Alternative non-drug rewarding activities associated with lower opioid craving and use
People in recovery from opioid use disorder may have difficulty experiencing pleasure, though it is unclear whether such experiences are present all the time. This study explored whether different patterns of daily rewarding activities were associated with recovery outcomes, including opioid use, opioid craving, mood, and quality of life.
Opioids – including both prescription opioids like oxycodone and illicit opioids like heroin – increase feelings of pleasure in the short-term due to their activation of opioid pleasure receptors in the brain in addition to their analgesic, pain relief effects. These naturally occurring opioid receptors are also important for the general experience of reward and are activated by everyday pleasures such as eating ice cream or laughing at a funny joke. With repeated use of opioids, the brain reduces the number of neurotransmitters at opioid receptor sites (i.e., down-regulation) thereby reducing the experience of pleasure when these same previously pleasurable activities (e.g., eating ice cream) are performed (a process known as neuroadaptation). For some, this persists, and can last for quite a while, when people make a recovery attempt which can impact the experience of more normal levels of reward from everyday pleasures. As a result, many people in recovery from opioid use disorder report an impaired ability to experience pleasure. This difficulty may even persist among those receiving opioid agonist therapies, such as buprenorphine (e.g., Suboxone) or methadone, which also stimulate opioid receptors but tend to do so in a more consistent, stable, and controlled fashion than the peaks and valleys that are experienced by patterns of illicit opioid use.
Research has shown that fun, substance-free rewarding activities can compete to some degree with the rewards from substances, and if made more available and accessible it might be useful in aiding recovery by stimulating those down-regulated receptors.
Importantly, feelings of pleasure, as well as access to reward, may fluctuate throughout the day, and different patterns of reward experience may predict recovery outcomes and inform clinical interventions. While many studies have investigated the protective effects of rewarding substance-free activities over extended periods of time, their benefits of course are likely to manifest in the short term – for example, within the same day. This study examined whether different patterns of daily non-drug reward was associated with recovery outcomes, including opioid use, opioid craving, mood, and quality of life.
HOW WAS THIS STUDY CONDUCTED?
This study used a naturalistic design to assess non-drug activities, substance use, and other recovery outcomes each day for 3 weeks in 153 adults who were receiving opioid agonist treatment – primarily methadone – for opioid use disorder.
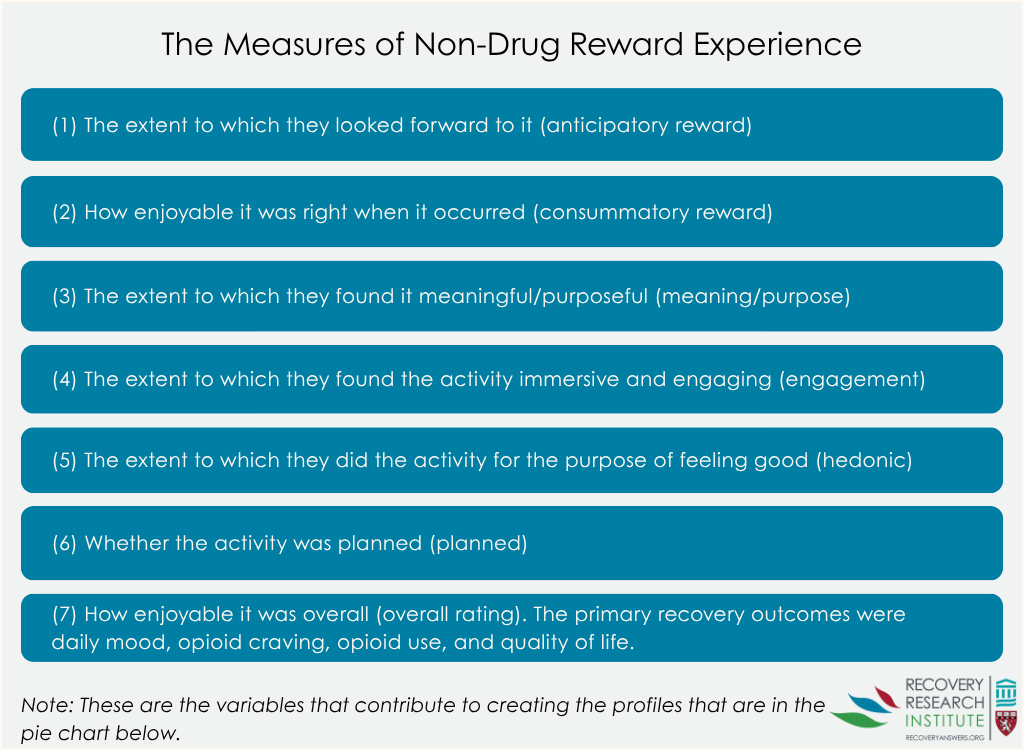
After completing a baseline survey, patients completed a brief survey every morning for 21 days. During the baseline survey, the patients reported on how long they have been in recovery and their overall lack of feelings of pleasure, often called, “anhedonia”. In each daily diary survey, participants reported on their experience with non-drug reward from the previous day. Participants were first asked how many things they did the day before that brought them pleasure or enjoyment. From this, for only the most rewarding activity, participants provided information on 7 facets of the rewarding experience on a 1 to 5 scale: (1) the extent to which they looked forward to it (anticipatory reward); (2) how enjoyable it was right when it occurred (consummatory reward); (3) the extent to which they found it meaningful/purposeful (meaning/purpose); (4) the extent to which they found the activity immersive and engaging (engagement); (5) the extent to which they did the activity for the purpose of feeling good (hedonic); (6) whether the activity was planned (planned); and (7) how enjoyable it was overall (overall rating). The primary recovery outcomes were daily mood, opioid craving, opioid use, and quality of life.
