Stigma toward people with substance use disorders, including the perception that they are dangerous, may limit public support for treatment and recovery support services. In this study, researchers examined the association between the public’s different views on what recovery is or should be, and how this relates to stigmatizing attitudes they may hold towards people currently suffering from a variety of different types of substance use disorders. It also took a further step to try to discover whether perceived dangerousness helps explain these stigmatizing attitudes.
Understanding attitudes that account for stigma toward people with substance use disorder can help identify public health intervention targets. It is possible, for example, that how the public understands recovery from substance use disorder may influence the extent to which they stigmatize those with an active substance use disorder. One way this could occur is if people believe that recovery means stopping use completely, then they may hold harsher or more punitive judgements toward someone who continues to use the substance, even if it is in much reduced amounts and less often. Also, the degree of negative attitudes that people may have in this regard may vary across different legal (e.g., alcohol) and illegal (e.g., cocaine, heroin) substances. One potential reason why these attitudes may vary across these legal and illegal substances is that the general public may view illicit substances as more dangerous – perhaps supported by the implicit rationale, “They’re illegal because they’re more dangerous”.
To investigate these ideas more formally, researchers in this study examined stigmatizing attitudes held by the general public toward people with different types of substance use disorder (e.g., alcohol use disorder, opioid use disorder, cocaine use disorder) and investigated their association with different ways of defining “recovery”, with specific investigation of the relationship between defining recovery foremost as stopping drug use completely (i.e., “no use of substances”), compared to other definitions. They also examined whether how dangerous the public perceives people with different types of substance use disorders to be plays a role in those associations.
HOW WAS THIS STUDY CONDUCTED?
To investigate the themes above, data were drawn from the AmeriSpeak survey, a national survey in the US.
The AmeriSpeak survey has been operated by the NORC at the University of Chicago since 2015. Data for the current study was drawn in Fall 2021. This survey is designed to be representative of the US population and randomly selects US households from the sampling frame to be invited to participate. Recruitment was conducted by mail and phone, and surveys were completed either online or via the phone if the household did not have internet access.
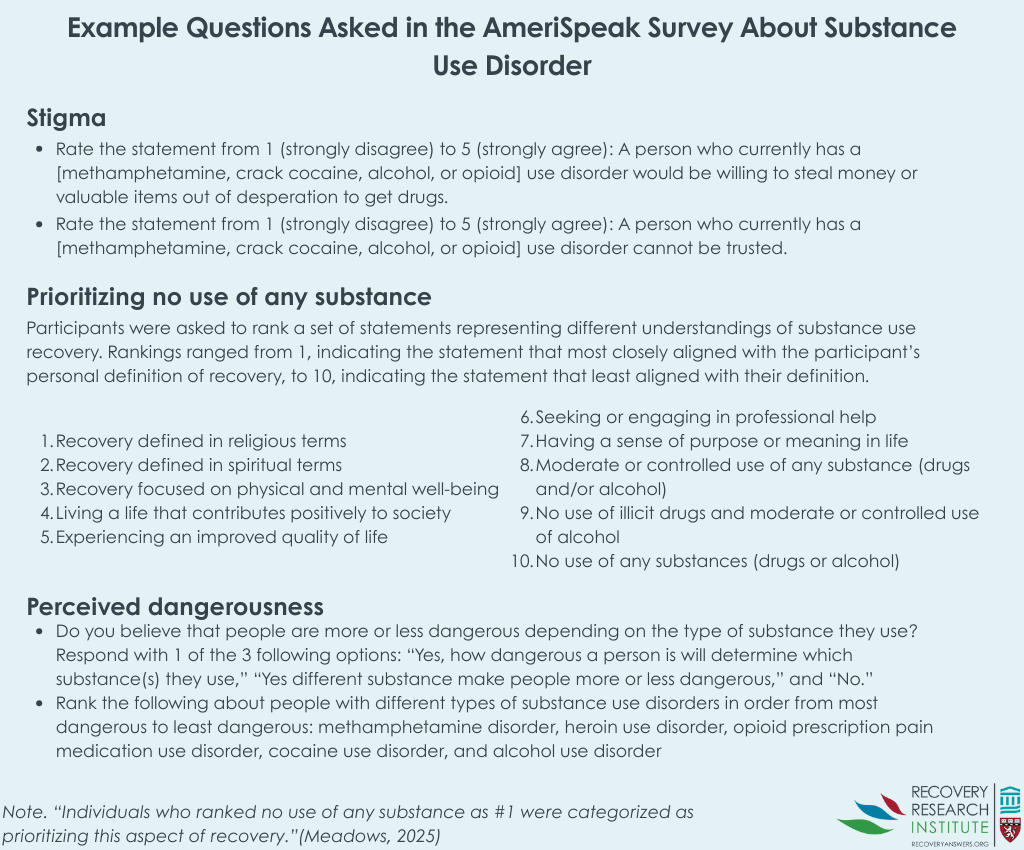
For the current study, a subset of participants who previously completed the AmeriSpeak survey was randomly selected and invited to participate in this survey about perceptions of drug use and recovery. Participants were compensated $25 USD for completing the survey. The variables of interest included defining recovery foremost as “no use of substances” vs any other definition, and the degree of stigmatizing attitudes toward people with different types of substance use disorders, some of which consisted of a legal drug (alcohol) and other illegal drugs (e.g., methamphetamine, heroin). Perceived dangerousness was a further variable examined to see if it helped explain (mediated) the relationship between the recovery definition variable and degree of stigma.
