Reflecting on opportunities to change after having an infection from injecting drugs
Little is known about how major drug use consequences such as serious infections affect a patient’s substance use and willingness to engage with addiction services. This study characterized patients’ perspectives on substance use, harm reduction, and medication treatments for opioid use disorder after hospitalization for an injection-related infection.
Individuals who inject drugs are at risk of injection-related infections and the rate of serious, life-threatening infections from drug injection are on the rise. These infections typically require a hospital stay with antibiotic treatment. It is also now standard practice to provide medication treatments for opioid use disorder (e.g., buprenorphine) onsite for people who are hospitalized for opioid-related reasons, such as an injection-related infection. However, even in states with greater availability of medication treatment, only half of individuals who present to the hospital with serious injection-related infections actually receive medication treatment for opioid use disorder (we do not know whether this is because they offered it and refused it, or were not offered it). Given buprenorphine/naloxone (commonly prescribed under the brand name, “Suboxone”) is considered the gold standard in opioid use disorder treatment and can help prevent overdose, this finding highlights an important treatment gap.
Hospitals offer an ideal location to educate patients about harm-reduction behaviors, deliver services (e.g., medication treatment), and link individuals to outpatient treatment and recovery support services that can help reduce drug-related harms and deaths. Yet, little is known about how serious injection-related hospitalizations affect patient’s substance use and willingness to engage in such services.
To help fill this knowledge gap, this study aimed to characterize patients’ perspectives on substance use, harm reduction, and medication treatments for opioid use disorder after hospitalization for injection-related infection. Gaining a better understanding of how individuals who had a hospital stay for an injection-related infection think about treatment and recovery could inform optimal clinical approaches that might better engage them with a helpful medication like buprenorphine/naloxone or some other harm reduction or recovery support service.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of adults hospitalized for a serious injection-related infection between 2020 and 2023, in which 30 patients completed questionnaires and interviews about their substance use, opinions on harm reduction and opioid use disorder medication treatments. Individuals were recruited from Boston Medical Center, an urban hospital in Massachusetts with comprehensive addiction and infection disease resources.
Eligible participants were recruited from hospital records and the community. All participants had experienced a serious infection related to injection drug use at least 2 weeks, and no more than 3 years, prior to study enrollment (median duration from infection to interview = 330 days). Infections related to injection drug use considered in this study required hospitalization and included, for example, endocarditis and bloodstream infection. At the time of infection, all participants also had diagnosed opioid use disorder.
Participants completed questionnaires about their demographics, substance use, and infection histories. During the semi-structured qualitative interviews, participants answered questions about the timeframe just before, during, and after hospitalization for a serious injection-related infection. Interviews asked about patient perspectives on their hospitalization experience and potential ways to improve care. Qualitative interviews were analyzed for themes related to the impact of hospitalization on subsequent substance use, perspectives on harm reduction, and perspectives on medication treatments for opioid use disorder.
The majority of participants were White Non-Hispanic (70.0%), men (63%), with a high-school or equivalent education (43%) and an average age of 39 years old. Thirty percent of participants were receiving disability income and 60% were living in their own home, alone or with other people, at the time of study participation. Patients experienced an average of 3 infections over their lifetime and were asked about the following types of infections that occurred most recently: endocarditis (33%), bacteremia (17%), osteomyelitis (30%), epidural abscess (13%), and septic arthritis (7%). Most patients reported finishing their prescribed antibiotic regimens for their infections, as instructed by their doctors (80%).
