Can a recovery support app add benefit to medications for opioid use disorder?
Methadone and buprenorphine improve opioid use disorder outcomes, but even when prescribed under ideal circumstances, over half continue to use illicit opioids. Researchers in this study tested whether the addition of a recovery support app called A-CHESS improved treatment outcomes.
This study was a clinical trial of 414 outpatient adults receiving any one of the three FDA approved medications for opioid use disorder (methadone, buprenorphine, or extended-release naltrexone), 206 of whom were randomized to medication treatment as usual and 208 to receive access to the A-CHESS recovery support app in addition to medication treatment as usual. Study participants also received treatment as usual from study recruitment sites that included recovery planning and counseling. Participants were free to engage with other substance use disorder treatments like psychotherapy and mutual-help programs outside of the study clinics. Participants were followed for 2 years, with assessments at study baseline, and then 4-, 8-, 12-, 16-, 20-, and 24-months post-baseline.
All participants were prescribed methadone, buprenorphine, or extended-release naltrexone as part of treatment as usual i.e., medication groups were self-selected. While the study did not provide information on medication pathway by group – researchers used a technique to randomize participants to the A-CHESS or comparison group considering which medication they were taking – so that any benefits of the A-CHESS condition could not be due to an imbalance on how medication type was randomized. At the beginning of treatment, 300 were receiving methadone, 90 were receiving buprenorphine, and 44 were receiving extended-release naltrexone and they were likely split evenly between the A-CHESS and medication as usual comparison group. These medications constituted initial pathways; they might have discontinued, switched, or remained on their initial medication. Participants who were randomized to also receive the A-CHESS app had access to the app using an Android operating system for 16 months. Participants who did not have an Android smartphone were provided one, pre-loaded with the app, and given data plans for the duration of the active, 16-month intervention period. While it is not stated directly whether those with Android smartphones were given access to the app on their own phone, this is a reasonable assumption. The A-CHESS app includes a range of functionalities that are designed to boost recovery motivation, enhance social support, and teach coping skills to help individuals better manage anxiety, stress, and craving.
Participants were 18 or older, had current moderate or severe opioid use disorder based on the DSM-5, but could not have acute medical problems or history of psychotic disorders. Individuals were recruited from outpatient programs in Massachusetts and Wisconsin.
The study’s primary outcomes were self-reported abstinence from opioids (yes or no) documented for the 30-days preceding each follow-up, confirmed by urine drug testing. If a participant reported abstinence but an available toxicology screen was positive (e.g., detecting the presence of one or more substances), their outcome was categorized as non-abstinent at the respective time point. Secondary outcomes included non-opioid substance use (i.e., alcohol, marijuana, sedatives, stimulants), medication treatment retention, engagement with other forms of treatment (e.g., outpatient treatment, residential treatment), mutual-help meeting attendance, and health service utilization. The researchers statistically controlled for characteristics including employment status, opioid use disorder treatment history, and baseline pain severity rating.
The sample of 414 individuals was on average 37 years old, predominantly White (94.0%) and 55% male. Participants endorsed, on average, 7 prior opioid use disorder treatment episodes.
WHAT DID THIS STUDY FIND?
Study non-completion was high, and use of A-CHESS diminished over time
Across all 414 study participants, 64% completed the final, 24-month follow-up session. Of the 208 study participants randomized to receive the A-CHESS app, 92% were still using the app after the first month, 74% after 6 months, and 59% after 12 months.
Participants randomized to receive the A-CHESS app utilized the app, on average, 32% of days during the first 12 months and then 18% of days in the second 12 months of the two-year study period.