From the graphic above that explains how the study was organized, if participants ranked the recovery statement, “no use of any substances,” as a 1, or most closely corresponding to their definition of recovery, they prioritized “no use of any substances” (what the study refers to as “preference for abstinence”). If they ranked that statement as anything greater than 1, they were considered to prioritize another aspect of recovery (e.g., moderate/controlled use of any substance, enhanced quality of life, etc.). For stigma, the researchers created 1 continuous scale for each of the 4 substance use disorders, with higher scores on the scale reflecting greater stigma. For dangerousness, variables were created for each substance use disorder and were coded from 1-5, reflecting the ranking each participant gave (i.e., the most dangerously ranked substance use disorder was coded 1 and the least was coded 5). The research team reverse coded the variables so that higher scores reflected greater perceptions of dangerousness. Note that the substance use disorders were not rated based on their perceived dangerous overall, only relative to the other substance use disorders. This is important because, in theory, people could perceive each substance as extremely dangerous, but this would not be reflected in the measure.
For the analyses, the researchers computed descriptive statistics to analyze the public’s mean, or average, levels of stigma towards different substances. Then, analyses were conducted to examine whether prioritizing nonuse of any substance in their definition of recovery was associated with stigma toward different substances and whether perceived dangerousness of people with substance use disorders moderated (i.e., influenced the strength of) any association. While the dangerousness analyses tested whether the association between prioritizing no use of any substance and stigma was conditional on the level of perceived dangerousness, conceptually, the question of whether perceived dangerousness explains the association may be a more apt research question to examine in this scenario, and could, to a certain extent, be examined here too. Notably, analyses involving perceived dangerousness tested opioid prescription pain medication use disorder and heroin use disorder separately.
In total, 6,515 of the 17,075 individuals contacted completed the survey and were included in the analyses. Age across participants was approximately equally distributed, with 19% being between the ages 19-29, 26% between the ages 30-44, 24% between the ages 45-59, and 31% aged 60 years or older. Approximately 47% of participants identified as men, 53% identified as women, and less than 1% identified as transgender. The majority of participants identified as White (63%). Most held either a high school diploma (27%) and a vocational degree or some college (28%). Income was also roughly equally distributed across participants.
WHAT DID THIS STUDY FIND?
Public stigma was greatest towards methamphetamine use disorder; defining recovery foremost as no use of any substance was associated with greater stigma overall towards all substances
Public stigma was greatest towards methamphetamine disorder, with a mean of 3.75. This was closely followed by cocaine use disorder, with a mean of 3.70, which was then followed by opioid use disorder (mean = 3.30) and alcohol use disorder (mean = 3.14). The study did not test whether these stigma values were statistically different.
One in 3 individuals (35%) prioritized “no use of any substance” in their recovery definition; with the remainder – 2 in 3 – prioritizing another aspect in their recovery definition. For the 35% of participants that prioritized no use of any substance, they reported greater stigma towards cocaine, opioid, methamphetamine, and alcohol use disorders. This relationship was strongest for the illegal substances (cocaine, methamphetamine, and opioid use disorders [including both heroin and prescription opioid use]) but the stigma differences were small between those with and without this “no use” recovery definition priority.