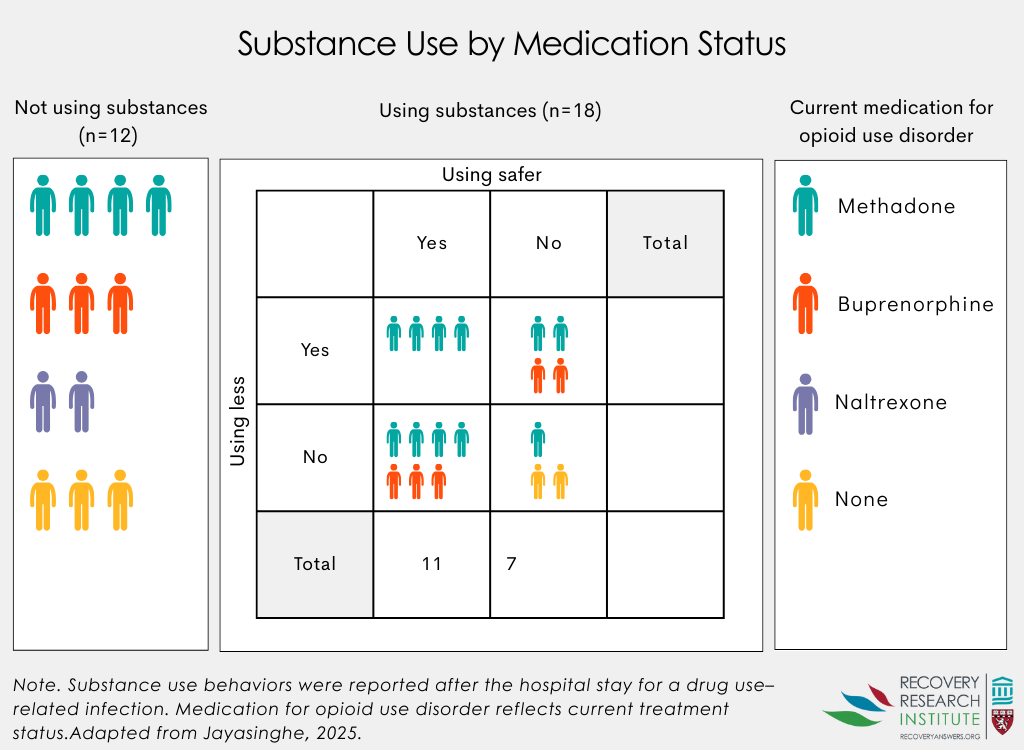
Opioids were reported as the preferred drug of choice for all but 1 participant (98%), who reported a stimulant preference. Fifty-seven percent of those who reported opioids as their preferred drug, also reported stimulant use. Nearly all patients had prior treatment experience with methadone (90%) and buprenorphine (87%), and 27% had been previously treated with extended-release injectable naltrexone, though not necessarily coinciding with when they were hospitalized. At the time of study participation, most patients were actively receiving treatment with methadone (50%), buprenorphine (27%), or extended-release naltrexone (7%); 16% of participants were not receiving any medication treatment.
WHAT DID THIS STUDY FIND?
Ongoing drug use after hospitalization was common, but many implemented harm-reduction techniques
After hospitalization for injection-related infection, 60% of patients continued to use drugs. Among the patients who continued to use drugs, 83% adopted harm reduction practices, including using less often or using in a safer way.