Effects of the A-CHESS app on opioid or other drug use were limited
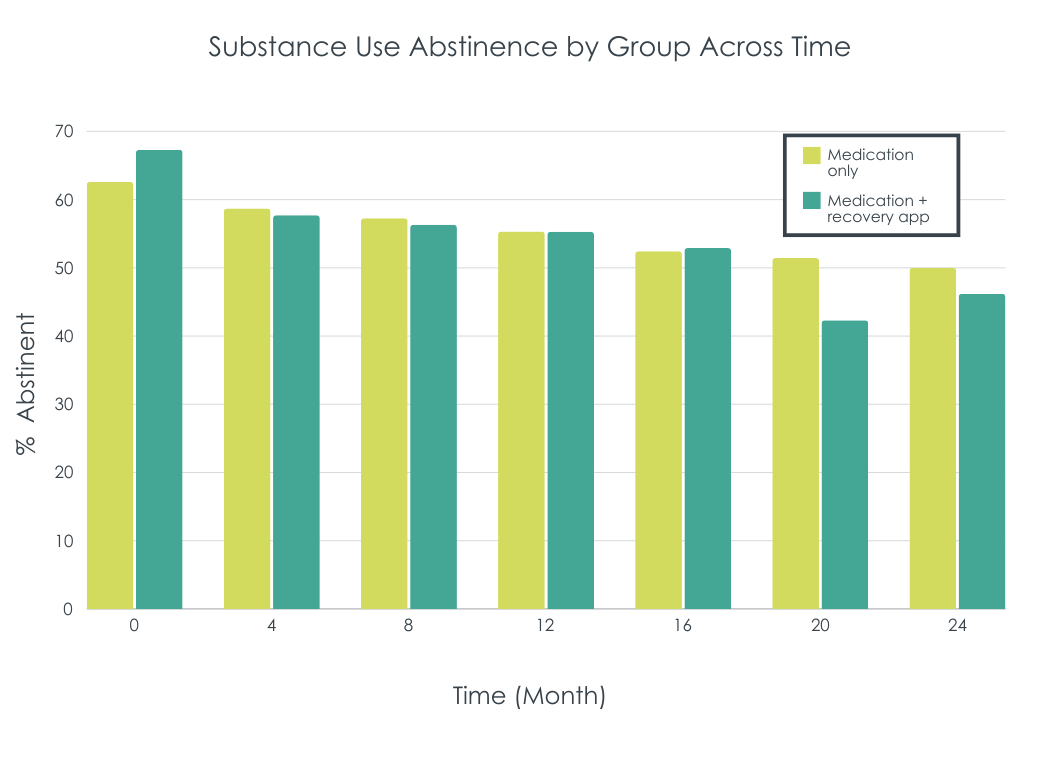
After accounting for individual characteristics, across the 24-month study period, the researchers did not find a marked difference in use of illicit opioids between study groups. To check if participant attrition was influencing this result, they also tested for between group differences with the assumption that participants lost to follow-up had used illicit opioids (i.e., intent-to-treat analysis). Groups were still not markedly different in terms of opioid use. Similarly, no between group differences were observed for other drug use (i.e., alcohol, cannabis, sedatives, stimulants).
Based on initial self-selected medication group, methadone patients had better response to receiving A-CHESS than buprenorphine patients. For the methadone sub-group, A-CHESS participants had improved abstinence over time – from approximately 75% to 95% abstinent –while those not receiving access had no such improvement – a “flat trajectory” over time. For the buprenorphine sub-group, access to A-CHESS did not improve their outcomes. While the study did not examine statistically if the benefits of A-CHESS access differed by medication sub-group, and furthermore participants self-selected into medication groups and could change their engagement with medications over time (e.g., discontinue medications or switch from one to another, etc.), this pattern may suggest A-CHESS access has utility for patients receiving methadone but not buprenorphine, although it is unclear why this may be the case.
A-CHESS access had some benefits on secondary outcomes
Participants who received the A-CHESS app, on average, attended more mutual-help meetings like Narcotics Anonymous over the study period. In addition, they were less likely to have emergency department and urgent care medical visits, though it can’t be known from the researchers’ data whether this was a result of less need for medical care (i.e., better physical health), or just less engagement with medical care. At the same time, groups were not different in medication treatment retention, and number of outpatient and therapy/counseling visits.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This kind of mobile health app (sometime also known as a digital therapeutic) like A-CHESS is attractive because it can include a lot of recovery support tools in an accessible, and low-cost package. While previous studies have suggested a benefit of the A-CHESS app on alcohol use outcomes and treatment retention in individuals with alcohol use disorder, findings from this study don’t immediately suggest a benefit of A-CHESS for individuals receiving medication for opioid use disorder, in terms of improving opioid or other substance use outcomes. The researchers, however, did see a benefit for the A-CHESS app for patients initially receiving methadone on substance use outcomes. Also, compared to those who did not get access to the app, the A-CHESS group, across the entire sample, increased their mutual-help meeting attendance and decreased their medical visits.