The relationship between prioritizing no use of any substance and stigma could potentially be explained by perceived dangerousness, but only for certain substances
The relationships between prioritizing no use of any substances and public stigma towards substances did not depend on perceived dangerousness of people with substance use disorder.
That said, there were differences in the substance use disorder-related stigma that might be explained by perceived dangerousness. Overall, the perceived dangerousness associated with alcohol use disorder was unrelated to stigma. Cocaine use disorder dangerousness was related to stigma, but the variable measuring recovery as “no use of any substance” versus something else remained significant, suggesting other variables account for this relationship between the priority and stigma. Methamphetamine dangerousness was also related to stigma, and may account in part for the relationship between priority and stigma. Prescription opioid use disorder dangerousness was related to stigma and may account for the relationship between priority and stigma. Similarly, heroin use disorder dangerousness was related to stigma and may account for the relationship between priority and stigma. Importantly, however, these variables – defining recovery as “no use of any substances” or not and dangerousness – only accounted for only 1-2% of the variability in stigma, suggested many other variables explain why someone has more or less stigmatizing attitudes toward individuals with substance use disorder.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined how different beliefs about what recovery is or should be relate to different degrees of stigmatizing beliefs including perceived danger. Defining addiction recovery foremost as “no use of any substance” was associated with greater stigma than defining it in other ways, but this varied by type of substance. In general, the pattern of results suggested that if you think that addiction recovery is about stopping use completely and someone still continues to use to some degree, then stigma is higher, and it is higher for illicit drugs compared to a legal one like alcohol. Stigma was found to be greatest towards methamphetamine and cocaine use disorder, when compared to alcohol and opioid use disorder, which may be due to methamphetamine and cocaine being illicit. Lower stigma toward opioid use disorder may be related to the greater acceptability of opioid pain medication use, because it has a medical indication and is often medically prescribed. However, the average score for the stigma scale on all substances was above 3 (out of 5), reflecting that many participants trended towards agreeing with the stigma statements and suggesting a fairly high degree of stigma against all substances.
While results showed that defining recovery foremost as no use of any substance was related to more stigma toward individuals with substance use disorders, the magnitude of these relationships were small. In studies with very large samples like this one, even very small effects can be statistically significant (i.e., reliable). Even when accounting for perceived dangerousness, the amount of public stigma explained by these variables was quite small, suggesting there are many factors contributing to public stigma toward individuals with substance use disorder. Importantly, as mentioned above the ranking style measurement both for defining recovery as no use of any substance and perceived dangerousness did not allow for more comprehensive ratings; e.g., no use of any substance and increased quality of life may both be equally important in one’s definition of recovery. This ultimately limits the degree to which these findings can be applied to real-world circumstances.
That said, it is possible that policies which promote a more nuanced, multi-pronged concept of recovery – e.g., that some in recovery may be cutting back rather than quitting, focused on personal growth, contributing positively to society, etc. – may help reduce public stigma against substance use disorders. Ultimately, initiatives that help reduce blame toward those with substance use disorder may help to improve public support for access to evidence-based treatment and recovery-support services.
These results also showed that increases in perceived dangerousness of people with all substance use disorders were associated with increases in public stigma, except for alcohol use disorder, which is likely due to alcohol being legal, more familiar to more people and more likely to be personally experienced at lower levels of exposure than those associated with typical alcohol-specific and related harms, and the general social acceptability of its use.
The study was conducted in the United States. Results may not generalize to other countries, such as countries with stricter laws and less favorable views of substance use or vice versa.
The survey was conducted at one time point. This study design prevents the researchers from being able to conclude that the associations between preferences for abstinence-based recovery and greater stigma towards substances is casual.
Given effects that were small in magnitude (despite statistical significance, a function of the study’s larger sample size), it is unclear to how these results may actually translate into real-world relationships between prioritizing different elements of recovery and stigma.
BOTTOM LINE
Being more likely to define recovery foremost as no use of any substances was generally associated with greater stigma towards individuals with current active substance use disorder who are still using the substance, though the magnitude of differences were small. That said, such small effects, at scale may make a major difference. It is possible that policies which promote recovery as taking many forms including reduced use, and involving several dimensions of personal growth and well-being could reduce stigma, but more research is needed given the specific design elements of the current study.