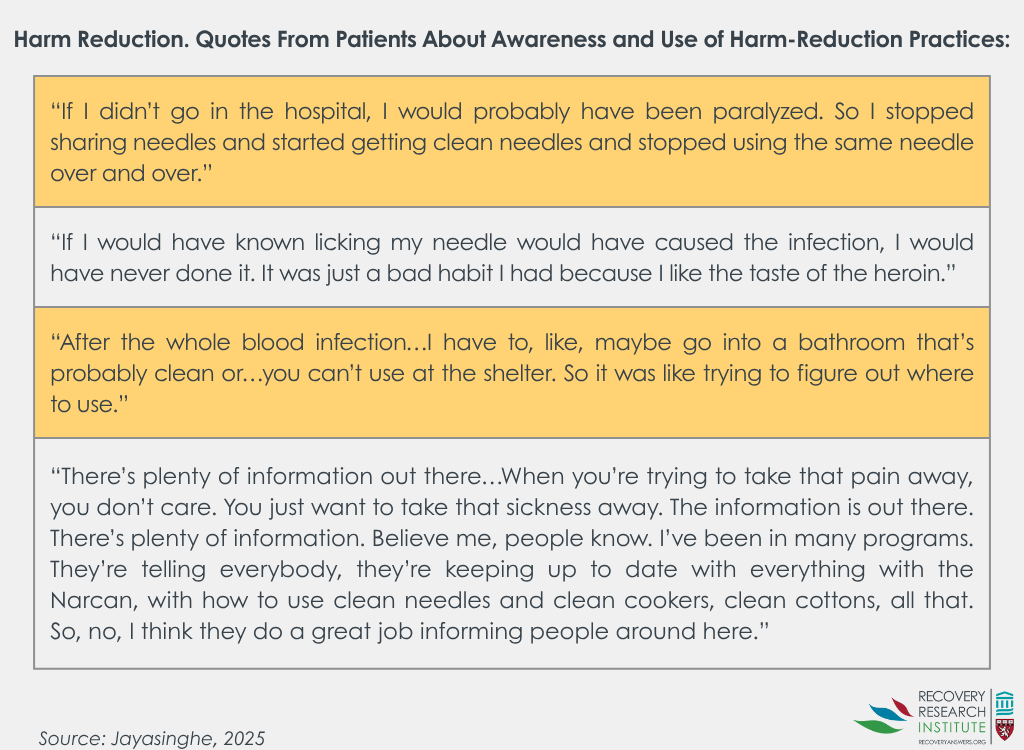
When asked about awareness and usefulness of harm-reduction practices, several patients noted that they started to use harm reduction practices following hospitalization to prevent future infections and related complications. Some patients said they were previously unaware of simple behavioral changes they could have made to prevent infection, while others were educated about harm reduction practices but weren’t always able to implement them prior to or after hospitalization, with some noting logistical barriers (e.g., finding a sterile space to inject).
Patients had mixed opinions on opioid use disorder medication treatments after hospitalization
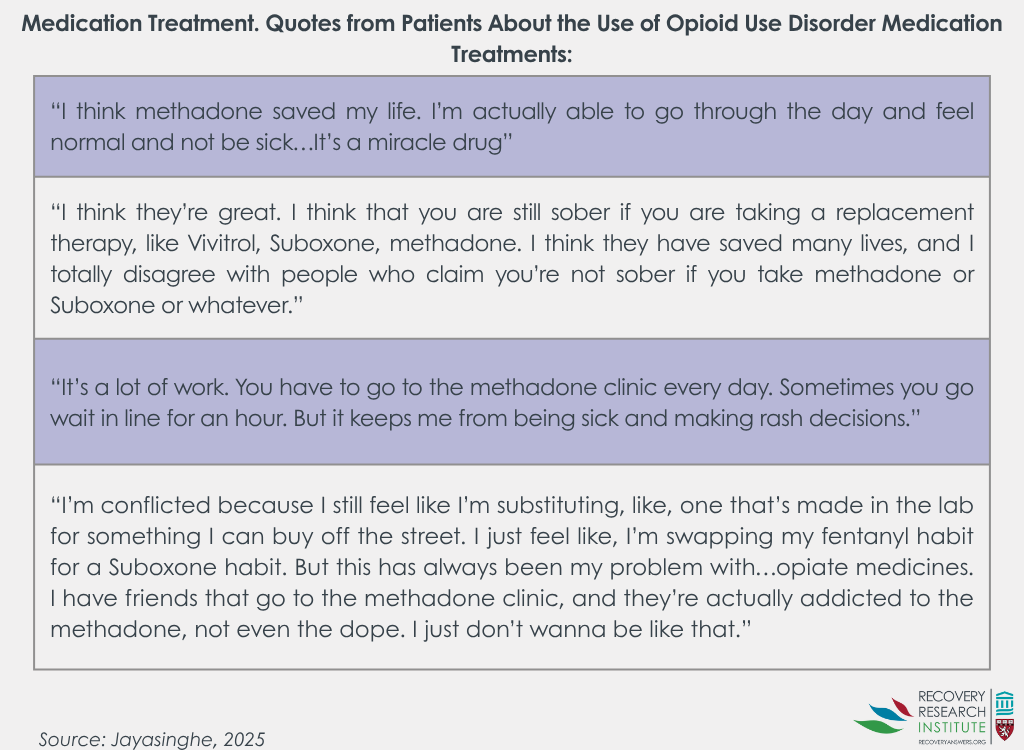
Patients broadly recognized the health benefits of opioid use disorder medication treatments and some noted gratitude for their lifesaving effects and ability to improve daily functioning. However, some patients still had concerns about medication treatment, noting the challenges associated with treatments requiring daily dosing (e.g., ‘liquid handcuffs’) and negative patient perceptions around physiological dependence on medications.