It is possible the app was conferring some specific benefit for some individuals, though it can’t be known from this study whether there’s a direct causal link between A-CHESS app usage and mutual-help meeting attendance and less medical visits. It is also notable that in spite of greater mutual-help meeting attendance, participants receiving A-CHESS did not have better substance use outcomes meaning this benefit, on average, didn’t translate into better substance use outcomes. Prior work has shown that in patients receiving the opioid use disorder medication buprenorphine/naloxone, mutual-help attendance is associated with greater likelihood of abstinence from opioids. The difference here may be related to the fact that most patients in this study were taking methadone with probably more severe opioid addiction histories which may require more intensive, or different types of, mutual-help or other treatment involvement to improve outcomes beyond that achieved through the medication alone. It may be also that in those with opioid use disorder, complete abstinence from alcohol and other drugs – which was the primary outcome measure used in this study – may be a higher threshold to reach compared to opioid abstinence specifically. While the study measured any mutual-help attendance as a secondary outcome, it did not account for other treatments and recovery supports that participants may have attended during the 2-year study.
On average, A-CHESS app usage was not particularly high, with participants using the app on 32% of days in study year 1, and 18% of days in status year 2, though there was a great deal of variability in frequency of individuals app usage. The A-CHESS app allows patients to identify a clinician (e.g., a therapist or counselor) to receive information from the app about individuals’ app engagement relapse risk. In this study, this information was sent to the study clinicians, though follow-up on this information was not part of the study design. Future studies will ideally explore how active use of this information affects both app engagement and recovery outcomes. In addition, participants in the A-CHESS condition were provided a new Android smartphone loaded with the app. The full benefits of A-CHESS, via greater adherence, may not be realized if A-CHESS is accessed outside patient’s typical day-to-day smartphone utility – that is, for people who already have a smartphone integrating A-CHESS engagement with their existing mobile and online communication (e.g., on the phone they use for phone calls and text messaging). Finally, although the research team did their best to account for participants dropping out from the study, 1/3 of the sample dropped out by 2-year follow-up. While there is no indication that drop-out differed by group and therefore impacted how the findings were interpreted, it may mean that these estimates are not truly representative of the population being studied – patients receiving medication for opioid use disorder.
Participants randomized to receive A-CHESS were provided with a smartphone and Internet service if needed and were thus incentivized to join the study and continue participation. This may limit the generalizability to real-world implementation involving individuals’ own cellphones and data plans.
The study sample included very little racial and ethnic diversity, which reduces the generalizability of findings to non-White and Hispanic populations.
Participants were free to engage with treatment as usual from the study clinic sites as well as additional treatments from outside clinics. Though this increased the translatability of the findings to the real-world, additional treatment quantity was not measured or controlled for in the study analyses and could have influenced the results in unknown ways.
It’s possible the largely negative findings in this study were a function of a robust response to medications for opioid use disorder that washed out a potentially mild but possibly meaningful benefit of the A-CHESS app. Future studies would ideally also include an additional study condition of A-CHESS app among opioid use disorder patients who do not wish to take any opioid use disorder medication to tease out these possible effects.
Participants receiving the A-CHESS app had fewer emergency department and urgent care medical visits, which could indicate better physical health and less need for medical treatment. However, it’s also possible patients had a similar number of medical issues but were not seeking care. Future studies like this will ideally monitor participants physical health to tease this out.
BOTTOM LINE
Digital therapeutics like the A-CHESS app are attractive because of their accessibility and affordability and have shown some benefit in alcohol use disorder treatment, but based on this initial trial, don’t appear to confer much average benefit for individuals receiving medication for opioid use disorder in terms of improving complete abstinence. There may however be a benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study. Future research should investigate which patients in particular may be a good match for this type of approach.
For individuals and families seeking recovery: Digital therapeutics like the A-CHESS app are attractive because of their accessibility and affordability and might be a helpful complement to first-line treatments for alcohol use disorder. However, based on this initial study of A-CHESS for individuals receiving medication for opioid use disorder, it does not appear to confer much benefit for these individuals in terms of improving rates of complete abstinence. There may some benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study.
For treatment professionals and treatment systems: Digital therapeutics like the A-CHESS app have shown capacity to support first-line alcohol use disorder treatment. Findings from this study, however, do not suggest a major benefit of this app on abstinence among individuals receiving medication for opioid use disorder. There may some benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study.