First, the authors used a statistical approach to identify patterns of day-level reward experience. Each of the seven reward indicators described above were used to identify these patterns. Second, analyses examined whether the proportions of days they experienced an opioid craving and of days they used opioids were associated with each day-level reward pattern, controlling for baseline anhedonia and the amount of time the person has been in recovery. Such statistical adjustments help to isolate the effect of interest – i.e., whether non-drug reward is independently related to opioid craving and use. Third, the authors explored whether these daily non-drug reward patterns were associated with same-day mood and quality of life.
The sample was, on average, 41 years old, primarily white (84%; 15% Black, 2% Native American, 1% Hispanic) and contained more females (57%) than males (43%). Participants were taking either methadone (85%) or buprenorphine (15%), and 65% had been in recovery for at least 1 year.
WHAT DID THIS STUDY FIND?
Many days included highly rewarding, planned activities
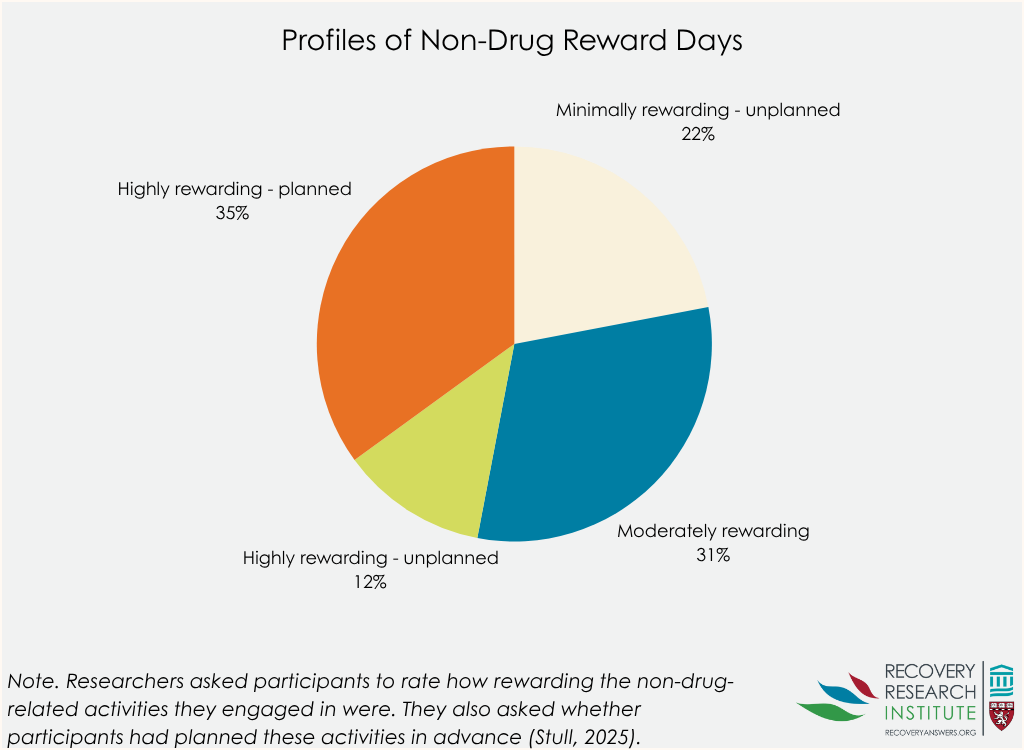
The authors identified 4 patterns of reward that occurred across people. The most common pattern included high ratings on every reward indicator and accounted for 35% of days across all participants (“Highly Rewarding-Planned” Pattern). The next most common had slightly lower mean ratings across all indicators and accounted for 31% of days (Moderately Rewarding Pattern). The Minimally Rewarding-Unplanned profile accounted for 22% of the days and was defined by low average ratings across indicators. Finally, 12% of the days were characterized by a Highly Rewarding-Unplanned profile with moderate to high ratings across all reward indicators and low scores on the “planned” indicator.
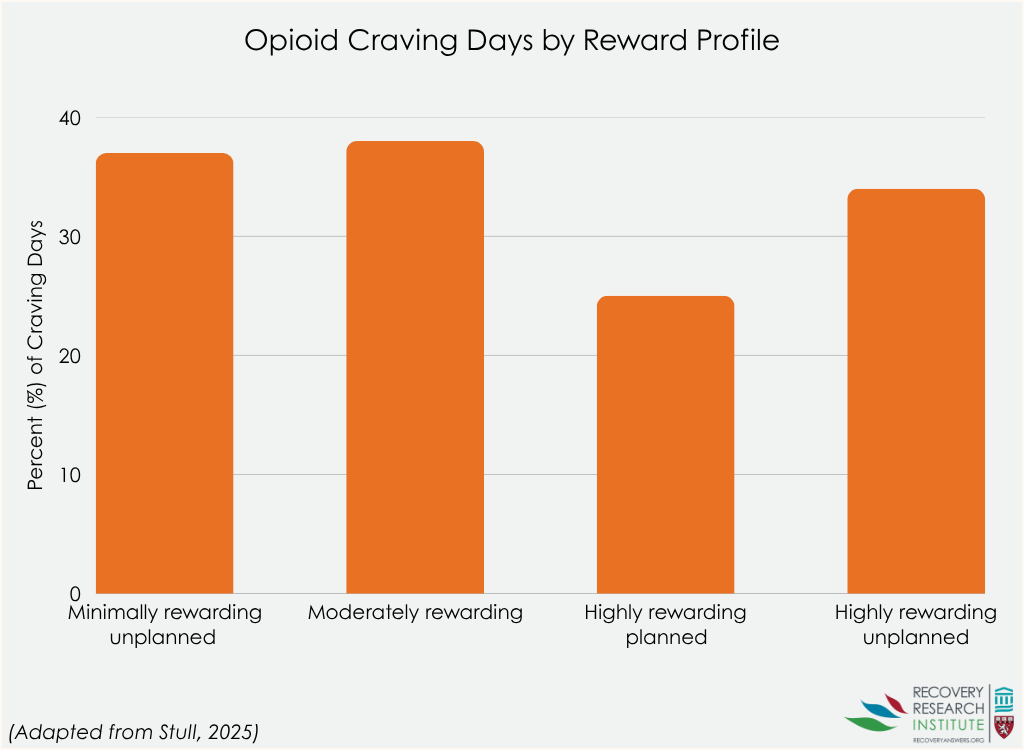
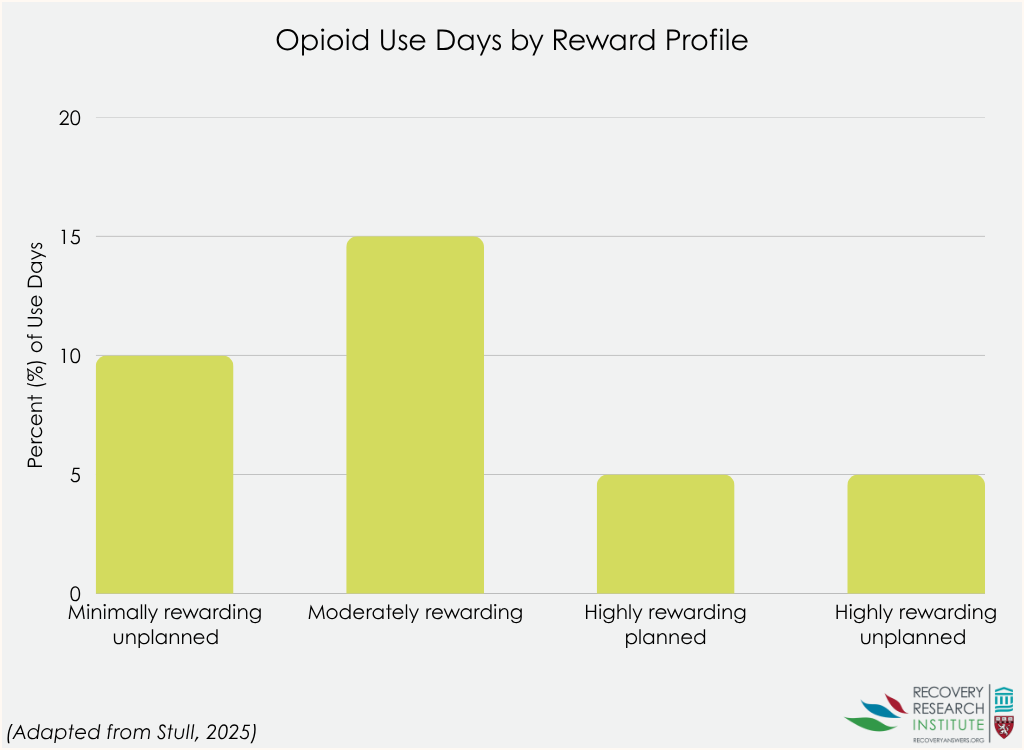
The planned highly rewarding daily pattern was associated with less opioid craving and use
Higher baseline pleasure scores were associated with a greater likelihood of experiencing a highly rewarding planned day relative to a moderately rewarding one – each additional point on the scale was associated with 4% increased odds of having a planned, highly rewarding day – or minimally rewarding day, which was associated with 5% increased odds. Also, opioid craving was associated with reward patterns, such that people who reported more craving had 60% lower likelihood of experiencing the highly rewarding planned pattern relative to the moderately reward pattern. Also, participants who reported more opioid use had an 80% lower likelihood of experiencing the highly rewarding planned pattern relative to the moderately rewarding one. Somewhat surprisingly, given the easier bar to surpass than moderately rewarding days, planned highly rewarding days were no more likely than minimally rewarding, unplanned days for people with fewer opioid use days.