Hospitalization was often seen as an opportunity for patient reflection and behavior change
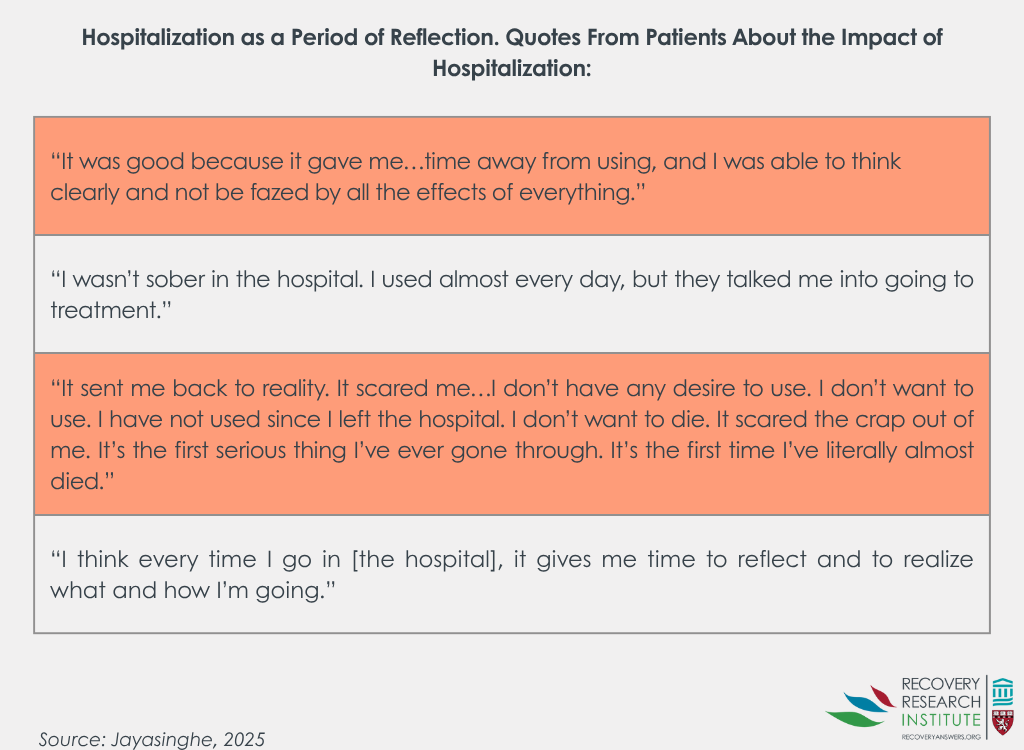
The majority of patients noted that being hospitalized for their infection led them to significantly reconsider their drug use and overall health. Many patients discussed how hospitalization acted as an interruption to their usual substance use patterns, with some opting to reduce drug use or start treatment as a result. Some noted hospitalization served as a meaningful warning and made them more aware of the severity of their disorder and worsening health. Patients with unstable housing at the time of hospitalization also noted the impact that environment had on their substance use, and how hospitalization offered a more stable environment for reflection on unhealthy behaviors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand the experiences and opinions of adults after a drug-related hospitalization, which can help inform and improve clinical approaches to engage patients with interventions during and post hospitalization. More specifically, this study of patients who were, on average, 330 days removed from the index hospital stay, provides a better understanding of patients’ willingness to engage in medication treatments and harm-reduction techniques after hospitalization for a serious drug injection-related infection. These findings can help inform procedures and approaches that may be more acceptable to patients and that could promote patient recovery and wellbeing after an injection-related infection.