For scientists: The A-CHESS app, and others like it have produced promising results in alcohol use disorder treatment. This study, which largely produced null results, was the first testing the efficacy of the A-CHESS app for supporting individuals receiving medication for opioid use disorder. These findings should be replicated, preferably in a study that also includes an app-only condition to explore if a medium/large medication effect may be washing out a smaller but still meaningful app effect. Additionally, the observed association between app access and mutual-help meeting attendance and fewer medical visits should be more fully explored. Future research should investigate which patients in particular may be a good match for this type of approach.
For policy makers: Digital therapeutics like the A-CHESS app have potential to offer cost effective support of substance use disorder recovery. Funding for further research should be provided to investigate which patients in particular may be a good match for this type of approach to foster personalized medicine.
This study was a clinical trial of 414 outpatient adults receiving any one of the three FDA approved medications for opioid use disorder (methadone, buprenorphine, or extended-release naltrexone), 206 of whom were randomized to medication treatment as usual and 208 to receive access to the A-CHESS recovery support app in addition to medication treatment as usual. Study participants also received treatment as usual from study recruitment sites that included recovery planning and counseling. Participants were free to engage with other substance use disorder treatments like psychotherapy and mutual-help programs outside of the study clinics. Participants were followed for 2 years, with assessments at study baseline, and then 4-, 8-, 12-, 16-, 20-, and 24-months post-baseline.
All participants were prescribed methadone, buprenorphine, or extended-release naltrexone as part of treatment as usual i.e., medication groups were self-selected. While the study did not provide information on medication pathway by group – researchers used a technique to randomize participants to the A-CHESS or comparison group considering which medication they were taking – so that any benefits of the A-CHESS condition could not be due to an imbalance on how medication type was randomized. At the beginning of treatment, 300 were receiving methadone, 90 were receiving buprenorphine, and 44 were receiving extended-release naltrexone and they were likely split evenly between the A-CHESS and medication as usual comparison group. These medications constituted initial pathways; they might have discontinued, switched, or remained on their initial medication. Participants who were randomized to also receive the A-CHESS app had access to the app using an Android operating system for 16 months. Participants who did not have an Android smartphone were provided one, pre-loaded with the app, and given data plans for the duration of the active, 16-month intervention period. While it is not stated directly whether those with Android smartphones were given access to the app on their own phone, this is a reasonable assumption. The A-CHESS app includes a range of functionalities that are designed to boost recovery motivation, enhance social support, and teach coping skills to help individuals better manage anxiety, stress, and craving.
Participants were 18 or older, had current moderate or severe opioid use disorder based on the DSM-5, but could not have acute medical problems or history of psychotic disorders. Individuals were recruited from outpatient programs in Massachusetts and Wisconsin.
The study’s primary outcomes were self-reported abstinence from opioids (yes or no) documented for the 30-days preceding each follow-up, confirmed by urine drug testing. If a participant reported abstinence but an available toxicology screen was positive (e.g., detecting the presence of one or more substances), their outcome was categorized as non-abstinent at the respective time point. Secondary outcomes included non-opioid substance use (i.e., alcohol, marijuana, sedatives, stimulants), medication treatment retention, engagement with other forms of treatment (e.g., outpatient treatment, residential treatment), mutual-help meeting attendance, and health service utilization. The researchers statistically controlled for characteristics including employment status, opioid use disorder treatment history, and baseline pain severity rating.
The sample of 414 individuals was on average 37 years old, predominantly White (94.0%) and 55% male. Participants endorsed, on average, 7 prior opioid use disorder treatment episodes.
WHAT DID THIS STUDY FIND?
Study non-completion was high, and use of A-CHESS diminished over time
Across all 414 study participants, 64% completed the final, 24-month follow-up session. Of the 208 study participants randomized to receive the A-CHESS app, 92% were still using the app after the first month, 74% after 6 months, and 59% after 12 months.
Participants randomized to receive the A-CHESS app utilized the app, on average, 32% of days during the first 12 months and then 18% of days in the second 12 months of the two-year study period.
Effects of the A-CHESS app on opioid or other drug use were limited
After accounting for individual characteristics, across the 24-month study period, the researchers did not find a marked difference in use of illicit opioids between study groups. To check if participant attrition was influencing this result, they also tested for between group differences with the assumption that participants lost to follow-up had used illicit opioids (i.e., intent-to-treat analysis). Groups were still not markedly different in terms of opioid use. Similarly, no between group differences were observed for other drug use (i.e., alcohol, cannabis, sedatives, stimulants).
