests that treatment professionals and those working in treatment systems that service those experiencing homelessness may do well to prioritize offering low-barrier substance use treatment, such as services on a sliding scale to facilitate their use by those with limited resources. In addition, implementing approaches to care that meet people “where they’re at” in the stages of therapeutic change may be effective in reducing unmet treatment needs among those experiencing homelessness, for example by offering medication-assisted treatment and overdose prevention tools (e.g., naloxone) for those using opioids. Outreach and mobile treatment services can help engage individuals who do not access traditional clinical settings.
For scientists: The present study underscores the need for scientists to investigate potential drivers of illicit substance use among those experiencing homelessness. Such drivers may include using illicit substances to cope with trauma and/or relapses precipitated by the stress of becoming homeless. Qualitative methodologies could offer valuable insight into the motivations for illicit substance use among this population. In addition, there is a need for scientists to investigate the barriers preventing those experiencing homelessness from seeking substance use treatment. It is likely that a combination of lack of health insurance, treatment affordability, and available providers contribute to unmet treatment needs. Empirical evidence is needed to better understand the specific reason why homeless individuals may be unable to access needed care, but from a hierarchy of needs perspective, it may be that housing that includes mental health and substance use treatment could be the ideal combination.
For policy makers: The present study suggests that policymakers may do well to consider strategies to expand services – especially addressing substance use – for those experiencing homelessness. Such efforts could include expanding outreach and mobile treatment services to engage individuals who cannot access traditional clinical settings. Additionally, there is a need for policy makers to expand wraparound services which can help provide affordable housing, metal health services and job assistance to those experiencing homelessness. Such programs may be critical for stopping the cycle of homelessness and addiction as they address the myriad challenges experienced by those experiencing homelessness simultaneously.
Illicit substance use is a significant challenge for those experiencing homelessness in the US while drug overdose is one of the leading causes of death among people experiencing homelessness. Concurrently, substance use can interfere with a person’s economic and social functioning making it challenging to find stable housing. In addition, some programs for the homeless (e.g., shelters) have strict abstinence policies which create a barrier for those with current substance use disorders to find shelter. There is also evidence that for some substance use initiation occurs after becoming homeless, suggesting that homelessness is a risk factor for problematic substance use and substance use disorders. Given these overlapping challenges, it is critically important to understand the scope of illicit substance use among people experiencing homelessness. Unfortunately, there has been a lack of research on this topic, with the most recent representative study being published in 1999. To address this knowledge gap, the current study utilized representative survey data to estimate patterns of illicit drug use and substance use treatment access among people experiencing homelessness in California.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the California Statewide Study of People Experiencing Homelessness project. This project, conducted by The University of California, San Francisco Benioff Homelessness and Housing Initiative, is the largest representative study of homelessness in the US in over 25 years. The goal of this project was to collect representative data on the scope of social and health issues for those experiencing homelessness to inform policies and programs to end adult homelessness in California. This project used a mixed methods design – both quantitative (surveys) and qualitative (in-depth interviews) data were collected, but only the survey data were analyzed for the present study. Data were collected between October 2021 and November 2022. Project staff conducted interviews in English or Spanish, or via interpreters (i.e., for other languages).
The California Statewide Study of People Experiencing Homelessness project authors utilized multiple approaches to recruit a diverse and representative sample. First, the authors divided the state into 8 distinct regions then selected 1 county per region in which to focus recruitment efforts. Counties were selected based on demographic makeup (i.e., were most representative of the overall population of California). The authors then compiled a list of venues within each county in which homeless populations were known to congregate (e.g., homeless shelters, non-shelter service providers, encampments, etc.). The project authors then sent interviewers to each venue to collect participant data. Interviewers were provided with a target number of interviews to complete per venue based on estimated venue size (e.g., 5 interviews for venues with 5-25 people experiencing homelessness). In addition, the project authors used respondent-driven sampling, a peer-referral based sampling strategy to recruit difficult to reach populations (e.g., LGBTQ individuals) and those that may have been missed in the venue-based sampling.