For individuals and families seeking recovery: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, but more research is needed.
For treatment professionals and treatment systems: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, which would ultimately increase the number of people receiving care, but more research is needed.
For scientists: Studies like these which examine the contributors and nature of public stigma toward individuals with substance use disorder are important to informing policies and campaigns that can help to reduce this stigma and ultimately increase access to treatment and recovery support services. Future work that employs stronger empirical measures of the constructs at hand, while also controlling for potential confounders, would help build on this well-intentioned, but limited study.
For policy makers: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, which would ultimately increase the number of people receiving care, but more research is needed.
Understanding attitudes that account for stigma toward people with substance use disorder can help identify public health intervention targets. It is possible, for example, that how the public understands recovery from substance use disorder may influence the extent to which they stigmatize those with an active substance use disorder. One way this could occur is if people believe that recovery means stopping use completely, then they may hold harsher or more punitive judgements toward someone who continues to use the substance, even if it is in much reduced amounts and less often. Also, the degree of negative attitudes that people may have in this regard may vary across different legal (e.g., alcohol) and illegal (e.g., cocaine, heroin) substances. One potential reason why these attitudes may vary across these legal and illegal substances is that the general public may view illicit substances as more dangerous – perhaps supported by the implicit rationale, “They’re illegal because they’re more dangerous”.
To investigate these ideas more formally, researchers in this study examined stigmatizing attitudes held by the general public toward people with different types of substance use disorder (e.g., alcohol use disorder, opioid use disorder, cocaine use disorder) and investigated their association with different ways of defining “recovery”, with specific investigation of the relationship between defining recovery foremost as stopping drug use completely (i.e., “no use of substances”), compared to other definitions. They also examined whether how dangerous the public perceives people with different types of substance use disorders to be plays a role in those associations.
HOW WAS THIS STUDY CONDUCTED?
To investigate the themes above, data were drawn from the AmeriSpeak survey, a national survey in the US.
The AmeriSpeak survey has been operated by the NORC at the University of Chicago since 2015. Data for the current study was drawn in Fall 2021. This survey is designed to be representative of the US population and randomly selects US households from the sampling frame to be invited to participate. Recruitment was conducted by mail and phone, and surveys were completed either online or via the phone if the household did not have internet access.
For the current study, a subset of participants who previously completed the AmeriSpeak survey was randomly selected and invited to participate in this survey about perceptions of drug use and recovery. Participants were compensated $25 USD for completing the survey. The variables of interest included defining recovery foremost as “no use of substances” vs any other definition, and the degree of stigmatizing attitudes toward people with different types of substance use disorders, some of which consisted of a legal drug (alcohol) and other illegal drugs (e.g., methamphetamine, heroin). Perceived dangerousness was a further variable examined to see if it helped explain (mediated) the relationship between the recovery definition variable and degree of stigma.
From the graphic above that explains how the study was organized, if participants ranked the recovery statement, “no use of any substances,” as a 1, or most closely corresponding to their definition of recovery, they prioritized “no use of any substances” (what the study refers to as “preference for abstinence”). If they ranked that statement as anything greater than 1, they were considered to prioritize another aspect of recovery (e.g., moderate/controlled use of any substance, enhanced quality of life, etc.). For stigma, the researchers created 1 continuous scale for each of the 4 substance use disorders, with higher scores on the scale reflecting greater stigma. For dangerousness, variables were created for each substance use disorder and were coded from 1-5, reflecting the ranking each participant gave (i.e., the most dangerously ranked substance use disorder was coded 1 and the least was coded 5). The research team reverse coded the variables so that higher scores reflected greater perceptions of dangerousness. Note that the substance use disorders were not rated based on their perceived dangerous overall, only relative to the other substance use disorders. This is important because, in theory, people could perceive each substance as extremely dangerous, but this would not be reflected in the measure.