Patients in this study saw hospitalization as an opportunity for reflection, with some noting that the environmental shift from chaotic day-to-day life and drug use to a more stable hospital environment, offered a period of reflection about self, substance use, and behavioral changes. This suggests that drug-related hospitalizations may be a good opportunity for timely interventions. For example, hospitalization may be a good time to educate patients about drug use risks, as well as potential harm-reduction strategies and treatment offerings they can engage in to avoid life threatening infections and hospitalizations in the future.
Even in the absence of timely interventions, being in a hospital setting and receiving care for more serious and sometimes life-threatening health conditions was enough to change the behavior of many patients. Forty percent of patients stopped using drugs altogether after hospitalization, suggesting that the health event may have acted as a wakeup call for patients to dramatically change their substance use behaviors. Though most patients continued to use drugs after hospitalization (60%), nearly all had changed their drug use behaviors in some way that reduced their risk of experiencing drug-related harms in the future. For example, some reduced use (e.g., less frequent use) and others used in safer ways (e.g., not reusing needles). Some patients noted that they learned information during their hospital stay that allowed them to start using harm-reduction behaviors that reduced their risk when using drugs. This suggests that hospital visits offer an ideal time to educate patients about harm-reduction techniques they can use to avoid health risks, as some individuals may not be educated about these practices. Indeed, prior research suggests that provider-patient interactions in hospital settings can help educate patients about the risks and benefits of harm reduction and medication treatments, and may even help link patients to these services.
Interestingly, despite this sample of patients having prior extensive experience with opioid use disorder medication treatments, some patients still felt uncertain about taking opioid use disorder medication after hospitalization. The vast majority acknowledged the lifesaving benefits of medication treatments, but beliefs about being physiologically dependent on a medication and about medication treatment dispensing (e.g., daily clinic visits for dosing) deterred individuals from wanting to take medication treatment after hospitalization. Beliefs like this are common and can impact treatment seeking decisions. Studies suggest 20-40% of individuals who receive opioid use disorder detoxification do not want to take a medication; strategies to engage these individuals in treatment and recovery supports are needed. Moreover, for those who do want medications but worry about the impact of daily dosing needs, for example, increasing the ease with which patients can access treatment and still live an autonomous life may help. Offering take-home doses of medication at earlier stages of treatment and providing telehealth appointments that don’t require patients to attend clinics on a regular basis or interfere with their daily work/life schedules may help change perceptions about treatment willingness. Indeed, extended-release injectable naltrexone or buprenorphine is one option that provides patients with greater scheduling flexibility, as it requires less frequent clinic visits. Adapted approaches to harm-reduction and medication treatment, that meet patients where they are at and help to increase their convenient access to life-saving services may ultimately help reduce drug-related harms.
As harm-reduction, treatment, and recovery services continue to expand and evolve, hospital visits are an ideal venue for timely education and introduction of patients to these services, which they may not otherwise be exposed to.
This study cohort consisted of patients with an extensive history of opioid use disorder medication treatment and findings may not apply to those without medication treatment histories.
The sample received care at a hospital with extensive resources for medication treatment and support services. Findings may not apply to all hospital settings or systems.
This study did not ask patients about the harm-reduction and medication treatment education or opportunities they received while hospitalized, only their views about these services after hospitalization.
Participants reflected on their experiences after hospital stays that for many, occurred quite a long time before; the average time between hospital stay and study participation was 330 days.