Days characterized by high reward were associated with higher positive mood, lower negative mood, and greater quality of life
Days characterized by planned, high reward were associated with greater positive mood and quality of life, and lower negative mood, relative to days characterized by moderate reward or unplanned minimal reward. While the effects on negative mood were relatively modest, the effects on positive mood were almost 1 point (on a 1 to 5 scale) and the effects on quality of life were 21 points (on an 8 to 40 scale). Days characterized by planned, high reward were associated with greater positive mood and quality of life relative to days characterized by moderate reward or unplanned minimal reward; unplanned high reward days were associated with lower positive mood relative to days characterized planned high reward.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results suggest that people recovering from opioid use disorder and taking an agonist medication, such as methadone or buprenorphine, experience variability across days in the experience of reward. Almost half of the days were consistent with patterns of high reward, either planned or unplanned. On the other hand, in the same group of people, almost 1/4 of days were consistent with an unplanned and minimally rewarding pattern of reward . Although early recovery is often thought to be marked by a considerable lack of pleasure, these results suggest that people in recovery from opioid use disorder have the capacity to experience highly pleasurable non-drug reward, albeit these experiences may be inconsistent. Also, some have suggested that people taking agonists like methadone or buprenorphine may experience pleasure in recovery in a more muted fashion, because of the medication. Although this study cannot speak to this, as there was not a recovering opioid use disorder group who were not taking agonist medication, the results nonetheless do suggest that even if such muting or compression of pleasure may be occurring to some degree, these individuals nevertheless experienced attainable high pleasure variation and this was correlated with lower craving and less illicit opioid use. Finally, while 65% of these individuals had 1+ year in recovery, indicating greater potential for non-drug rewarding activities, surprisingly , whether someone had 1+ year or less than 1 year in recovery did not predict whether someone experienced a rewarding day. Overall, people considering recovery from opioids may benefit from knowing that they will likely be able to experience pleasures in alternative ways if they take a step toward abstinence.