For the analyses, the researchers computed descriptive statistics to analyze the public’s mean, or average, levels of stigma towards different substances. Then, analyses were conducted to examine whether prioritizing nonuse of any substance in their definition of recovery was associated with stigma toward different substances and whether perceived dangerousness of people with substance use disorders moderated (i.e., influenced the strength of) any association. While the dangerousness analyses tested whether the association between prioritizing no use of any substance and stigma was conditional on the level of perceived dangerousness, conceptually, the question of whether perceived dangerousness explains the association may be a more apt research question to examine in this scenario, and could, to a certain extent, be examined here too. Notably, analyses involving perceived dangerousness tested opioid prescription pain medication use disorder and heroin use disorder separately.
In total, 6,515 of the 17,075 individuals contacted completed the survey and were included in the analyses. Age across participants was approximately equally distributed, with 19% being between the ages 19-29, 26% between the ages 30-44, 24% between the ages 45-59, and 31% aged 60 years or older. Approximately 47% of participants identified as men, 53% identified as women, and less than 1% identified as transgender. The majority of participants identified as White (63%). Most held either a high school diploma (27%) and a vocational degree or some college (28%). Income was also roughly equally distributed across participants.
WHAT DID THIS STUDY FIND?
Public stigma was greatest towards methamphetamine use disorder; defining recovery foremost as no use of any substance was associated with greater stigma overall towards all substances
Public stigma was greatest towards methamphetamine disorder, with a mean of 3.75. This was closely followed by cocaine use disorder, with a mean of 3.70, which was then followed by opioid use disorder (mean = 3.30) and alcohol use disorder (mean = 3.14). The study did not test whether these stigma values were statistically different.
One in 3 individuals (35%) prioritized “no use of any substance” in their recovery definition; with the remainder – 2 in 3 – prioritizing another aspect in their recovery definition. For the 35% of participants that prioritized no use of any substance, they reported greater stigma towards cocaine, opioid, methamphetamine, and alcohol use disorders. This relationship was strongest for the illegal substances (cocaine, methamphetamine, and opioid use disorders [including both heroin and prescription opioid use]) but the stigma differences were small between those with and without this “no use” recovery definition priority.
The relationship between prioritizing no use of any substance and stigma could potentially be explained by perceived dangerousness, but only for certain substances
The relationships between prioritizing no use of any substances and public stigma towards substances did not depend on perceived dangerousness of people with substance use disorder.
That said, there were differences in the substance use disorder-related stigma that might be explained by perceived dangerousness. Overall, the perceived dangerousness associated with alcohol use disorder was unrelated to stigma. Cocaine use disorder dangerousness was related to stigma, but the variable measuring recovery as “no use of any substance” versus something else remained significant, suggesting other variables account for this relationship between the priority and stigma. Methamphetamine dangerousness was also related to stigma, and may account in part for the relationship between priority and stigma. Prescription opioid use disorder dangerousness was related to stigma and may account for the relationship between priority and stigma. Similarly, heroin use disorder dangerousness was related to stigma and may account for the relationship between priority and stigma. Importantly, however, these variables – defining recovery as “no use of any substances” or not and dangerousness – only accounted for only 1-2% of the variability in stigma, suggested many other variables explain why someone has more or less stigmatizing attitudes toward individuals with substance use disorder.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined how different beliefs about what recovery is or should be relate to different degrees of stigmatizing beliefs including perceived danger. Defining addiction recovery foremost as “no use of any substance” was associated with greater stigma than defining it in other ways, but this varied by type of substance. In general, the pattern of results suggested that if you think that addiction recovery is about stopping use completely and someone still continues to use to some degree, then stigma is higher, and it is higher for illicit drugs compared to a legal one like alcohol. Stigma was found to be greatest towards methamphetamine and cocaine use disorder, when compared to alcohol and opioid use disorder, which may be due to methamphetamine and cocaine being illicit. Lower stigma toward opioid use disorder may be related to the greater acceptability of opioid pain medication use, because it has a medical indication and is often medically prescribed. However, the average score for the stigma scale on all substances was above 3 (out of 5), reflecting that many participants trended towards agreeing with the stigma statements and suggesting a fairly high degree of stigma against all substances.
While results showed that defining recovery foremost as no use of any substance was related to more stigma toward individuals with substance use disorders, the magnitude of these relationships were small. In studies with very large samples like this one, even very small effects can be statistically significant (i.e., reliable). Even when accounting for perceived dangerousness, the amount of public stigma explained by these variables was quite small, suggesting there are many factors contributing to public stigma toward individuals with substance use disorder. Importantly, as mentioned above the ranking style measurement both for defining recovery as no use of any substance and perceived dangerousness did not allow for more comprehensive ratings; e.g., no use of any substance and increased quality of life may both be equally important in one’s definition of recovery. This ultimately limits the degree to which these findings can be applied to real-world circumstances.