BOTTOM LINE
When patients present to the hospital with drug-related infections, it constitutes a timely opportunity for healthcare providers to educate and offer patients interventions like harm-reduction, treatment, and recovery services. However, not all patients are willing or able to engage in these practices and services, requiring additional research and adapted approaches to harm-reduction and medication treatment, that “meet patients where they are” and help to increase their convenient access to life-saving services (e.g., not requiring daily clinic visits for medication treatment, offering best practice advice for sterile injection in non-sterile spaces).
For individuals and families seeking recovery: Individuals who experience drug-related hospitalizations and their families are encouraged to talk to their hospital providers about services or behaviors they can engage in to help reduce future drug-related consequences. For example, many harm-reduction techniques, medication treatments (e.g., buprenorphine for opioid use disorder), and recovery support services can help patients avoid physical health ailments, overdose, death, and even illicit drug use.
For treatment professionals and treatment systems: Healthcare providers and systems are encouraged to educate their patients about harm-reduction techniques that can reduce drug-related harms, as well as medication treatments and places that they can receive these treatments in a way that is convenient for them. It is also important to educate patients about a variety of options for help seeking, including recovery support services like mutual help groups and recovery community centers that patients can have the option to engage in alongside or as an alternative to medication treatment or harm reduction services, as not all patients are able or willing to engage in certain pathways.
For scientists: Additional qualitative studies are needed in additional hospitals offering a range of services to better understand how hospital setting and personnel influence patient behaviors after injection-related hospitalization. Quantitative investigations and randomized trials of novel interventions for enhancing patient education about harm reduction, medication treatment, as well as recovery support services are needed to assess methods that enhance beneficial outcomes for patients after drug-related hospitalizations.
For policy makers: Harm reduction services and medication treatments have been shown to reduce criminal activity, overdose deaths, and the spread of infectious diseases. Hospitalization for drug injection-related infections presents an ideal opportunity for timely interventions that help educate patients and link them to services like harm reduction and medication treatment, that can ultimately help reduce individual and societal harm. Funding for research that develops and tests novel hospitalization and post-hospitalization programs to promote patient use of harm-reduction behaviors and treatment/recovery services will help enhance hospital programs and patient outcomes.
Individuals who inject drugs are at risk of injection-related infections and the rate of serious, life-threatening infections from drug injection are on the rise. These infections typically require a hospital stay with antibiotic treatment. It is also now standard practice to provide medication treatments for opioid use disorder (e.g., buprenorphine) onsite for people who are hospitalized for opioid-related reasons, such as an injection-related infection. However, even in states with greater availability of medication treatment, only half of individuals who present to the hospital with serious injection-related infections actually receive medication treatment for opioid use disorder (we do not know whether this is because they offered it and refused it, or were not offered it). Given buprenorphine/naloxone (commonly prescribed under the brand name, “Suboxone”) is considered the gold standard in opioid use disorder treatment and can help prevent overdose, this finding highlights an important treatment gap.
Hospitals offer an ideal location to educate patients about harm-reduction behaviors, deliver services (e.g., medication treatment), and link individuals to outpatient treatment and recovery support services that can help reduce drug-related harms and deaths. Yet, little is known about how serious injection-related hospitalizations affect patient’s substance use and willingness to engage in such services.
To help fill this knowledge gap, this study aimed to characterize patients’ perspectives on substance use, harm reduction, and medication treatments for opioid use disorder after hospitalization for injection-related infection. Gaining a better understanding of how individuals who had a hospital stay for an injection-related infection think about treatment and recovery could inform optimal clinical approaches that might better engage them with a helpful medication like buprenorphine/naloxone or some other harm reduction or recovery support service.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of adults hospitalized for a serious injection-related infection between 2020 and 2023, in which 30 patients completed questionnaires and interviews about their substance use, opinions on harm reduction and opioid use disorder medication treatments. Individuals were recruited from Boston Medical Center, an urban hospital in Massachusetts with comprehensive addiction and infection disease resources.
Eligible participants were recruited from hospital records and the community. All participants had experienced a serious infection related to injection drug use at least 2 weeks, and no more than 3 years, prior to study enrollment (median duration from infection to interview = 330 days). Infections related to injection drug use considered in this study required hospitalization and included, for example, endocarditis and bloodstream infection. At the time of infection, all participants also had diagnosed opioid use disorder.