Based on initial self-selected medication group, methadone patients had better response to receiving A-CHESS than buprenorphine patients. For the methadone sub-group, A-CHESS participants had improved abstinence over time – from approximately 75% to 95% abstinent –while those not receiving access had no such improvement – a “flat trajectory” over time. For the buprenorphine sub-group, access to A-CHESS did not improve their outcomes. While the study did not examine statistically if the benefits of A-CHESS access differed by medication sub-group, and furthermore participants self-selected into medication groups and could change their engagement with medications over time (e.g., discontinue medications or switch from one to another, etc.), this pattern may suggest A-CHESS access has utility for patients receiving methadone but not buprenorphine, although it is unclear why this may be the case.
A-CHESS access had some benefits on secondary outcomes
Participants who received the A-CHESS app, on average, attended more mutual-help meetings like Narcotics Anonymous over the study period. In addition, they were less likely to have emergency department and urgent care medical visits, though it can’t be known from the researchers’ data whether this was a result of less need for medical care (i.e., better physical health), or just less engagement with medical care. At the same time, groups were not different in medication treatment retention, and number of outpatient and therapy/counseling visits.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This kind of mobile health app (sometime also known as a digital therapeutic) like A-CHESS is attractive because it can include a lot of recovery support tools in an accessible, and low-cost package. While previous studies have suggested a benefit of the A-CHESS app on alcohol use outcomes and treatment retention in individuals with alcohol use disorder, findings from this study don’t immediately suggest a benefit of A-CHESS for individuals receiving medication for opioid use disorder, in terms of improving opioid or other substance use outcomes. The researchers, however, did see a benefit for the A-CHESS app for patients initially receiving methadone on substance use outcomes. Also, compared to those who did not get access to the app, the A-CHESS group, across the entire sample, increased their mutual-help meeting attendance and decreased their medical visits.
It is possible the app was conferring some specific benefit for some individuals, though it can’t be known from this study whether there’s a direct causal link between A-CHESS app usage and mutual-help meeting attendance and less medical visits. It is also notable that in spite of greater mutual-help meeting attendance, participants receiving A-CHESS did not have better substance use outcomes meaning this benefit, on average, didn’t translate into better substance use outcomes. Prior work has shown that in patients receiving the opioid use disorder medication buprenorphine/naloxone, mutual-help attendance is associated with greater likelihood of abstinence from opioids. The difference here may be related to the fact that most patients in this study were taking methadone with probably more severe opioid addiction histories which may require more intensive, or different types of, mutual-help or other treatment involvement to improve outcomes beyond that achieved through the medication alone. It may be also that in those with opioid use disorder, complete abstinence from alcohol and other drugs – which was the primary outcome measure used in this study – may be a higher threshold to reach compared to opioid abstinence specifically. While the study measured any mutual-help attendance as a secondary outcome, it did not account for other treatments and recovery supports that participants may have attended during the 2-year study.
On average, A-CHESS app usage was not particularly high, with participants using the app on 32% of days in study year 1, and 18% of days in status year 2, though there was a great deal of variability in frequency of individuals app usage. The A-CHESS app allows patients to identify a clinician (e.g., a therapist or counselor) to receive information from the app about individuals’ app engagement relapse risk. In this study, this information was sent to the study clinicians, though follow-up on this information was not part of the study design. Future studies will ideally explore how active use of this information affects both app engagement and recovery outcomes. In addition, participants in the A-CHESS condition were provided a new Android smartphone loaded with the app. The full benefits of A-CHESS, via greater adherence, may not be realized if A-CHESS is accessed outside patient’s typical day-to-day smartphone utility – that is, for people who already have a smartphone integrating A-CHESS engagement with their existing mobile and online communication (e.g., on the phone they use for phone calls and text messaging). Finally, although the research team did their best to account for participants dropping out from the study, 1/3 of the sample dropped out by 2-year follow-up. While there is no indication that drop-out differed by group and therefore impacted how the findings were interpreted, it may mean that these estimates are not truly representative of the population being studied – patients receiving medication for opioid use disorder.
Participants randomized to receive A-CHESS were provided with a smartphone and Internet service if needed and were thus incentivized to join the study and continue participation. This may limit the generalizability to real-world implementation involving individuals’ own cellphones and data plans.
The study sample included very little racial and ethnic diversity, which reduces the generalizability of findings to non-White and Hispanic populations.
Participants were free to engage with treatment as usual from the study clinic sites as well as additional treatments from outside clinics. Though this increased the translatability of the findings to the real-world, additional treatment quantity was not measured or controlled for in the study analyses and could have influenced the results in unknown ways.
