WHAT PROBLEM DOES THIS STUDY ADDRESS?
Animal studies and early human research suggest that GLP-1 medications like Zepbound, Ozempic, Mounjaro, and Wegovy, may dampen the rewarding effects that can help drive addictive behavior. However, most previous studies have focused on alcohol, and few have examined whether these medications might also help people who already have a substance use disorder. This study examined whether GLP-1 medications lowered the risk of developing substance use disorder, and substance-related harms among those already having a substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was an observational cohort investigation using electronic health record data from the United States Department of Veterans Affairs and included 606,434 patients with type 2 diabetes who newly started either a GLP-1 medication or, as a comparator, a sodium-glucose cotransporter-2 inhibitor (a type 2 diabetes medication that doesn’t affect appetite and reward pathways) based on filled outpatient pharmacy records. One set of analyses examined people without a recent history of the specific substance use disorder being studied to see whether a new diagnosis emerged over the following 3 years. Diagnosis codes were identified across a number of potential services including inpatient/outpatient, specialty care, and pharmacotherapy prescriptions. Presumably, these diagnoses were all determined by clinical judgment. A second set of analyses examined people who already had a substance use disorder to see whether they later had substance-related emergency department visits, hospital admissions, deaths, overdoses, or suicidal ideation or attempts. While this study was observational – i.e., participants were not randomly assigned to one medication or the other – the study used a complex weighting strategy to control for many variables that might influence the relationship between mediation prescription and substance use outcomes. The study population was mostly older, white, and male.
WHAT DID THIS STUDY FIND?
GLP-1s were associated with lower risk of new substance use disorder diagnoses
Across alcohol, cannabis, cocaine, nicotine, opioids, and other drug categories, people who started a GLP-1 medication were less likely to receive a new substance use disorder diagnosis over the following 3 years relative to those who started the comparison diabetes medication, sodium-glucose cotransporter-2 inhibitor. The risk reduction in the hazard ratio was in the range of about 13% to 25%, depending on the substance. The overall pattern was similar across age, sex, body size, blood sugar level, and the most commonly used medications within this drug class.
Looking at the broadest combined results, people who started a GLP-1 medication were less likely to develop any substance use disorder over the next 3 years compared to the people who started the comparison diabetes medication. However, this does not mean there were 25% fewer cases of substance use disorder among those taking GLP-1s. But rather the relative risk of developing a substance use disorder was 25% lower for those taking GLP-1s compared to the comparison medications. Overall, the reduction was modest but meaningful at the population level, amounting to about 7 fewer cases of any substance use disorder (including nicotine) for every 1,000 people treated.
GLP-1s were associated with lower risk of complications for those already having a substance use disorder
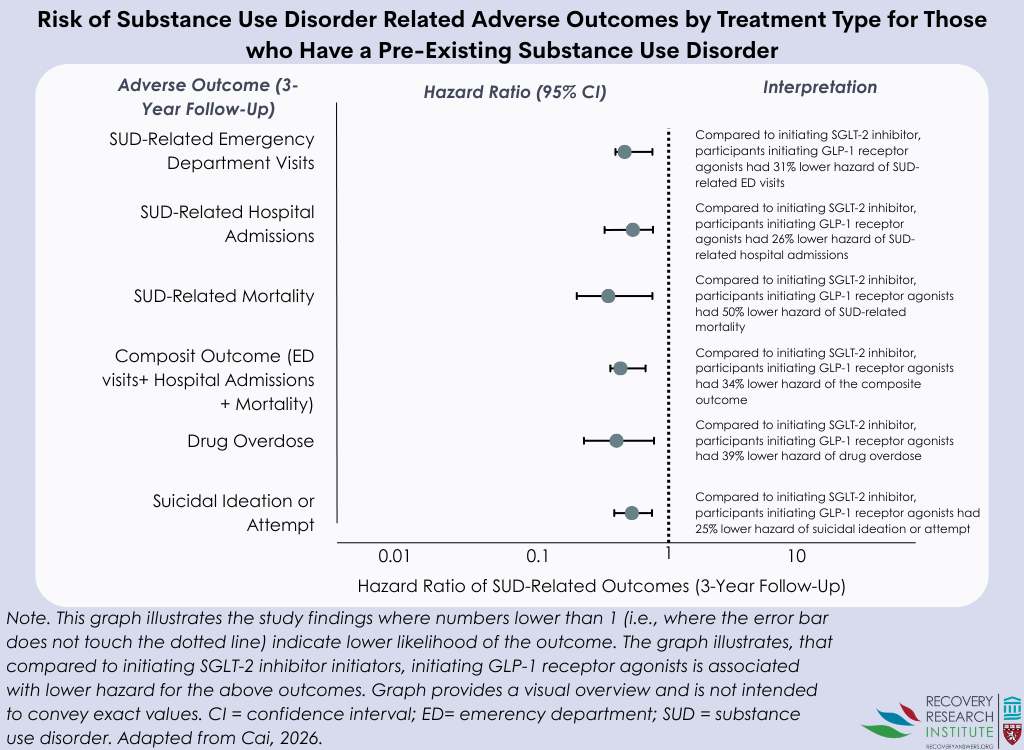
Among people who already had a substance use disorder, starting a GLP-1 medication was associated with fewer substance-related emergency department visits, hospital admissions, overdose events, episodes of suicidal ideation or attempts, and lower mortality (see graph below). In general, the reductions in these serious outcomes were larger than those seen for new diagnoses, falling in the range of about 25% to 50%. Again, however, this does not mean there were 50% fewer instances of substance use disorder complications. For the study’s main combined adverse outcome of substance-related emergency department visits, hospital admissions, or death, this worked out to about 12 fewer serious events for every 1,000 people treated over 3 years.
