
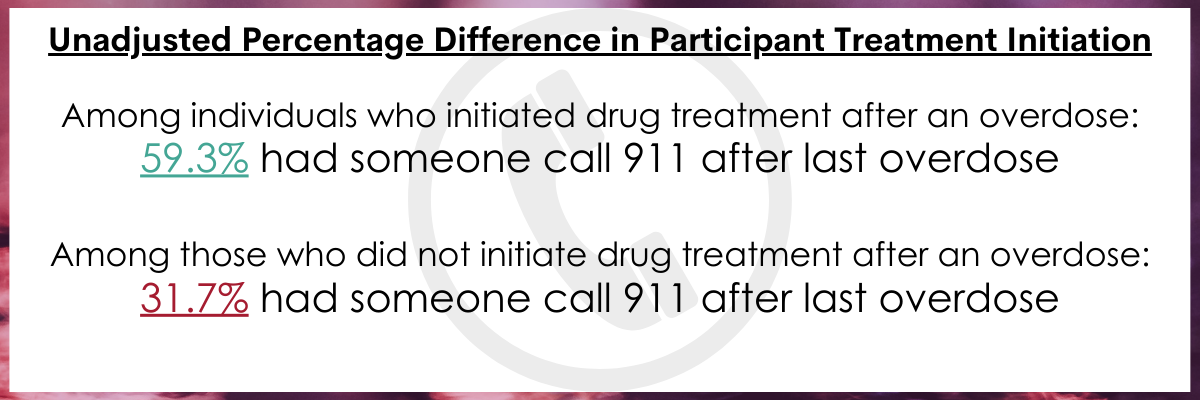
Having someone call 911 after an overdose increases likelihood of treatment engagement
A non-fatal overdose can be a critical time to engage someone in substance use disorder treatment. Yet, despite this opportunity, many individuals who experience an overdose do not engage in follow-up care, and this is especially true for individuals living in rural areas. To increase treatment engagement and to enhance targeted outreach for people who inject drugs in rural communities, the researchers in this study identified factors associated with entering treatment after a recent overdose.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
A non-fatal overdose can be a critical time for an individual to engage with treatment services to address their substance use for several reasons. First, on a personal level, this major life experience can be highly motivating to seek additional services to prevent it from happening again. Second, it can be a time to garner additional support for getting treatment from friends and loved ones, if they witness or learn about the overdose. Third, if emergency service personnel respond to the overdose, their involvement can provide a direct connection to other treatment service providers who may be able to suggest and help enroll someone in appropriate follow-up care.
Despite these motivating factors and opportunities, those who experience a non-fatal overdose often do not engage in follow-up services. This treatment gap is especially wide for individuals who live in more rural areas for several reasons. Health insurance coverage may not be broad enough to cover such treatment, there may be fewer treatment providers than in urban areas, and it may be more difficult to access appropriate treatment services. Alternatively, the available treatment services may not be ones that individuals in rural areas are comfortable with or aware of. There may also be more stigma in these areas around injection drug use and those who might wish to seek treatment may feel their experience would not remain confidential. Much of the prior research in this area has focused on urban populations. Consequently, research that can help identify as of yet unknown factors influencing the lack of access to follow-up treatment after a non-fatal overdose for individuals living in rural areas could be of immense value.
To this end, this study examined factors related to entering any form of drug treatment after a recent overdose among individuals who inject drugs and who reside in a rural county in West Virginia. It was part of a larger, overall effort to create and implement tailored interventions that could increase treatment engagement among individuals in rural communities.
HOW WAS THIS STUDY CONDUCTED?
This was secondary data analysis from a 2018 Population Estimation study, a type of study which aims to estimate the prevalence of the population of specific illness or behaviors. In this population estimation study, the researchers used a “capture-recapture” approach to identify individuals who injected drugs in a rural Appalachian county in West Virginia. The capture-recapture approach is when study participants are sampled to represent the larger population of individuals with a certain condition (or behavior) and then the researchers attempt to find the same population of participants after a certain amount of time. The capture-recapture for this study took place in June and July and sampled from the Cabell-Huntington Harm Reduction Program and local community settings. The researchers included individuals who were (1) adults, 18 years old or older and (2) who ever used drugs by any route of administration. Although the overall population estimation study sampled 420 individuals, only 43% of those were eligible for this study that focused on individuals who had both injected drugs and experienced at least one non-fatal overdose in the past 6 months.