That said, it is possible that policies which promote a more nuanced, multi-pronged concept of recovery – e.g., that some in recovery may be cutting back rather than quitting, focused on personal growth, contributing positively to society, etc. – may help reduce public stigma against substance use disorders. Ultimately, initiatives that help reduce blame toward those with substance use disorder may help to improve public support for access to evidence-based treatment and recovery-support services.
These results also showed that increases in perceived dangerousness of people with all substance use disorders were associated with increases in public stigma, except for alcohol use disorder, which is likely due to alcohol being legal, more familiar to more people and more likely to be personally experienced at lower levels of exposure than those associated with typical alcohol-specific and related harms, and the general social acceptability of its use.
The study was conducted in the United States. Results may not generalize to other countries, such as countries with stricter laws and less favorable views of substance use or vice versa.
The survey was conducted at one time point. This study design prevents the researchers from being able to conclude that the associations between preferences for abstinence-based recovery and greater stigma towards substances is casual.
Given effects that were small in magnitude (despite statistical significance, a function of the study’s larger sample size), it is unclear to how these results may actually translate into real-world relationships between prioritizing different elements of recovery and stigma.
BOTTOM LINE
Being more likely to define recovery foremost as no use of any substances was generally associated with greater stigma towards individuals with current active substance use disorder who are still using the substance, though the magnitude of differences were small. That said, such small effects, at scale may make a major difference. It is possible that policies which promote recovery as taking many forms including reduced use, and involving several dimensions of personal growth and well-being could reduce stigma, but more research is needed given the specific design elements of the current study.
For individuals and families seeking recovery: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, but more research is needed.
For treatment professionals and treatment systems: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, which would ultimately increase the number of people receiving care, but more research is needed.
For scientists: Studies like these which examine the contributors and nature of public stigma toward individuals with substance use disorder are important to informing policies and campaigns that can help to reduce this stigma and ultimately increase access to treatment and recovery support services. Future work that employs stronger empirical measures of the constructs at hand, while also controlling for potential confounders, would help build on this well-intentioned, but limited study.
For policy makers: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, which would ultimately increase the number of people receiving care, but more research is needed.
Understanding attitudes that account for stigma toward people with substance use disorder can help identify public health intervention targets. It is possible, for example, that how the public understands recovery from substance use disorder may influence the extent to which they stigmatize those with an active substance use disorder. One way this could occur is if people believe that recovery means stopping use completely, then they may hold harsher or more punitive judgements toward someone who continues to use the substance, even if it is in much reduced amounts and less often. Also, the degree of negative attitudes that people may have in this regard may vary across different legal (e.g., alcohol) and illegal (e.g., cocaine, heroin) substances. One potential reason why these attitudes may vary across these legal and illegal substances is that the general public may view illicit substances as more dangerous – perhaps supported by the implicit rationale, “They’re illegal because they’re more dangerous”.
To investigate these ideas more formally, researchers in this study examined stigmatizing attitudes held by the general public toward people with different types of substance use disorder (e.g., alcohol use disorder, opioid use disorder, cocaine use disorder) and investigated their association with different ways of defining “recovery”, with specific investigation of the relationship between defining recovery foremost as stopping drug use completely (i.e., “no use of substances”), compared to other definitions. They also examined whether how dangerous the public perceives people with different types of substance use disorders to be plays a role in those associations.
HOW WAS THIS STUDY CONDUCTED?
To investigate the themes above, data were drawn from the AmeriSpeak survey, a national survey in the US.
The AmeriSpeak survey has been operated by the NORC at the University of Chicago since 2015. Data for the current study was drawn in Fall 2021. This survey is designed to be representative of the US population and randomly selects US households from the sampling frame to be invited to participate. Recruitment was conducted by mail and phone, and surveys were completed either online or via the phone if the household did not have internet access.