Of note, there was a complex set of analyses to determine if the degree to which individuals adhered to their medication affect results. Overall, these sensitivity analyses yielded the same conclusions.
Important cautions when interpreting the findings
These results are promising, but while compelling the study does not show that the medication itself caused the differences. People were not randomly assigned to treatment, and substance use disorder is often underdiagnosed in routine care, which means some cases may have been missed. Additionally, some of the smaller subgroup analyses included relatively few events. Also, most participants were men and all were US combat veterans.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings from this and similar observational studies extend preliminary alcohol-specific findings potentially to other substance use disorders. This may strengthen the case for studying GLP-1 medications as potentially helpful tools for both prevention and reducing the consequences of substance use in addiction care, especially for people who already have a clear medical reason to receive them. At the same time, this was an observational study, so the results should be viewed as encouraging and hypothesis-generating rather than practice-changing on their own. In addition, we cannot know from this study whether the effects of GLP-1s are moderated by type of substance use disorder (e.g., alcohol vs. opioid) or level of severity. The next step will be to carefully design randomized trials that test whether these medications truly lower substance use disorder risk and improve clinical outcomes, while also weighing those possible benefits against known medication side effects.
BOTTOM LINE
In this large Department of Veterans Affairs study, GLP-1 medications were associated with modestly lower risk of both new substance use disorder diagnoses and serious substance-related problems among those who already had a substance use disorder. The results are encouraging, but randomized controlled trials are needed before these medications can be recommended specifically for addiction treatment.
- For individuals and families seeking recovery: This study suggests that GLP-1 medications may modestly lower addiction risk and risk of addiction-related problems for those who already have a substance use disorder. At the same time, these medications are not yet approved to treat addiction and can have significant side effects. Cognitive Behavioral Therapy and FDA-approved medications may be more suitable, at present, for individuals trying to reduce or stop substance use.
- For treatment professionals and treatment systems: This study suggests that GLP-1 medications may modestly lower risk for developing substance use disorder and risk of addiction-related problems for those who already have a substance use disorder. While not definitive, these results support closer attention to this drug class as clinical trials move forward.
- For scientists: This study provides a modest observational signal across multiple substances and across both prevention and services used to reduce harm outcomes. It also offers a useful roadmap for future randomized trials, mechanistic work, and subgroup analyses designed to identify who benefits most and which outcomes are most responsive.
- For policy makers: These findings point to a potentially important dual benefit for some people who already qualify for GLP-1 medications because of type 2 diabetes. Policy discussions should focus on supporting rigorous trials and ensuring that future decisions balance possible addiction-related benefits with cost, access, and medication safety.
CITATIONS
Cai, M., Choi, T., Xie, Y., & Al-Aly, Z. (2026). Glucagon-like peptide-1 receptor agonists and risk of substance use disorders among US veterans with type 2 diabetes: Cohort study. BMJ, 392. doi: 10.1136/bmj-2025-086886.
 Medications originally developed for type 2 diabetes are now drawing attention for their possible effects on substance use craving and reward. This study examined whether people who started a glucagon-like peptide-1 receptor agonist (GLP-1) like Zepbound or Ozempic were less likely to develop a substance use disorder, and whether people who already had a substance use disorder had fewer serious complications.
Medications originally developed for type 2 diabetes are now drawing attention for their possible effects on substance use craving and reward. This study examined whether people who started a glucagon-like peptide-1 receptor agonist (GLP-1) like Zepbound or Ozempic were less likely to develop a substance use disorder, and whether people who already had a substance use disorder had fewer serious complications.