WHAT PROBLEM DOES THIS STUDY ADDRESS?
Methamphetamine use and methamphetamine-related overdose deaths have risen in the United States but there are still no FDA-approved medications, and few psychosocial interventions, that reliably treat methamphetamine use disorder. Contingency management, in which patients are rewarded with financial incentives to stay abstinent – verified by negative urine drug tests, is shown to be one of the most consistently helpful behavioral approaches for this condition, but it has faced implementation barriers because of concerns about cost, regulation, and public perception.
In early 2025, the federal government raised the annual cap on contingency management incentives to $750, but it is not clear whether programs at that incentive level offer value. This study used a modelling-based approach to explore whether the costs associated with delivering contingency management are likely to be justified given the potential benefits in improved health and overdose death prevention.
HOW WAS THIS STUDY CONDUCTED?
The researchers built a microsimulation model (informed by existing research studies) that followed a hypothetical cohort of 10,000 United States adults with methamphetamine use disorder over their lifetimes. The model compared no substance use disorder treatment with two outpatient contingency management approaches; a 12-week program with up to $375 in incentives, and a 24-week program with up to $750 in incentives. In both cases, contingency management was combined with counseling, though the type and nature of counseling is not described in the study. The model estimated changes in methamphetamine use, withdrawal symptoms, abstinence, depressive symptoms, psychotic symptoms, cardiovascular events, deaths, healthcare costs, and quality-adjusted life years (QALYs; the additional years of life adjusted for how healthy those years are) based on existing data tracking these factors. It also estimated healthcare costs from studies of standard healthcare expenditures, costs associated with methamphetamine use and methamphetamine use disorder, associated psychiatric and cardiovascular symptoms, and costs of the outpatient contingency management program (monetary rewards and counseling sessions). Note that the models did not account for criminal justice costs and several health outcomes, as many cost-effectiveness studies do often include.
The researchers tested 3 versions of the model; a main analysis, a pessimistic scenario, and an optimistic scenario. In the main analysis, people were assumed to follow the usual pattern after treatment ended, while the pessimistic scenario assumed everyone returned to methamphetamine use right away, and the optimistic scenario assumed the treatment benefits lasted longer after the contingency management program ended.
WHAT DID THIS STUDY FIND?
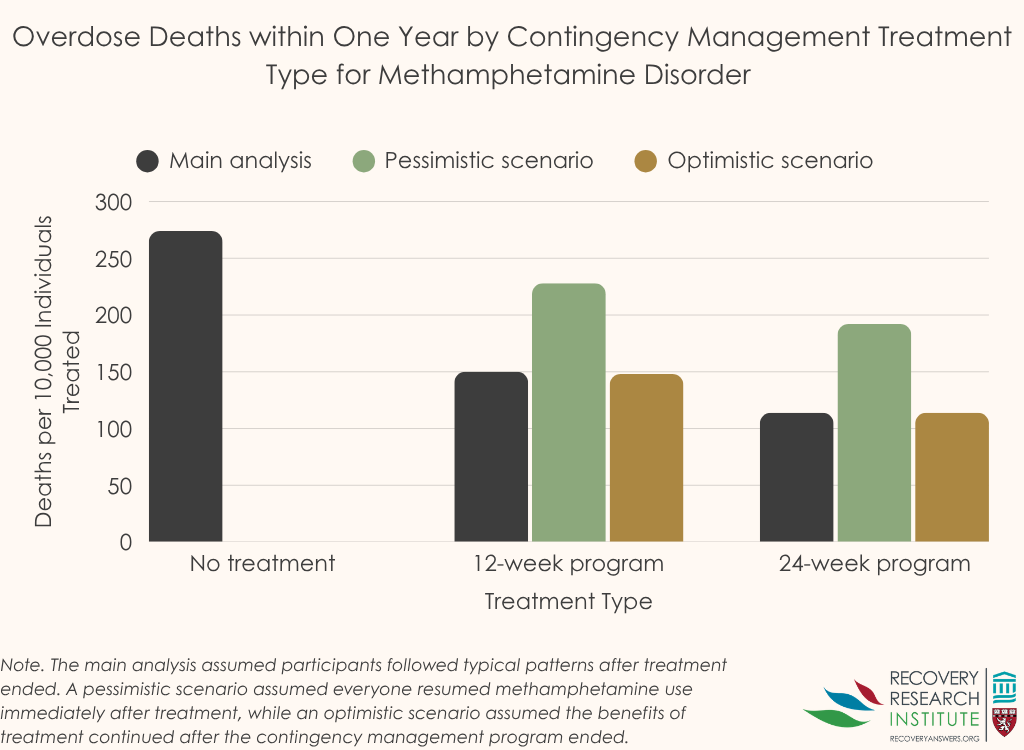
Both contingency management programs appeared to provide substantial health benefit
Compared with no treatment, both programs reduced deaths over the first year and increased lifetime quality-adjusted life years. In the researchers’ main analysis, the 12-week program prevented about 117 deaths per 10,000 people over one year, while the 24-week program prevented about 153 deaths (see graph below). Most of the difference came from fewer overdose deaths, suggesting that even a time-limited behavioral program could produce meaningful short-term survival gains.