For the current study, a subset of participants who previously completed the AmeriSpeak survey was randomly selected and invited to participate in this survey about perceptions of drug use and recovery. Participants were compensated $25 USD for completing the survey. The variables of interest included defining recovery foremost as “no use of substances” vs any other definition, and the degree of stigmatizing attitudes toward people with different types of substance use disorders, some of which consisted of a legal drug (alcohol) and other illegal drugs (e.g., methamphetamine, heroin). Perceived dangerousness was a further variable examined to see if it helped explain (mediated) the relationship between the recovery definition variable and degree of stigma.
From the graphic above that explains how the study was organized, if participants ranked the recovery statement, “no use of any substances,” as a 1, or most closely corresponding to their definition of recovery, they prioritized “no use of any substances” (what the study refers to as “preference for abstinence”). If they ranked that statement as anything greater than 1, they were considered to prioritize another aspect of recovery (e.g., moderate/controlled use of any substance, enhanced quality of life, etc.). For stigma, the researchers created 1 continuous scale for each of the 4 substance use disorders, with higher scores on the scale reflecting greater stigma. For dangerousness, variables were created for each substance use disorder and were coded from 1-5, reflecting the ranking each participant gave (i.e., the most dangerously ranked substance use disorder was coded 1 and the least was coded 5). The research team reverse coded the variables so that higher scores reflected greater perceptions of dangerousness. Note that the substance use disorders were not rated based on their perceived dangerous overall, only relative to the other substance use disorders. This is important because, in theory, people could perceive each substance as extremely dangerous, but this would not be reflected in the measure.
For the analyses, the researchers computed descriptive statistics to analyze the public’s mean, or average, levels of stigma towards different substances. Then, analyses were conducted to examine whether prioritizing nonuse of any substance in their definition of recovery was associated with stigma toward different substances and whether perceived dangerousness of people with substance use disorders moderated (i.e., influenced the strength of) any association. While the dangerousness analyses tested whether the association between prioritizing no use of any substance and stigma was conditional on the level of perceived dangerousness, conceptually, the question of whether perceived dangerousness explains the association may be a more apt research question to examine in this scenario, and could, to a certain extent, be examined here too. Notably, analyses involving perceived dangerousness tested opioid prescription pain medication use disorder and heroin use disorder separately.
In total, 6,515 of the 17,075 individuals contacted completed the survey and were included in the analyses. Age across participants was approximately equally distributed, with 19% being between the ages 19-29, 26% between the ages 30-44, 24% between the ages 45-59, and 31% aged 60 years or older. Approximately 47% of participants identified as men, 53% identified as women, and less than 1% identified as transgender. The majority of participants identified as White (63%). Most held either a high school diploma (27%) and a vocational degree or some college (28%). Income was also roughly equally distributed across participants.
WHAT DID THIS STUDY FIND?
Public stigma was greatest towards methamphetamine use disorder; defining recovery foremost as no use of any substance was associated with greater stigma overall towards all substances
Public stigma was greatest towards methamphetamine disorder, with a mean of 3.75. This was closely followed by cocaine use disorder, with a mean of 3.70, which was then followed by opioid use disorder (mean = 3.30) and alcohol use disorder (mean = 3.14). The study did not test whether these stigma values were statistically different.
One in 3 individuals (35%) prioritized “no use of any substance” in their recovery definition; with the remainder – 2 in 3 – prioritizing another aspect in their recovery definition. For the 35% of participants that prioritized no use of any substance, they reported greater stigma towards cocaine, opioid, methamphetamine, and alcohol use disorders. This relationship was strongest for the illegal substances (cocaine, methamphetamine, and opioid use disorders [including both heroin and prescription opioid use]) but the stigma differences were small between those with and without this “no use” recovery definition priority.
The relationship between prioritizing no use of any substance and stigma could potentially be explained by perceived dangerousness, but only for certain substances
The relationships between prioritizing no use of any substances and public stigma towards substances did not depend on perceived dangerousness of people with substance use disorder.