One important caveat is that the activities were measured on the same day as opioid and other recovery outcomes. Thus, it is possible that positive experiences early in the day (e.g., restful sleep, taking one’s medication as prescribed, etc.) led to opportunities for fun, rewarding activities later. Also important is that there appeared to be an extra boost from planned rewarding activities, compared to those which were not planned, suggesting someone is already doing well, then plans a fun activity. For example, people who make new, recovery supportive friends – a longer-term process – may be better positioned to plan fun activities . Also of note is that the study used only the most rewarding activity each day, rather than combining all the activities to determine the degree to which somebody engaged in pleasurable activities – this might overestimate the relationship between fun, planned activities and reduced opioid use and craving.
Nevertheless, these findings are important because recovery from opioid use disorder can be difficult, and many people make multiple recovery attempts before being able to sustain recovery over the long-term, in part, because of lack of alternative reward accessibility and engagement with such alternatives. Early recovery is a period of high risk for return to use and overdose, which increases the urgency to identify mechanisms to improve success rates.
The results showed that days with high reward were associated with lower craving and opioid use and associated with higher quality of life and positive mood. Although, as noted above, the direction of effect here cannot be determined from this study design, the finding that daily non-drug reward may be an important buffer against return to use during recovery from opioid use disorder makes sense and is in keeping with people’s reported experiences. Some interventions, such as cognitive behavioral therapies or behavioral activation, also teach skills such as planning and goal setting to help people identify highly rewarding activities and to plan such activities. Therapies that help people reflect on their day’s positive experiences (e.g., gratitude lists) may also be useful for increasing perceived daily rewards.
The authors asked participants to rate their reward experiences based on the most pleasurable experience they had each day; this may have missed other important sources of reward, and on some days that may have been the only rewarding experience.
Though the sample did include a range of people with different amounts of time in recovery, the study did not explicitly focus on the initial recovery period. The experience of reward may shift rapidly in the first several months of recovery from opioid use disorder, and future research may explore similar research questions in a sample of people who are still new to recovery to determine whether these variables are particularly important for this initial risky period.
BOTTOM LINE
Though recovery from opioid use disorder is often thought to be accompanied at least initially by low levels of reward experience, in this study of individuals mostly taking methadone for 1+ years, many experienced different patterns of reward experience that varied day to day. In some cases, people experience minimal reward, whereas on other days those same people experience high levels of reward through planned activities. Planning highly rewarding activities may be associated with reduced opioid craving and less likelihood of opioid use, as well as high positive mood and quality of life. Importantly, doing well over an extended period may position someone better to plan fun activities. This suggests that while daily activities are important, activities that support longer-term recovery (e.g., making new recovery-supportive friends) may also be important and these may make rewarding activity planning easier on a more frequent basis. Interventions that emphasize increasing rewarding experiences through planning and goal setting, like cognitive and behavioral therapy strategies, may be able to help.
For individuals and families seeking recovery: If you are in recovery from opioid use disorder, you may experience fluctuations in your daily experience of reward, including both lower and higher pleasure days. Planning highly rewarding activities may lead to reduced opioid craving and less likelihood of opioid use as these activities offer compelling and pleasurable alternatives that can provide some level of reward. Interventions may be able to increase reward experience through planning and goal setting.
For treatment professionals and treatment systems: Planning highly rewarding activities may lead to reduced opioid craving and less likelihood of opioid use, as well as higher positive mood and quality of life. Some interventions, such as behavioral activation, explicitly attempt to plan rewarding, non-drug activities. Interventions like this may be useful to strategies to deploy to help improve recovery rates among people with opioid use disorder.
For scientists: These findings are an important step towards understanding the heterogeneity in experience of reward day to day. However, reward experience may also differ moment to moment, and in the degree to which they are perceived as rewarding over time – for example, the very same activity (e.g., bowling, mini-golf, hiking, etc.) may be quite dull early in recovery, but over time, become more pleasurable. Ecological momentary assessment studies may be able to further parse out different experiences in this regard even within the same day . Multiple episodes of these short assessment bursts may be needed to examine how reward sensitivity described above may shift over time. Further, research may benefit from comprehensive appraisal of definitions and measurement of pleasure, reward, meaning, purpose, and other elements commonly associated with reward and reinforcement. These are likely important elements, though the proper measurement may help us to more adequately understand interactions among facets of reward. Further, studies exploring these processes in initial recovery may help us understand them during the most critical time when anhedonia is likely at its highest level.
For policy makers: These findings suggest that access to and experience of high levels of reward is protective against return to opioid use and may improve quality of life among people in recovery from opioid use disorder. Policies that help facilitate this access and provide access to pleasurable rewards (e.g., nature, green spaces, bike/walking paths, free concerts in the park) may improve recovery rates. Further, funding for research that better explicates the relationship between non-pleasure and recovery would likely improve existing interventions and lead to novel approaches that can enhance recovery.
Opioids – including both prescription opioids like oxycodone and illicit opioids like heroin – increase feelings of pleasure in the short-term due to their activation of opioid pleasure receptors in the brain in addition to their analgesic, pain relief effects. These naturally occurring opioid receptors are also important for the general experience of reward and are activated by everyday pleasures such as eating ice cream or laughing at a funny joke. With repeated use of opioids, the brain reduces the number of neurotransmitters at opioid receptor sites (i.e., down-regulation) thereby reducing the experience of pleasure when these same previously pleasurable activities (e.g., eating ice cream) are performed (a process known as neuroadaptation). For some, this persists, and can last for quite a while, when people make a recovery attempt which can impact the experience of more normal levels of reward from everyday pleasures. As a result, many people in recovery from opioid use disorder report an impaired ability to experience pleasure. This difficulty may even persist among those receiving opioid agonist therapies, such as buprenorphine (e.g., Suboxone) or methadone, which also stimulate opioid receptors but tend to do so in a more consistent, stable, and controlled fashion than the peaks and valleys that are experienced by patterns of illicit opioid use.