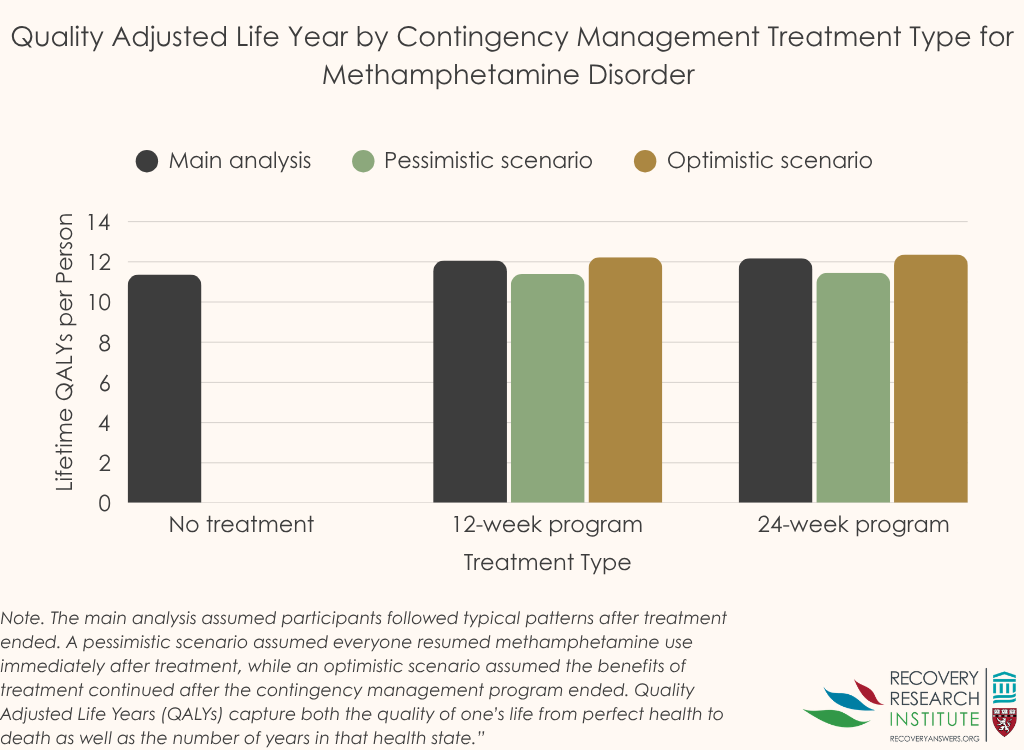
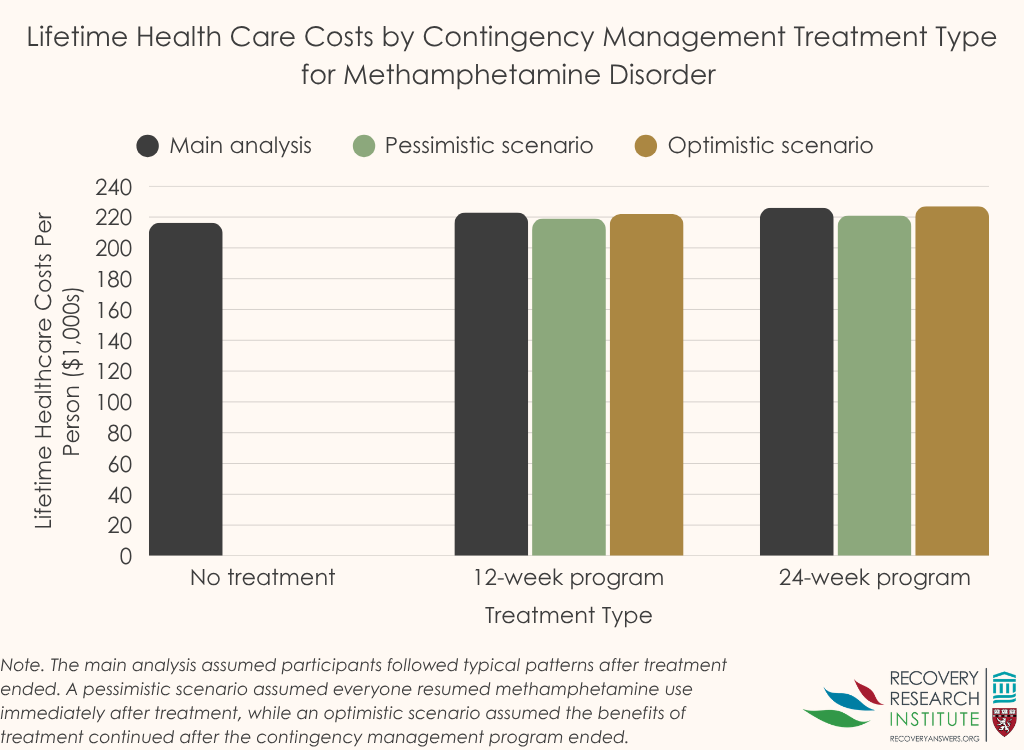
The added health benefit came at a relatively modest additional healthcare cost
Under the study’s main set of assumptions, the 12-week program added about 0.70 quality-adjusted life years per person and increased lifetime healthcare spending by about $6,850 per person relative to no contingency management.
