
Benefits of the “Therapeutic” Alliance Between Sponsor & Sponsee in 12-step Groups
12-step mutual-help groups, like Alcoholics Anonymous, are freely available and have proven to be valuable recovery support resources.
A sponsor is a fellow 12-step mutual-help member with lived recovery experience that is intended to guide a newer member (i.e., with less recovery time) through the 12-step program, and in some cases, provide advice and support when needed.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Randomized trials have shown, for example, that interventions linking individuals with these community-based groups produce outcomes on par with, or better than, other active psychosocial treatments like cognitive-behavioral therapy. More recently, researchers are investigating what aspects of 12-step participation are most helpful. Having a sponsor appears to be one of these valuable recovery-supportive 12-step activities.
Because relatively little is known about how having a sponsor is beneficial, Kelly and colleagues investigated whether the quality of the relationship, or “therapeutic alliance”, an individual has with his/her sponsor may contribute to the chances of further AA participation and ongoing recovery, similar to the ways in which a relationship with one’s therapist can positively influence treatment benefit beyond the specific treatment technique.
HOW WAS THIS STUDY CONDUCTED?
The researchers conducted a naturalistic SUD treatment study (i.e., observing and measuring participants that sought treatment as it was naturally provided, without manipulating the treatment being delivered) of 302 young adults aged 18-24 (sometimes referred to as “emerging” adults) that attended a residential SUD treatment program. They completed follow-up assessments 3 months, 6 months, and 12 months after treatment discharge. Researchers’ analyses focused on a subset of 153 emerging adults that had a sponsor and completed measures assessing contact with one’s sponsor and one’s perceived relationship with his/her sponsor (i.e., the “sponsor alliance”), for at least one of the three follow-ups.
The sponsor alliance was measured by a novel 10-item self-report measure adapted from the short-form of the Working Alliance Inventory, which has been used extensively in the science of psychotherapy to measure the therapeutic alliance. The Sponsor Alliance Inventory covers the bond between sponsor and sponsee (the individual being sponsored), as well as the extent to which the sponsee sees their goals – and the sponsor’s understanding of those goals – as aligned.
Items asked participants to rate their level of agreement with statements such as:
- “My sponsor and I agree about the things I will need to do in AA/NA to improve my situation”
- “I believe my sponsor likes me” (see here for more information on the measure).
The researchers analyzed whether sponsor alliance was related to 12-step attendance, active involvement beyond attendance (e.g., socializing with other members outside of meetings), and abstinence measured by percent days abstinent from alcohol and other drugs during a follow-up period. These analyses adjusted for several factors that might be correlated with sponsor alliance and also influence the outcomes (i.e., a statistical confound), including demographic characteristics and level of commitment to abstinence upon treatment intake.
WHAT DID THIS STUDY FIND?
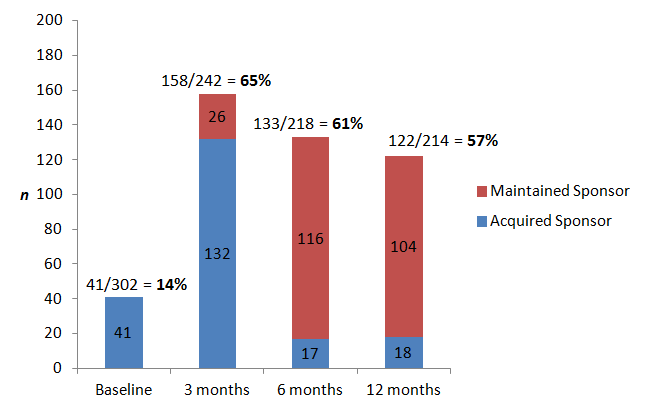
First individuals that had a sponsor at any point in the study, overall (n = 208), were more clinically severe (e.g., more substance use consequences) and more motivated for abstinence upon entering the study than those who did not have a sponsor (n = 92). Also, for those who did not have a sponsor coming into the study, about two-thirds acquired one by the 3-month follow-up. See figure below for acquisition and maintenance of a sponsor during the 1 year following residential substance use disorder (SUD) treatment.
Having a sponsor was related to more attendance and involvement in 12-step groups, & abstinence over time.