It’s possible the largely negative findings in this study were a function of a robust response to medications for opioid use disorder that washed out a potentially mild but possibly meaningful benefit of the A-CHESS app. Future studies would ideally also include an additional study condition of A-CHESS app among opioid use disorder patients who do not wish to take any opioid use disorder medication to tease out these possible effects.
Participants receiving the A-CHESS app had fewer emergency department and urgent care medical visits, which could indicate better physical health and less need for medical treatment. However, it’s also possible patients had a similar number of medical issues but were not seeking care. Future studies like this will ideally monitor participants physical health to tease this out.
BOTTOM LINE
Digital therapeutics like the A-CHESS app are attractive because of their accessibility and affordability and have shown some benefit in alcohol use disorder treatment, but based on this initial trial, don’t appear to confer much average benefit for individuals receiving medication for opioid use disorder in terms of improving complete abstinence. There may however be a benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study. Future research should investigate which patients in particular may be a good match for this type of approach.
For individuals and families seeking recovery: Digital therapeutics like the A-CHESS app are attractive because of their accessibility and affordability and might be a helpful complement to first-line treatments for alcohol use disorder. However, based on this initial study of A-CHESS for individuals receiving medication for opioid use disorder, it does not appear to confer much benefit for these individuals in terms of improving rates of complete abstinence. There may some benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study.
For treatment professionals and treatment systems: Digital therapeutics like the A-CHESS app have shown capacity to support first-line alcohol use disorder treatment. Findings from this study, however, do not suggest a major benefit of this app on abstinence among individuals receiving medication for opioid use disorder. There may some benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study.
For scientists: The A-CHESS app, and others like it have produced promising results in alcohol use disorder treatment. This study, which largely produced null results, was the first testing the efficacy of the A-CHESS app for supporting individuals receiving medication for opioid use disorder. These findings should be replicated, preferably in a study that also includes an app-only condition to explore if a medium/large medication effect may be washing out a smaller but still meaningful app effect. Additionally, the observed association between app access and mutual-help meeting attendance and fewer medical visits should be more fully explored. Future research should investigate which patients in particular may be a good match for this type of approach.
For policy makers: Digital therapeutics like the A-CHESS app have potential to offer cost effective support of substance use disorder recovery. Funding for further research should be provided to investigate which patients in particular may be a good match for this type of approach to foster personalized medicine.
This study was a clinical trial of 414 outpatient adults receiving any one of the three FDA approved medications for opioid use disorder (methadone, buprenorphine, or extended-release naltrexone), 206 of whom were randomized to medication treatment as usual and 208 to receive access to the A-CHESS recovery support app in addition to medication treatment as usual. Study participants also received treatment as usual from study recruitment sites that included recovery planning and counseling. Participants were free to engage with other substance use disorder treatments like psychotherapy and mutual-help programs outside of the study clinics. Participants were followed for 2 years, with assessments at study baseline, and then 4-, 8-, 12-, 16-, 20-, and 24-months post-baseline.
All participants were prescribed methadone, buprenorphine, or extended-release naltrexone as part of treatment as usual i.e., medication groups were self-selected. While the study did not provide information on medication pathway by group – researchers used a technique to randomize participants to the A-CHESS or comparison group considering which medication they were taking – so that any benefits of the A-CHESS condition could not be due to an imbalance on how medication type was randomized. At the beginning of treatment, 300 were receiving methadone, 90 were receiving buprenorphine, and 44 were receiving extended-release naltrexone and they were likely split evenly between the A-CHESS and medication as usual comparison group. These medications constituted initial pathways; they might have discontinued, switched, or remained on their initial medication. Participants who were randomized to also receive the A-CHESS app had access to the app using an Android operating system for 16 months. Participants who did not have an Android smartphone were provided one, pre-loaded with the app, and given data plans for the duration of the active, 16-month intervention period. While it is not stated directly whether those with Android smartphones were given access to the app on their own phone, this is a reasonable assumption. The A-CHESS app includes a range of functionalities that are designed to boost recovery motivation, enhance social support, and teach coping skills to help individuals better manage anxiety, stress, and craving.
Participants were 18 or older, had current moderate or severe opioid use disorder based on the DSM-5, but could not have acute medical problems or history of psychotic disorders. Individuals were recruited from outpatient programs in Massachusetts and Wisconsin.