The main outcomes of the present study were lifetime and past 6-month illicit substance use and drug type (i.e., methamphetamine, nonprescription opioids [heroin, fentanyl,
or other opioid], and cocaine [cocaine/crack cocaine]). These outcomes were measured via a modified version of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test. The authors categorized Illicit drug use as regular (i.e., ≥3 times per week), occasional (i.e., >2 times per month and < 3 times per week, once or twice a month, or less than monthly), or no use (i.e., no self-reported illicit drug use). Participants who reported regular lifetime use of any substance were also asked when they had initiated use (i.e., before or after experiencing homelessness). In addition, the authors assessed unmet substance use treatment needs by asking participants if they wanted treatment but were unable to obtain it.
This study had a sample of 3,200 people experiencing homelessness (3,042 from venue-based recruitment and 158 from respondent-driven sampling). The sample mostly consisted of cisgender men (67.3%) followed by cisgender women (31.2%) and gender minorities (e.g., transgender) people (1.6%). The average age of participants was 46 years old. The study sample was racially and ethnically diverse – most participants identified as either White (27.9%), Hispanic/Latine (26.4%), or Black/African American (26.3%), with the remaining participants identifying as Multiracial and Multiethnic (14.3%), American Indian/Alaskan Native (2.9%), Asian/Pacific Islander (1.7%), or another race not listed (0.5%). Most participants reported being homeless for less than 3 years (64.3%) and were unsheltered (i.e., they slept in places not meant for human habitation, excluding vehicles, such as on the streets).
WHAT DID THIS STUDY FIND?
Illicit substance use was common among participants
Over 75% of participants reported using illicit drugs at least once during their lifetime, with 65% reporting lifetime regular use. Approximately 50% and 37% reported any and regular drug use in the last 6 months, respectively. Nearly a quarter reported using illicit substances regularly after becoming homeless.
Methamphetamine was the most used illicit substance
Approximately 65% of participants reported any lifetime methamphetamine use and 55% reported regular lifetime use. As shown in the graph below, recent (past 6 month) methamphetamine use was reported by 46% of participants, with 33% reporting regular use.
As shown in the graph below, 1/4 reported heavy drinking – 6 or more drinks on a single occasion. Half did not use any alcohol in the past 6 months.
Participants reported unmet substance use treatment needs
The graphs below depict participants’ treatment histories. While only 5% were currently in treatment or attending a 12-step mutual-help group, half had been to substance use treatment in their lifetime. Moreover, 23% reported being unable to receive substance use treatment despite wanting it at some point in their lives while 11% currently wanted treatment but were unable to receive it. For those currently wanting treatment but unable to receive it, this figure was even higher – 21% – for those with regular illicit drug use in the last 6 months.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study show that illicit drug use (particularly methamphetamine) is commonplace among people experiencing homelessness in California. The data also shows that those experiencing homelessness have unmet substance use treatment needs and that many participants began regular drug use after becoming homeless. While important, the present study can only tell us about the prevalence of illicit drug use – not drug use disorder – while giving some clues about potential unmet treatment needs among those experiencing homelessness. That is, these data cannot explain why this population may engage in illicit substance use nor offer clues on how to address illicit substance use. It is likely that a substantial proportion of this population suffer from severe mental illnesses including psychosis or bipolar disorders. It is possible that some use illicit substances to cope with trauma and therefore addressing the mental health needs of those experiencing homelessness may be one strategy to address emerging problematic substance use and substance use disorders. However, this is speculative and beyond the scope of the current study. Given the ongoing homelessness crisis, there is a desperate need to understand what contributes to the high rates of illicit substance use among those experiencing homelessness. Such knowledge can lead to the development of interventions to address the needs of those experiencing homelessness.
Irrespective of the underlying reasons, results of this study underscore how illicit drug use may both precede and perpetuate the cycle of homelessness. Although many participants (41.6%) reported initiating regular illicit drug use before first experiencing homelessness, a sizeable number (23.2%) began using regularly only after becoming homeless. This suggests that, for some, regular use may have been an effect of the psychosocial consequences of becoming homeless rather than a cause. The initiation of regular substance use after becoming homeless could be a means of seeking some kind of pleasure, psychological escape, or relief including coping with trauma (e.g., of losing shelter). That 1/5 of participants with regular drug use in the past 6 months wanted, but could not obtain, treatment is noteworthy – this is substantially higher than the general population, where only 4% of those with substance use disorder thought they needed treatment but could not obtain it (e.g., due to health insurance limitations). This observed unmet substance use treatment need among participants demonstrates the difficulty those experiencing homelessness face in overcoming problematic substance use. That is, without treatment those suffering from addiction will experience more obstacles to finding stable housing.