Research has shown that fun, substance-free rewarding activities can compete to some degree with the rewards from substances, and if made more available and accessible it might be useful in aiding recovery by stimulating those down-regulated receptors.
Importantly, feelings of pleasure, as well as access to reward, may fluctuate throughout the day, and different patterns of reward experience may predict recovery outcomes and inform clinical interventions. While many studies have investigated the protective effects of rewarding substance-free activities over extended periods of time, their benefits of course are likely to manifest in the short term – for example, within the same day. This study examined whether different patterns of daily non-drug reward was associated with recovery outcomes, including opioid use, opioid craving, mood, and quality of life.
HOW WAS THIS STUDY CONDUCTED?
This study used a naturalistic design to assess non-drug activities, substance use, and other recovery outcomes each day for 3 weeks in 153 adults who were receiving opioid agonist treatment – primarily methadone – for opioid use disorder.
After completing a baseline survey, patients completed a brief survey every morning for 21 days. During the baseline survey, the patients reported on how long they have been in recovery and their overall lack of feelings of pleasure, often called, “anhedonia”. In each daily diary survey, participants reported on their experience with non-drug reward from the previous day. Participants were first asked how many things they did the day before that brought them pleasure or enjoyment. From this, for only the most rewarding activity, participants provided information on 7 facets of the rewarding experience on a 1 to 5 scale: (1) the extent to which they looked forward to it (anticipatory reward); (2) how enjoyable it was right when it occurred (consummatory reward); (3) the extent to which they found it meaningful/purposeful (meaning/purpose); (4) the extent to which they found the activity immersive and engaging (engagement); (5) the extent to which they did the activity for the purpose of feeling good (hedonic); (6) whether the activity was planned (planned); and (7) how enjoyable it was overall (overall rating). The primary recovery outcomes were daily mood, opioid craving, opioid use, and quality of life.
First, the authors used a statistical approach to identify patterns of day-level reward experience. Each of the seven reward indicators described above were used to identify these patterns. Second, analyses examined whether the proportions of days they experienced an opioid craving and of days they used opioids were associated with each day-level reward pattern, controlling for baseline anhedonia and the amount of time the person has been in recovery. Such statistical adjustments help to isolate the effect of interest – i.e., whether non-drug reward is independently related to opioid craving and use. Third, the authors explored whether these daily non-drug reward patterns were associated with same-day mood and quality of life.
The sample was, on average, 41 years old, primarily white (84%; 15% Black, 2% Native American, 1% Hispanic) and contained more females (57%) than males (43%). Participants were taking either methadone (85%) or buprenorphine (15%), and 65% had been in recovery for at least 1 year.
WHAT DID THIS STUDY FIND?
Many days included highly rewarding, planned activities
The authors identified 4 patterns of reward that occurred across people. The most common pattern included high ratings on every reward indicator and accounted for 35% of days across all participants (“Highly Rewarding-Planned” Pattern). The next most common had slightly lower mean ratings across all indicators and accounted for 31% of days (Moderately Rewarding Pattern). The Minimally Rewarding-Unplanned profile accounted for 22% of the days and was defined by low average ratings across indicators. Finally, 12% of the days were characterized by a Highly Rewarding-Unplanned profile with moderate to high ratings across all reward indicators and low scores on the “planned” indicator.
The planned highly rewarding daily pattern was associated with less opioid craving and use
Higher baseline pleasure scores were associated with a greater likelihood of experiencing a highly rewarding planned day relative to a moderately rewarding one – each additional point on the scale was associated with 4% increased odds of having a planned, highly rewarding day – or minimally rewarding day, which was associated with 5% increased odds. Also, opioid craving was associated with reward patterns, such that people who reported more craving had 60% lower likelihood of experiencing the highly rewarding planned pattern relative to the moderately reward pattern. Also, participants who reported more opioid use had an 80% lower likelihood of experiencing the highly rewarding planned pattern relative to the moderately rewarding one. Somewhat surprisingly, given the easier bar to surpass than moderately rewarding days, planned highly rewarding days were no more likely than minimally rewarding, unplanned days for people with fewer opioid use days.
Days characterized by high reward were associated with higher positive mood, lower negative mood, and greater quality of life
Days characterized by planned, high reward were associated with greater positive mood and quality of life, and lower negative mood, relative to days characterized by moderate reward or unplanned minimal reward. While the effects on negative mood were relatively modest, the effects on positive mood were almost 1 point (on a 1 to 5 scale) and the effects on quality of life were 21 points (on an 8 to 40 scale). Days characterized by planned, high reward were associated with greater positive mood and quality of life relative to days characterized by moderate reward or unplanned minimal reward; unplanned high reward days were associated with lower positive mood relative to days characterized planned high reward.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results suggest that people recovering from opioid use disorder and taking an agonist medication, such as methadone or buprenorphine, experience variability across days in the experience of reward. Almost half of the days were consistent with patterns of high reward, either planned or unplanned. On the other hand, in the same group of people, almost 1/4 of days were consistent with an unplanned and minimally rewarding pattern of reward . Although early recovery is often thought to be marked by a considerable lack of pleasure, these results suggest that people in recovery from opioid use disorder have the capacity to experience highly pleasurable non-drug reward, albeit these experiences may be inconsistent. Also, some have suggested that people taking agonists like methadone or buprenorphine may experience pleasure in recovery in a more muted fashion, because of the medication. Although this study cannot speak to this, as there was not a recovering opioid use disorder group who were not taking agonist medication, the results nonetheless do suggest that even if such muting or compression of pleasure may be occurring to some degree, these individuals nevertheless experienced attainable high pleasure variation and this was correlated with lower craving and less illicit opioid use. Finally, while 65% of these individuals had 1+ year in recovery, indicating greater potential for non-drug rewarding activities, surprisingly , whether someone had 1+ year or less than 1 year in recovery did not predict whether someone experienced a rewarding day. Overall, people considering recovery from opioids may benefit from knowing that they will likely be able to experience pleasures in alternative ways if they take a step toward abstinence.