The study’s primary outcomes were self-reported abstinence from opioids (yes or no) documented for the 30-days preceding each follow-up, confirmed by urine drug testing. If a participant reported abstinence but an available toxicology screen was positive (e.g., detecting the presence of one or more substances), their outcome was categorized as non-abstinent at the respective time point. Secondary outcomes included non-opioid substance use (i.e., alcohol, marijuana, sedatives, stimulants), medication treatment retention, engagement with other forms of treatment (e.g., outpatient treatment, residential treatment), mutual-help meeting attendance, and health service utilization. The researchers statistically controlled for characteristics including employment status, opioid use disorder treatment history, and baseline pain severity rating.
The sample of 414 individuals was on average 37 years old, predominantly White (94.0%) and 55% male. Participants endorsed, on average, 7 prior opioid use disorder treatment episodes.
WHAT DID THIS STUDY FIND?
Study non-completion was high, and use of A-CHESS diminished over time
Across all 414 study participants, 64% completed the final, 24-month follow-up session. Of the 208 study participants randomized to receive the A-CHESS app, 92% were still using the app after the first month, 74% after 6 months, and 59% after 12 months.
Participants randomized to receive the A-CHESS app utilized the app, on average, 32% of days during the first 12 months and then 18% of days in the second 12 months of the two-year study period.
Effects of the A-CHESS app on opioid or other drug use were limited
After accounting for individual characteristics, across the 24-month study period, the researchers did not find a marked difference in use of illicit opioids between study groups. To check if participant attrition was influencing this result, they also tested for between group differences with the assumption that participants lost to follow-up had used illicit opioids (i.e., intent-to-treat analysis). Groups were still not markedly different in terms of opioid use. Similarly, no between group differences were observed for other drug use (i.e., alcohol, cannabis, sedatives, stimulants).
Based on initial self-selected medication group, methadone patients had better response to receiving A-CHESS than buprenorphine patients. For the methadone sub-group, A-CHESS participants had improved abstinence over time – from approximately 75% to 95% abstinent –while those not receiving access had no such improvement – a “flat trajectory” over time. For the buprenorphine sub-group, access to A-CHESS did not improve their outcomes. While the study did not examine statistically if the benefits of A-CHESS access differed by medication sub-group, and furthermore participants self-selected into medication groups and could change their engagement with medications over time (e.g., discontinue medications or switch from one to another, etc.), this pattern may suggest A-CHESS access has utility for patients receiving methadone but not buprenorphine, although it is unclear why this may be the case.
A-CHESS access had some benefits on secondary outcomes
Participants who received the A-CHESS app, on average, attended more mutual-help meetings like Narcotics Anonymous over the study period. In addition, they were less likely to have emergency department and urgent care medical visits, though it can’t be known from the researchers’ data whether this was a result of less need for medical care (i.e., better physical health), or just less engagement with medical care. At the same time, groups were not different in medication treatment retention, and number of outpatient and therapy/counseling visits.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This kind of mobile health app (sometime also known as a digital therapeutic) like A-CHESS is attractive because it can include a lot of recovery support tools in an accessible, and low-cost package. While previous studies have suggested a benefit of the A-CHESS app on alcohol use outcomes and treatment retention in individuals with alcohol use disorder, findings from this study don’t immediately suggest a benefit of A-CHESS for individuals receiving medication for opioid use disorder, in terms of improving opioid or other substance use outcomes. The researchers, however, did see a benefit for the A-CHESS app for patients initially receiving methadone on substance use outcomes. Also, compared to those who did not get access to the app, the A-CHESS group, across the entire sample, increased their mutual-help meeting attendance and decreased their medical visits.
It is possible the app was conferring some specific benefit for some individuals, though it can’t be known from this study whether there’s a direct causal link between A-CHESS app usage and mutual-help meeting attendance and less medical visits. It is also notable that in spite of greater mutual-help meeting attendance, participants receiving A-CHESS did not have better substance use outcomes meaning this benefit, on average, didn’t translate into better substance use outcomes. Prior work has shown that in patients receiving the opioid use disorder medication buprenorphine/naloxone, mutual-help attendance is associated with greater likelihood of abstinence from opioids. The difference here may be related to the fact that most patients in this study were taking methadone with probably more severe opioid addiction histories which may require more intensive, or different types of, mutual-help or other treatment involvement to improve outcomes beyond that achieved through the medication alone. It may be also that in those with opioid use disorder, complete abstinence from alcohol and other drugs – which was the primary outcome measure used in this study – may be a higher threshold to reach compared to opioid abstinence specifically. While the study measured any mutual-help attendance as a secondary outcome, it did not account for other treatments and recovery supports that participants may have attended during the 2-year study.