The primary outcome of interest was whether the individual had started drug treatment in the 30 days following their most recent overdose experience.
Drug treatment was considered to be any form of service or support, including detoxification, inpatient or outpatient treatment, and medication treatment.
The study team also collected information on participant characteristics and behaviors they thought might influence treatment engagement: age, gender, race, ethnicity, high school education, sexual orientation, employment status, relationship status, age of first injection, drugs injected in past 6 months, how many people they typically used drugs with, number of times they had overdosed in the past 6 months, and whether 911 was called during the most recent overdose.
The study sample included 179 individuals in Cabell County, West Virginia who inject drugs and who reported that they had overdosed in the past 6 months. They were on average 35.7 years old and primarily male (60.3%), non-Hispanic white (83.7%), and high school educated (74.7%). Of this group, about 12% identified as a sexual minority, and 53% were single. These individuals appeared to have an extensive drug use history in that on average, individuals reported their first drug injection was over 10 years ago. The most frequently injected drugs in the past 6 months were heroin (94.4%), crystal methamphetamine (82.7%), and fentanyl (74.3%). All participants indicated they had used at least one type of opioid in the past 6 months.
WHAT DID THIS STUDY FIND?
Many overdose experiences, but low treatment engagement.
Among this sample of individuals who inject drugs and who had overdosed in the past 6 months, on average, participants reported nearly 1 overdose per month in that time frame (5.2 overdoses in the past 6 months). The majority (75%) of participants reported that they typically used drugs with at least one other person and just under half (40.8%) of participants reported that someone had called 911 after their most recent overdose. Despite the high number of overdoses in a short period, only 33% of participants started any form of drug treatment in the month following their most recent overdose: the number of overdoses experienced was not different between those who did and did not start treatment.
Treatment engagement predicted by individual characteristics.
Drug treatment engagement after someone’s most recent overdose experience was predicted by three main factors in models that controlled for participant age, gender, and relationship status.
First, an individual was the most likely to engage in treatment if someone (self or other) had called 911 after their most recent overdose. Second, if an individual had recently injected buprenorphine or Suboxone (i.e., non-medical use of these substances), they were also more likely to engage in treatment. Finally, older individuals were less likely to engage in treatment after a recent overdose experience.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of individuals who inject drugs and who had also experienced an overdose, the rate of non-fatal overdoses was very high, nearly once a month in the previous 6 months. Yet, similar to previous research in an urban environment, a third of participants in this rural area did report engaging in some form of drug treatment after their most recent overdose in the past 6 months. Among these participants, the strongest predictor of treatment seeking was a call to emergency services for their overdose. This call suggests some level of social or community capital, as it suggests that these individuals who engaged in treatment had access to social support (to make the call) and/or to community resources where emergency service use was available, and they were able to make the call themselves. As well, the fact that the second strongest predictor was recent non-medical use of buprenorphine or Suboxone through injection, does suggest that these individuals have access to these medications and may have some community capital already present. Use of the medication in this way may also mean some level of individual motivation to change their substance use by injecting something less potent (for example, by injecting buprenorphine instead of heroin). Follow-up qualitative research with these individuals may help to further understand why some were able to engage in treatment and others were not.
As most participants reported using substances with at least one other person, this may be a form of social support for recovery that can be used to better facilitate approaches to reduce fatalities and support people in seeking care for their substance use. For example, harm reduction approaches such as by increasing education around safer drug use practices (e.g., when using substances, having at least one other person nearby), developing syringe service programs, and implementing Naloxone training and distribution in communities may be one way to build social network capacity in rural communities. Furthermore, community recovery capital could be built by creating stronger links between emergency and follow-up drug treatment services and structuring these so that they are more assertive and systematic, and thus, more likely to be used. Using a cascade of care approach which focuses on improving services from a systems-level to break down public health silos and reduce barriers to access may be one way to more systematically address this issue for rural populations. Indeed, especially for individuals that have barriers to accessing care, and in light of data that suggests that overdose deaths may be increasing in rural regions, a whole-community approach, and one that focuses on needs of rural areas, seems necessary to address these service gaps.