That said, there were differences in the substance use disorder-related stigma that might be explained by perceived dangerousness. Overall, the perceived dangerousness associated with alcohol use disorder was unrelated to stigma. Cocaine use disorder dangerousness was related to stigma, but the variable measuring recovery as “no use of any substance” versus something else remained significant, suggesting other variables account for this relationship between the priority and stigma. Methamphetamine dangerousness was also related to stigma, and may account in part for the relationship between priority and stigma. Prescription opioid use disorder dangerousness was related to stigma and may account for the relationship between priority and stigma. Similarly, heroin use disorder dangerousness was related to stigma and may account for the relationship between priority and stigma. Importantly, however, these variables – defining recovery as “no use of any substances” or not and dangerousness – only accounted for only 1-2% of the variability in stigma, suggested many other variables explain why someone has more or less stigmatizing attitudes toward individuals with substance use disorder.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined how different beliefs about what recovery is or should be relate to different degrees of stigmatizing beliefs including perceived danger. Defining addiction recovery foremost as “no use of any substance” was associated with greater stigma than defining it in other ways, but this varied by type of substance. In general, the pattern of results suggested that if you think that addiction recovery is about stopping use completely and someone still continues to use to some degree, then stigma is higher, and it is higher for illicit drugs compared to a legal one like alcohol. Stigma was found to be greatest towards methamphetamine and cocaine use disorder, when compared to alcohol and opioid use disorder, which may be due to methamphetamine and cocaine being illicit. Lower stigma toward opioid use disorder may be related to the greater acceptability of opioid pain medication use, because it has a medical indication and is often medically prescribed. However, the average score for the stigma scale on all substances was above 3 (out of 5), reflecting that many participants trended towards agreeing with the stigma statements and suggesting a fairly high degree of stigma against all substances.
While results showed that defining recovery foremost as no use of any substance was related to more stigma toward individuals with substance use disorders, the magnitude of these relationships were small. In studies with very large samples like this one, even very small effects can be statistically significant (i.e., reliable). Even when accounting for perceived dangerousness, the amount of public stigma explained by these variables was quite small, suggesting there are many factors contributing to public stigma toward individuals with substance use disorder. Importantly, as mentioned above the ranking style measurement both for defining recovery as no use of any substance and perceived dangerousness did not allow for more comprehensive ratings; e.g., no use of any substance and increased quality of life may both be equally important in one’s definition of recovery. This ultimately limits the degree to which these findings can be applied to real-world circumstances.
That said, it is possible that policies which promote a more nuanced, multi-pronged concept of recovery – e.g., that some in recovery may be cutting back rather than quitting, focused on personal growth, contributing positively to society, etc. – may help reduce public stigma against substance use disorders. Ultimately, initiatives that help reduce blame toward those with substance use disorder may help to improve public support for access to evidence-based treatment and recovery-support services.
These results also showed that increases in perceived dangerousness of people with all substance use disorders were associated with increases in public stigma, except for alcohol use disorder, which is likely due to alcohol being legal, more familiar to more people and more likely to be personally experienced at lower levels of exposure than those associated with typical alcohol-specific and related harms, and the general social acceptability of its use.
The study was conducted in the United States. Results may not generalize to other countries, such as countries with stricter laws and less favorable views of substance use or vice versa.
The survey was conducted at one time point. This study design prevents the researchers from being able to conclude that the associations between preferences for abstinence-based recovery and greater stigma towards substances is casual.
Given effects that were small in magnitude (despite statistical significance, a function of the study’s larger sample size), it is unclear to how these results may actually translate into real-world relationships between prioritizing different elements of recovery and stigma.
BOTTOM LINE
Being more likely to define recovery foremost as no use of any substances was generally associated with greater stigma towards individuals with current active substance use disorder who are still using the substance, though the magnitude of differences were small. That said, such small effects, at scale may make a major difference. It is possible that policies which promote recovery as taking many forms including reduced use, and involving several dimensions of personal growth and well-being could reduce stigma, but more research is needed given the specific design elements of the current study.
For individuals and families seeking recovery: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, but more research is needed.
For treatment professionals and treatment systems: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, which would ultimately increase the number of people receiving care, but more research is needed.
For scientists: Studies like these which examine the contributors and nature of public stigma toward individuals with substance use disorder are important to informing policies and campaigns that can help to reduce this stigma and ultimately increase access to treatment and recovery support services. Future work that employs stronger empirical measures of the constructs at hand, while also controlling for potential confounders, would help build on this well-intentioned, but limited study.
For policy makers: Describing recovery as taking many forms and involving several dimensions of personal growth and well-being could reduce public stigma, which would ultimately increase the number of people receiving care, but more research is needed.