On average, A-CHESS app usage was not particularly high, with participants using the app on 32% of days in study year 1, and 18% of days in status year 2, though there was a great deal of variability in frequency of individuals app usage. The A-CHESS app allows patients to identify a clinician (e.g., a therapist or counselor) to receive information from the app about individuals’ app engagement relapse risk. In this study, this information was sent to the study clinicians, though follow-up on this information was not part of the study design. Future studies will ideally explore how active use of this information affects both app engagement and recovery outcomes. In addition, participants in the A-CHESS condition were provided a new Android smartphone loaded with the app. The full benefits of A-CHESS, via greater adherence, may not be realized if A-CHESS is accessed outside patient’s typical day-to-day smartphone utility – that is, for people who already have a smartphone integrating A-CHESS engagement with their existing mobile and online communication (e.g., on the phone they use for phone calls and text messaging). Finally, although the research team did their best to account for participants dropping out from the study, 1/3 of the sample dropped out by 2-year follow-up. While there is no indication that drop-out differed by group and therefore impacted how the findings were interpreted, it may mean that these estimates are not truly representative of the population being studied – patients receiving medication for opioid use disorder.
Participants randomized to receive A-CHESS were provided with a smartphone and Internet service if needed and were thus incentivized to join the study and continue participation. This may limit the generalizability to real-world implementation involving individuals’ own cellphones and data plans.
The study sample included very little racial and ethnic diversity, which reduces the generalizability of findings to non-White and Hispanic populations.
Participants were free to engage with treatment as usual from the study clinic sites as well as additional treatments from outside clinics. Though this increased the translatability of the findings to the real-world, additional treatment quantity was not measured or controlled for in the study analyses and could have influenced the results in unknown ways.
It’s possible the largely negative findings in this study were a function of a robust response to medications for opioid use disorder that washed out a potentially mild but possibly meaningful benefit of the A-CHESS app. Future studies would ideally also include an additional study condition of A-CHESS app among opioid use disorder patients who do not wish to take any opioid use disorder medication to tease out these possible effects.
Participants receiving the A-CHESS app had fewer emergency department and urgent care medical visits, which could indicate better physical health and less need for medical treatment. However, it’s also possible patients had a similar number of medical issues but were not seeking care. Future studies like this will ideally monitor participants physical health to tease this out.
BOTTOM LINE
Digital therapeutics like the A-CHESS app are attractive because of their accessibility and affordability and have shown some benefit in alcohol use disorder treatment, but based on this initial trial, don’t appear to confer much average benefit for individuals receiving medication for opioid use disorder in terms of improving complete abstinence. There may however be a benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study. Future research should investigate which patients in particular may be a good match for this type of approach.
For individuals and families seeking recovery: Digital therapeutics like the A-CHESS app are attractive because of their accessibility and affordability and might be a helpful complement to first-line treatments for alcohol use disorder. However, based on this initial study of A-CHESS for individuals receiving medication for opioid use disorder, it does not appear to confer much benefit for these individuals in terms of improving rates of complete abstinence. There may some benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study.
For treatment professionals and treatment systems: Digital therapeutics like the A-CHESS app have shown capacity to support first-line alcohol use disorder treatment. Findings from this study, however, do not suggest a major benefit of this app on abstinence among individuals receiving medication for opioid use disorder. There may some benefit related to greater mutual-help meeting attendance and less medical care utilization, though this needs further study.
For scientists: The A-CHESS app, and others like it have produced promising results in alcohol use disorder treatment. This study, which largely produced null results, was the first testing the efficacy of the A-CHESS app for supporting individuals receiving medication for opioid use disorder. These findings should be replicated, preferably in a study that also includes an app-only condition to explore if a medium/large medication effect may be washing out a smaller but still meaningful app effect. Additionally, the observed association between app access and mutual-help meeting attendance and fewer medical visits should be more fully explored. Future research should investigate which patients in particular may be a good match for this type of approach.
For policy makers: Digital therapeutics like the A-CHESS app have potential to offer cost effective support of substance use disorder recovery. Funding for further research should be provided to investigate which patients in particular may be a good match for this type of approach to foster personalized medicine.