One important caveat is that the activities were measured on the same day as opioid and other recovery outcomes. Thus, it is possible that positive experiences early in the day (e.g., restful sleep, taking one’s medication as prescribed, etc.) led to opportunities for fun, rewarding activities later. Also important is that there appeared to be an extra boost from planned rewarding activities, compared to those which were not planned, suggesting someone is already doing well, then plans a fun activity. For example, people who make new, recovery supportive friends – a longer-term process – may be better positioned to plan fun activities . Also of note is that the study used only the most rewarding activity each day, rather than combining all the activities to determine the degree to which somebody engaged in pleasurable activities – this might overestimate the relationship between fun, planned activities and reduced opioid use and craving.
Nevertheless, these findings are important because recovery from opioid use disorder can be difficult, and many people make multiple recovery attempts before being able to sustain recovery over the long-term, in part, because of lack of alternative reward accessibility and engagement with such alternatives. Early recovery is a period of high risk for return to use and overdose, which increases the urgency to identify mechanisms to improve success rates.
The results showed that days with high reward were associated with lower craving and opioid use and associated with higher quality of life and positive mood. Although, as noted above, the direction of effect here cannot be determined from this study design, the finding that daily non-drug reward may be an important buffer against return to use during recovery from opioid use disorder makes sense and is in keeping with people’s reported experiences. Some interventions, such as cognitive behavioral therapies or behavioral activation, also teach skills such as planning and goal setting to help people identify highly rewarding activities and to plan such activities. Therapies that help people reflect on their day’s positive experiences (e.g., gratitude lists) may also be useful for increasing perceived daily rewards.
The authors asked participants to rate their reward experiences based on the most pleasurable experience they had each day; this may have missed other important sources of reward, and on some days that may have been the only rewarding experience.
Though the sample did include a range of people with different amounts of time in recovery, the study did not explicitly focus on the initial recovery period. The experience of reward may shift rapidly in the first several months of recovery from opioid use disorder, and future research may explore similar research questions in a sample of people who are still new to recovery to determine whether these variables are particularly important for this initial risky period.
BOTTOM LINE
Though recovery from opioid use disorder is often thought to be accompanied at least initially by low levels of reward experience, in this study of individuals mostly taking methadone for 1+ years, many experienced different patterns of reward experience that varied day to day. In some cases, people experience minimal reward, whereas on other days those same people experience high levels of reward through planned activities. Planning highly rewarding activities may be associated with reduced opioid craving and less likelihood of opioid use, as well as high positive mood and quality of life. Importantly, doing well over an extended period may position someone better to plan fun activities. This suggests that while daily activities are important, activities that support longer-term recovery (e.g., making new recovery-supportive friends) may also be important and these may make rewarding activity planning easier on a more frequent basis. Interventions that emphasize increasing rewarding experiences through planning and goal setting, like cognitive and behavioral therapy strategies, may be able to help.
For individuals and families seeking recovery: If you are in recovery from opioid use disorder, you may experience fluctuations in your daily experience of reward, including both lower and higher pleasure days. Planning highly rewarding activities may lead to reduced opioid craving and less likelihood of opioid use as these activities offer compelling and pleasurable alternatives that can provide some level of reward. Interventions may be able to increase reward experience through planning and goal setting.
For treatment professionals and treatment systems: Planning highly rewarding activities may lead to reduced opioid craving and less likelihood of opioid use, as well as higher positive mood and quality of life. Some interventions, such as behavioral activation, explicitly attempt to plan rewarding, non-drug activities. Interventions like this may be useful to strategies to deploy to help improve recovery rates among people with opioid use disorder.
For scientists: These findings are an important step towards understanding the heterogeneity in experience of reward day to day. However, reward experience may also differ moment to moment, and in the degree to which they are perceived as rewarding over time – for example, the very same activity (e.g., bowling, mini-golf, hiking, etc.) may be quite dull early in recovery, but over time, become more pleasurable. Ecological momentary assessment studies may be able to further parse out different experiences in this regard even within the same day . Multiple episodes of these short assessment bursts may be needed to examine how reward sensitivity described above may shift over time. Further, research may benefit from comprehensive appraisal of definitions and measurement of pleasure, reward, meaning, purpose, and other elements commonly associated with reward and reinforcement. These are likely important elements, though the proper measurement may help us to more adequately understand interactions among facets of reward. Further, studies exploring these processes in initial recovery may help us understand them during the most critical time when anhedonia is likely at its highest level.
For policy makers: These findings suggest that access to and experience of high levels of reward is protective against return to opioid use and may improve quality of life among people in recovery from opioid use disorder. Policies that help facilitate this access and provide access to pleasurable rewards (e.g., nature, green spaces, bike/walking paths, free concerts in the park) may improve recovery rates. Further, funding for research that better explicates the relationship between non-pleasure and recovery would likely improve existing interventions and lead to novel approaches that can enhance recovery.