The 24-week program added about 0.81 quality-adjusted life years per person and increased lifetime healthcare spending by about $10,000 per person relative to no contingency management. See graphs below for QALYs and cost estimates by condition. Overall, the cost-effectiveness estimates were well below common United States benchmarks used to judge whether an intervention offers good value for money.
The 24-week program generally produced greater benefit than the 12-week program
Across the main and more optimistic scenarios, the longer program was associated with fewer overdose deaths and more quality-adjusted life years gained than the shorter program. It cost more overall, but the added cost per additional unit of health benefit remained favorable. This pattern suggests that extending contingency management may be worthwhile when programs can sustain engagement.
Findings remained encouraging even under conservative assumptions, but the shorter program looked less favorable if all benefit disappeared immediately after treatment
When the model assumed that everyone returned to methamphetamine use right after the program ended, the 24-week program still appeared to offer acceptable value, while the 12-week program became much less attractive economically. This means conclusions about cost value depend partly on whether treatment effects last beyond the incentive period, something the model could not determine directly. Because the study was based on simulation rather than a head-to-head clinical trial, the findings are best understood as model-based estimates rather than definitive real-world evidence of what will happen in real-world settings.
The value of contingency management may be underestimated
The model did not include some consequences that could make contingency management look even better, such as reduced criminal legal system involvement, reduced child welfare costs, or reduced transmission of HIV and hepatitis C. It also did not capture every real-world difference in access, dropout, repeated treatment episodes, or patient severity. As a result, the estimates may be conservative, especially for systems interested in broader social costs and benefits beyond healthcare spending alone.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that contingency management for methamphetamine use disorder is likely to be a helpful and economically attractive treatment option, even at the newer federal incentive cap. The longer 24-week version appeared especially promising because it produced larger health gains and still met commonly used value thresholds. In other words, contingency management is worth doing because it is highly cost-effective; for example, the standard case of the 24-week contingency management cost $12,000 per additional quality life year gained, which is much lower than the typical benchmark of $50,000 per additional quality life year gained used by health economists. It compares favorably to many accepted medical interventions, including modern cancer treatments which cost $100,000 – $300,000 per quality life year gained, and to hypertension treatments which cost nearly $20,000 per quality life year gained. That said, the findings come from a model built from prior studies rather than direct observation of a national program, so real-world implementation, engagement, and durability of benefit will matter. Even so, the results support expanding access to contingency management while continuing to study which program designs work best for different populations and settings.
BOTTOM LINE
Contingency management for methamphetamine use disorder may save lives, improve health outcomes, and provide good value for healthcare spending, with a 24-week approach showing the strongest overall promise. These findings suggest that the current federal incentive limit is consistent with good economic value.
- For individuals and families seeking recovery: This study suggests that monetary reward-based treatment approaches may help people reduce methamphetamine use and improve health, especially when support continues for several months.
- For treatment professionals and treatment systems: Programs that use incentives for drug-free tests may offer good value for patients and health systems, especially if they can maintain participation over a longer period. These findings may help justify broader adoption of contingency management in outpatient care.
- For scientists: The study supports further real-world testing of contingency management duration, incentive structure, and post-treatment durability. Future work should also examine how dropout, re-entry, housing instability, and co-occurring conditions change outcomes and cost-effectiveness.
- For policy makers: The analysis suggests that the current federal incentive cap for contingency management represents good economic value and may still be conservative. Policies that support implementation, reimbursement, and workforce training could expand access to a potentially life-saving intervention.
CITATIONS
Qian, G. L., Chen, Y., Rawson, R. A., Humphreys, K., & Brandeau, M. L. (2026). Cost-effectiveness of contingency management for methamphetamine use disorder: A model-based analysis. Addiction. doi: 10.1111/add.70377.