Sponsor alliance, too, was related to 12-step participation and abstinence, even when adjusting for the confounds mentioned above, as well as simply having contact with one’s sponsor outside of 12-step meetings.
The strength of the relationship between sponsor alliance and abstinence increased over time, as one moved further in time from their treatment discharge. In other words, the relationship was stronger 1 year after treatment discharge than it was 3 months after treatment discharge. In line with anecdotally-derived advice in 12-step groups about the importance of getting a sponsor, scientific studies have also shown that having a sponsor is likely a key 12-step recovery activity. This research demonstrating the value of engagement with a sponsor has even shown its advantage compared to, or over and above, other types of 12-step activities like working the 12 steps (as examples, see studies by Zemore et al. here and Tonigan & Rice here).
This Kelly et al. study extended the evidence of sponsorship-related recovery benefit to a young adult sample. It also highlighted that the nature and quality of this bond may be related to positive recovery outcomes like abstinence, and are certainly worthy of further study.
This study suggests the benefits from having a sponsor could come from the relationship itself – that is, from the support and empathy offered by the sponsor and felt by the sponsee.
- LIMITATIONS
-
- There are two important cautions in interpreting and applying these findings. First, these young adult residential treatment seekers with a sponsor were more clinically severe and motivated for abstinence than those without a sponsor. So it cannot be determined whether these findings generalize to other samples (i.e., that are more ambivalent about change).
- Second, as mentioned above, the relationships between sponsor-mediated variables like the alliance, and outcomes over time (e.g., abstinence) were measured at the same point in time; that a better alliance with one’s sponsor caused better outcomes cannot be determined with certainty from these analyses. One important note for future research: time-lagged correlations (i.e., unadjusted) between sponsor alliance at 3 months/6 months and abstinence at 6 months/12 months, respectively, were modest (~ r = .2) but significant, while the reverse correlations (e.g., between abstinence at 6 months and sponsor alliance at 12 months) were not significant. Thus, it seems more likely that having a good relationship with one’s sponsor is contributing to increased abstinence and not the other way around, though this hypothesis certainly needs to be tested.
NEXT STEPS
Next, researchers might investigate what factors explain the effect of having a sponsor on positive recovery outcomes in formal statistical mediation models, including the sponsor alliance, as well as other sponsor-mediated activities, like phoning or texting him/her to help cope with a craving to drink or use drugs.
BOTTOM LINE
- For individuals & families seeking recovery: While more research is needed on the nature of the relationship between sponsors and sponsees, based on this study, having a sponsor you feel supported by emotionally, and that understands your recovery goals, could positively impact your recovery outcomes, including abstinence. This study only looked at sponsorship during the first year after attending residential treatment, so it is not clear whether this applies beyond that time frame.
- For scientists: This study used longitudinal models to test the contemporaneous association between the relationship between sponsor/sponsee and abstinence. While models controlled for potential confounds, and also showed a unique effect of this sponsor alliance over and above simple contact with one’s sponsor, findings cannot speak to causality due to the lack of temporal precedence between the putative cause (i.e., alliance) and effect (i.e., abstinence). However, time-lagged bivariate correlations suggested the alliance may be contributing to increased abstinence, though the reverse is unlikely. Future research will be needed to better tease this apart.
- For policy makers: This study was among the first to delve further into the impact of the sponsor/sponsee relationship on recovery outcomes among individuals attending 12-step mutual-help groups. Results suggest the alliance between sponsor and sponsee may be playing a key role in one’s recovery. Consider devoting funding to help illuminate the recovery-supportive processes and activities occurring in 12-step mutual-help organizations, including but not limited to sponsorship.
- For treatment professionals and treatment systems: This study suggested the relationship between individuals and their 12-step sponsors could be important to recovery outcomes. While more research is needed before strong recommendations can be offered, you may wish to discuss this particular 12-step activity in more detail with your patients, and inquire about the nature and quality of this relationship.
CITATIONS
**Note: One or more authors of this study were Recovery Research Institute Staff, including the director and/or other research scientists. As with all summaries, staff made the greatest possible effort to recognize and account for any potential biases in the review of this article.