Opioids – including both prescription opioids like oxycodone and illicit opioids like heroin – increase feelings of pleasure in the short-term due to their activation of opioid pleasure receptors in the brain in addition to their analgesic, pain relief effects. These naturally occurring opioid receptors are also important for the general experience of reward and are activated by everyday pleasures such as eating ice cream or laughing at a funny joke. With repeated use of opioids, the brain reduces the number of neurotransmitters at opioid receptor sites (i.e., down-regulation) thereby reducing the experience of pleasure when these same previously pleasurable activities (e.g., eating ice cream) are performed (a process known as neuroadaptation). For some, this persists, and can last for quite a while, when people make a recovery attempt which can impact the experience of more normal levels of reward from everyday pleasures. As a result, many people in recovery from opioid use disorder report an impaired ability to experience pleasure. This difficulty may even persist among those receiving opioid agonist therapies, such as buprenorphine (e.g., Suboxone) or methadone, which also stimulate opioid receptors but tend to do so in a more consistent, stable, and controlled fashion than the peaks and valleys that are experienced by patterns of illicit opioid use.
Research has shown that fun, substance-free rewarding activities can compete to some degree with the rewards from substances, and if made more available and accessible it might be useful in aiding recovery by stimulating those down-regulated receptors.
Importantly, feelings of pleasure, as well as access to reward, may fluctuate throughout the day, and different patterns of reward experience may predict recovery outcomes and inform clinical interventions. While many studies have investigated the protective effects of rewarding substance-free activities over extended periods of time, their benefits of course are likely to manifest in the short term – for example, within the same day. This study examined whether different patterns of daily non-drug reward was associated with recovery outcomes, including opioid use, opioid craving, mood, and quality of life.
HOW WAS THIS STUDY CONDUCTED?
This study used a naturalistic design to assess non-drug activities, substance use, and other recovery outcomes each day for 3 weeks in 153 adults who were receiving opioid agonist treatment – primarily methadone – for opioid use disorder.
After completing a baseline survey, patients completed a brief survey every morning for 21 days. During the baseline survey, the patients reported on how long they have been in recovery and their overall lack of feelings of pleasure, often called, “anhedonia”. In each daily diary survey, participants reported on their experience with non-drug reward from the previous day. Participants were first asked how many things they did the day before that brought them pleasure or enjoyment. From this, for only the most rewarding activity, participants provided information on 7 facets of the rewarding experience on a 1 to 5 scale: (1) the extent to which they looked forward to it (anticipatory reward); (2) how enjoyable it was right when it occurred (consummatory reward); (3) the extent to which they found it meaningful/purposeful (meaning/purpose); (4) the extent to which they found the activity immersive and engaging (engagement); (5) the extent to which they did the activity for the purpose of feeling good (hedonic); (6) whether the activity was planned (planned); and (7) how enjoyable it was overall (overall rating). The primary recovery outcomes were daily mood, opioid craving, opioid use, and quality of life.
First, the authors used a statistical approach to identify patterns of day-level reward experience. Each of the seven reward indicators described above were used to identify these patterns. Second, analyses examined whether the proportions of days they experienced an opioid craving and of days they used opioids were associated with each day-level reward pattern, controlling for baseline anhedonia and the amount of time the person has been in recovery. Such statistical adjustments help to isolate the effect of interest – i.e., whether non-drug reward is independently related to opioid craving and use. Third, the authors explored whether these daily non-drug reward patterns were associated with same-day mood and quality of life.
The sample was, on average, 41 years old, primarily white (84%; 15% Black, 2% Native American, 1% Hispanic) and contained more females (57%) than males (43%). Participants were taking either methadone (85%) or buprenorphine (15%), and 65% had been in recovery for at least 1 year.
WHAT DID THIS STUDY FIND?
Many days included highly rewarding, planned activities
The authors identified 4 patterns of reward that occurred across people. The most common pattern included high ratings on every reward indicator and accounted for 35% of days across all participants (“Highly Rewarding-Planned” Pattern). The next most common had slightly lower mean ratings across all indicators and accounted for 31% of days (Moderately Rewarding Pattern). The Minimally Rewarding-Unplanned profile accounted for 22% of the days and was defined by low average ratings across indicators. Finally, 12% of the days were characterized by a Highly Rewarding-Unplanned profile with moderate to high ratings across all reward indicators and low scores on the “planned” indicator.
The planned highly rewarding daily pattern was associated with less opioid craving and use
Higher baseline pleasure scores were associated with a greater likelihood of experiencing a highly rewarding planned day relative to a moderately rewarding one – each additional point on the scale was associated with 4% increased odds of having a planned, highly rewarding day – or minimally rewarding day, which was associated with 5% increased odds. Also, opioid craving was associated with reward patterns, such that people who reported more craving had 60% lower likelihood of experiencing the highly rewarding planned pattern relative to the moderately reward pattern. Also, participants who reported more opioid use had an 80% lower likelihood of experiencing the highly rewarding planned pattern relative to the moderately rewarding one. Somewhat surprisingly, given the easier bar to surpass than moderately rewarding days, planned highly rewarding days were no more likely than minimally rewarding, unplanned days for people with fewer opioid use days.
Days characterized by high reward were associated with higher positive mood, lower negative mood, and greater quality of life
Days characterized by planned, high reward were associated with greater positive mood and quality of life, and lower negative mood, relative to days characterized by moderate reward or unplanned minimal reward. While the effects on negative mood were relatively modest, the effects on positive mood were almost 1 point (on a 1 to 5 scale) and the effects on quality of life were 21 points (on an 8 to 40 scale). Days characterized by planned, high reward were associated with greater positive mood and quality of life relative to days characterized by moderate reward or unplanned minimal reward; unplanned high reward days were associated with lower positive mood relative to days characterized planned high reward.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results suggest that people recovering from opioid use disorder and taking an agonist medication, such as methadone or buprenorphine, experience variability across days in the experience of reward. Almost half of the days were consistent with patterns of high reward, either planned or unplanned. On the other hand, in the same group of people, almost 1/4 of days were consistent with an unplanned and minimally rewarding pattern of reward . Although early recovery is often thought to be marked by a considerable lack of pleasure, these results suggest that people in recovery from opioid use disorder have the capacity to experience highly pleasurable non-drug reward, albeit these experiences may be inconsistent. Also, some have suggested that people taking agonists like methadone or buprenorphine may experience pleasure in recovery in a more muted fashion, because of the medication. Although this study cannot speak to this, as there was not a recovering opioid use disorder group who were not taking agonist medication, the results nonetheless do suggest that even if such muting or compression of pleasure may be occurring to some degree, these individuals nevertheless experienced attainable high pleasure variation and this was correlated with lower craving and less illicit opioid use. Finally, while 65% of these individuals had 1+ year in recovery, indicating greater potential for non-drug rewarding activities, surprisingly , whether someone had 1+ year or less than 1 year in recovery did not predict whether someone experienced a rewarding day. Overall, people considering recovery from opioids may benefit from knowing that they will likely be able to experience pleasures in alternative ways if they take a step toward abstinence.