The present study was restricted to California and therefore has limited generalizability to the rest of the US. Evidence shows that the homeless population in California may differ from those experiencing homelessness elsewhere. For example, older adults (i.e., those 50+ years of age) comprise 40% of the homeless population in California, compared to 20% nationally. Furthermore, evidence shows that those experiencing homelessness in California are more likely to be unsheltered compared to those experiencing homelessness in other states. The reasons for these differences are unknown but are likely due to a combination of economic and environmental factors unique to California.
Utilizing a venue-based sampling strategy may have impacted the results. This strategy may have failed to recruit participants experiencing homelessness who would not be present at identified venues (e.g., shelters), such as those staying with friends/family or living in their vehicles (a common phenomenon in California). Such individuals may engage in illicit substance use at different rates compared to the predominantly unsheltered participants recruited for the study.
The use of interviewer administered questionnaires may have impacted the study findings. For example, participants may have underreported their substance use due to desirability bias or interviewer characteristics (e.g., gender).
This representative study shows that illicit substance use (especially methamphetamine) is highly prevalent among individuals experiencing homelessness in California. The results of the study also show that a substantial number of participants began using illicit substances regularly only after experiencing homelessness and had unmet substance use treatment needs. Taken together, these results suggest that illicit substance use may be both a cause and effect of homelessness. However, it is beyond the scope of these data to show why this may be the case, nor can the data provide clues on how to address this ongoing crisis. Future research to understand the underlying reasons for illicit substance use among those experiencing homelessness is critical for developing public health interventions.
For individuals and families seeking recovery: The present study suggests that at least some of those experiencing homelessness have unmet substance use treatment needs. Therefore, it may be important for those seeking recovery for themselves or their loved ones to look for low-barrier treatment programs that allow for person-centered goals. These may include low- or no-cost services (e.g., Salvation Army) or those that may not require abstinence for entry (e.g., Housing First style programs or syringe exchange programs). Such programs may be more accessible for those seeking treatment but are unable or not desiring to abstain from use. In addition, it may be beneficial to seek out care that is paired with stable housing, mental health support, and social services. Seek out providers that offer wraparound services or can refer you to programs that connect health care with housing and employment support.
For treatment professionals and treatment systems: The present study suggests that treatment professionals and those working in treatment systems that service those experiencing homelessness may do well to prioritize offering low-barrier substance use treatment, such as services on a sliding scale to facilitate their use by those with limited resources. In addition, implementing approaches to care that meet people “where they’re at” in the stages of therapeutic change may be effective in reducing unmet treatment needs among those experiencing homelessness, for example by offering medication-assisted treatment and overdose prevention tools (e.g., naloxone) for those using opioids. Outreach and mobile treatment services can help engage individuals who do not access traditional clinical settings.
For scientists: The present study underscores the need for scientists to investigate potential drivers of illicit substance use among those experiencing homelessness. Such drivers may include using illicit substances to cope with trauma and/or relapses precipitated by the stress of becoming homeless. Qualitative methodologies could offer valuable insight into the motivations for illicit substance use among this population. In addition, there is a need for scientists to investigate the barriers preventing those experiencing homelessness from seeking substance use treatment. It is likely that a combination of lack of health insurance, treatment affordability, and available providers contribute to unmet treatment needs. Empirical evidence is needed to better understand the specific reason why homeless individuals may be unable to access needed care, but from a hierarchy of needs perspective, it may be that housing that includes mental health and substance use treatment could be the ideal combination.
For policy makers: The present study suggests that policymakers may do well to consider strategies to expand services – especially addressing substance use – for those experiencing homelessness. Such efforts could include expanding outreach and mobile treatment services to engage individuals who cannot access traditional clinical settings. Additionally, there is a need for policy makers to expand wraparound services which can help provide affordable housing, metal health services and job assistance to those experiencing homelessness. Such programs may be critical for stopping the cycle of homelessness and addiction as they address the myriad challenges experienced by those experiencing homelessness simultaneously.