Finally, despite the findings that there is some degree of treatment engagement among rural individuals after an overdose, it is important to note that this study used a very broad definition of treatment and captured what the participants’ considered treatment. Thus, we do not know whether the treatment engaged in was evidence-based or even effective for those who engaged, and we do not know the ultimate recovery outcomes, including substance use as well as other areas of health and well-being, for those individuals.
- LIMITATIONS
-
- The researchers used a broad definition of drug treatment and as a result, inferences can only be drawn about treatment engagement based on the participant’s understanding of treatment, not whether this treatment was appropriate or evidence-based. As well, there is no way of knowing whether treatment was successful or not. So, while the study demonstrates factors that lead to treatment engagement after an overdose, it does not identify what factors might lead to treatment maintenance or further distal outcomes such as long-term remission from substance use among rural individuals.
- As this is self-report overdose data, a highly complex experience that can involve losing consciousness, there may be some inaccuracies related to the experience and events surrounding it (e.g., whether/when/who called 911).
- A variety of additional important factors to understanding overdose and treatment engagement were not collected. For example, the research team did not collect comorbid mental health data, which is a risk factor for overdose. This leaves an opportunity for future research to address whether these factors may influence treatment engagement for rural populations.
BOTTOM LINE
In this study, the researchers found that among a rural sample of individuals who inject drugs in West Virginia, only a third engaged in treatment after a non-fatal overdose. Those who reported engaging in treatment were most likely to do so if someone had called 911 during their most recent overdose, suggesting that in those places there was access to emergency medical services and other forms of social network support. As well, those who had recently engaged in non-medical use of buprenorphine or Suboxone were also more likely to engage in treatment after a recent overdose, suggesting that prior connection to the treatment system may be helpful in re-engaging with it.
- For individuals and families seeking recovery: An overdose event sometimes, but not always, leads to initiating change in substance use and engaging in treatment. If you or a loved one has experienced a non-fatal overdose, it is important to prepare for the future: the research in this study shows that individuals can have several overdoses before seeking treatment and other research demonstrates how fatal even a single overdose can be. Harm reduction approaches such as being trained in the use of Naloxone and carrying it or in offering to be with a friend while you know they are using may show your support for them to prevent a future overdose fatality. Using the time following an overdose to seek help or to seek help for others may also help initiate their recovery journey.
- For treatment professionals and treatment systems: These findings suggest a need for building in more systematic community recovery capital supports to address services gaps and needs, as well as targeting specific settings/events where these services are most likely to be accessed. In the case of rural communities, providing training and education to first responders and emergency room personnel on creating an opportunity for assertive linkage to care and follow-up may be an effective approach in increasing post-overdose treatment engagement and reducing future fatalities. As well, providing education and training to those seeking treatment and any accompanying family or friends on the use of Naloxone may be one way to begin to build community capacity to reduce overdose deaths.
- For scientists: TThe findings in this study demonstrate the potential opportunity of emergency service intervention to increase access to treatment for some individuals following an overdose. Yet, there are many unexplored factors which could influence this relationship, and these are both at the individual level (e.g., motivation for change) as well as at the social (e.g., network recovery support/barriers) and community levels (e.g., existing system of linkage to care initiated by a 911 call). Future research, especially qualitative research after a non-fatal overdose, may help to fill in some of these gaps in knowledge and lead to future interventions to support assertive linkage to treatment.
- For policy makers: The findings from this research study suggest a need for advocating for and funding system-level recovery supports in communities to address services gaps and needs, and to target rural communities with these efforts, including through expanding access to the life-saving Naloxone. Future funding could be used to examine the cost-benefit of providing training, education, and infrastructure to healthcare providers on how to create an opportunity for assertive linkages to care and follow-up.
CITATIONS
Allen, S. T., Wedlock, P. T., White, R. H., Schneider, K. E., O’Rourke, A., Ahmad, N. J., . . . Sherman, S. G. (2021). Engagement in drug treatment following nonfatal overdose among people who inject drugs in Appalachia. International Journal of Drug Policy, 93, 103176. doi: 10.1016/j.drugpo.2021.103176