One important caveat is that the activities were measured on the same day as opioid and other recovery outcomes. Thus, it is possible that positive experiences early in the day (e.g., restful sleep, taking one’s medication as prescribed, etc.) led to opportunities for fun, rewarding activities later. Also important is that there appeared to be an extra boost from planned rewarding activities, compared to those which were not planned, suggesting someone is already doing well, then plans a fun activity. For example, people who make new, recovery supportive friends – a longer-term process – may be better positioned to plan fun activities . Also of note is that the study used only the most rewarding activity each day, rather than combining all the activities to determine the degree to which somebody engaged in pleasurable activities – this might overestimate the relationship between fun, planned activities and reduced opioid use and craving.
Nevertheless, these findings are important because recovery from opioid use disorder can be difficult, and many people make multiple recovery attempts before being able to sustain recovery over the long-term, in part, because of lack of alternative reward accessibility and engagement with such alternatives. Early recovery is a period of high risk for return to use and overdose, which increases the urgency to identify mechanisms to improve success rates.
The results showed that days with high reward were associated with lower craving and opioid use and associated with higher quality of life and positive mood. Although, as noted above, the direction of effect here cannot be determined from this study design, the finding that daily non-drug reward may be an important buffer against return to use during recovery from opioid use disorder makes sense and is in keeping with people’s reported experiences. Some interventions, such as cognitive behavioral therapies or behavioral activation, also teach skills such as planning and goal setting to help people identify highly rewarding activities and to plan such activities. Therapies that help people reflect on their day’s positive experiences (e.g., gratitude lists) may also be useful for increasing perceived daily rewards.
The authors asked participants to rate their reward experiences based on the most pleasurable experience they had each day; this may have missed other important sources of reward, and on some days that may have been the only rewarding experience.
Though the sample did include a range of people with different amounts of time in recovery, the study did not explicitly focus on the initial recovery period. The experience of reward may shift rapidly in the first several months of recovery from opioid use disorder, and future research may explore similar research questions in a sample of people who are still new to recovery to determine whether these variables are particularly important for this initial risky period.
BOTTOM LINE
Though recovery from opioid use disorder is often thought to be accompanied at least initially by low levels of reward experience, in this study of individuals mostly taking methadone for 1+ years, many experienced different patterns of reward experience that varied day to day. In some cases, people experience minimal reward, whereas on other days those same people experience high levels of reward through planned activities. Planning highly rewarding activities may be associated with reduced opioid craving and less likelihood of opioid use, as well as high positive mood and quality of life. Importantly, doing well over an extended period may position someone better to plan fun activities. This suggests that while daily activities are important, activities that support longer-term recovery (e.g., making new recovery-supportive friends) may also be important and these may make rewarding activity planning easier on a more frequent basis. Interventions that emphasize increasing rewarding experiences through planning and goal setting, like cognitive and behavioral therapy strategies, may be able to help.
For individuals and families seeking recovery: If you are in recovery from opioid use disorder, you may experience fluctuations in your daily experience of reward, including both lower and higher pleasure days. Planning highly rewarding activities may lead to reduced opioid craving and less likelihood of opioid use as these activities offer compelling and pleasurable alternatives that can provide some level of reward. Interventions may be able to increase reward experience through planning and goal setting.
For treatment professionals and treatment systems: Planning highly rewarding activities may lead to reduced opioid craving and less likelihood of opioid use, as well as higher positive mood and quality of life. Some interventions, such as behavioral activation, explicitly attempt to plan rewarding, non-drug activities. Interventions like this may be useful to strategies to deploy to help improve recovery rates among people with opioid use disorder.
For scientists: These findings are an important step towards understanding the heterogeneity in experience of reward day to day. However, reward experience may also differ moment to moment, and in the degree to which they are perceived as rewarding over time – for example, the very same activity (e.g., bowling, mini-golf, hiking, etc.) may be quite dull early in recovery, but over time, become more pleasurable. Ecological momentary assessment studies may be able to further parse out different experiences in this regard even within the same day . Multiple episodes of these short assessment bursts may be needed to examine how reward sensitivity described above may shift over time. Further, research may benefit from comprehensive appraisal of definitions and measurement of pleasure, reward, meaning, purpose, and other elements commonly associated with reward and reinforcement. These are likely important elements, though the proper measurement may help us to more adequately understand interactions among facets of reward. Further, studies exploring these processes in initial recovery may help us understand them during the most critical time when anhedonia is likely at its highest level.
For policy makers: These findings suggest that access to and experience of high levels of reward is protective against return to opioid use and may improve quality of life among people in recovery from opioid use disorder. Policies that help facilitate this access and provide access to pleasurable rewards (e.g., nature, green spaces, bike/walking paths, free concerts in the park) may improve recovery rates. Further, funding for research that better explicates the relationship between non-pleasure and recovery would likely improve existing interventions and lead to novel approaches that can enhance recovery.