Participants completed questionnaires about their demographics, substance use, and infection histories. During the semi-structured qualitative interviews, participants answered questions about the timeframe just before, during, and after hospitalization for a serious injection-related infection. Interviews asked about patient perspectives on their hospitalization experience and potential ways to improve care. Qualitative interviews were analyzed for themes related to the impact of hospitalization on subsequent substance use, perspectives on harm reduction, and perspectives on medication treatments for opioid use disorder.
The majority of participants were White Non-Hispanic (70.0%), men (63%), with a high-school or equivalent education (43%) and an average age of 39 years old. Thirty percent of participants were receiving disability income and 60% were living in their own home, alone or with other people, at the time of study participation. Patients experienced an average of 3 infections over their lifetime and were asked about the following types of infections that occurred most recently: endocarditis (33%), bacteremia (17%), osteomyelitis (30%), epidural abscess (13%), and septic arthritis (7%). Most patients reported finishing their prescribed antibiotic regimens for their infections, as instructed by their doctors (80%).
Opioids were reported as the preferred drug of choice for all but 1 participant (98%), who reported a stimulant preference. Fifty-seven percent of those who reported opioids as their preferred drug, also reported stimulant use. Nearly all patients had prior treatment experience with methadone (90%) and buprenorphine (87%), and 27% had been previously treated with extended-release injectable naltrexone, though not necessarily coinciding with when they were hospitalized. At the time of study participation, most patients were actively receiving treatment with methadone (50%), buprenorphine (27%), or extended-release naltrexone (7%); 16% of participants were not receiving any medication treatment.
WHAT DID THIS STUDY FIND?
Ongoing drug use after hospitalization was common, but many implemented harm-reduction techniques
After hospitalization for injection-related infection, 60% of patients continued to use drugs. Among the patients who continued to use drugs, 83% adopted harm reduction practices, including using less often or using in a safer way.
When asked about awareness and usefulness of harm-reduction practices, several patients noted that they started to use harm reduction practices following hospitalization to prevent future infections and related complications. Some patients said they were previously unaware of simple behavioral changes they could have made to prevent infection, while others were educated about harm reduction practices but weren’t always able to implement them prior to or after hospitalization, with some noting logistical barriers (e.g., finding a sterile space to inject).
Patients had mixed opinions on opioid use disorder medication treatments after hospitalization
Patients broadly recognized the health benefits of opioid use disorder medication treatments and some noted gratitude for their lifesaving effects and ability to improve daily functioning. However, some patients still had concerns about medication treatment, noting the challenges associated with treatments requiring daily dosing (e.g., ‘liquid handcuffs’) and negative patient perceptions around physiological dependence on medications.
Hospitalization was often seen as an opportunity for patient reflection and behavior change
The majority of patients noted that being hospitalized for their infection led them to significantly reconsider their drug use and overall health. Many patients discussed how hospitalization acted as an interruption to their usual substance use patterns, with some opting to reduce drug use or start treatment as a result. Some noted hospitalization served as a meaningful warning and made them more aware of the severity of their disorder and worsening health. Patients with unstable housing at the time of hospitalization also noted the impact that environment had on their substance use, and how hospitalization offered a more stable environment for reflection on unhealthy behaviors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand the experiences and opinions of adults after a drug-related hospitalization, which can help inform and improve clinical approaches to engage patients with interventions during and post hospitalization. More specifically, this study of patients who were, on average, 330 days removed from the index hospital stay, provides a better understanding of patients’ willingness to engage in medication treatments and harm-reduction techniques after hospitalization for a serious drug injection-related infection. These findings can help inform procedures and approaches that may be more acceptable to patients and that could promote patient recovery and wellbeing after an injection-related infection.
Patients in this study saw hospitalization as an opportunity for reflection, with some noting that the environmental shift from chaotic day-to-day life and drug use to a more stable hospital environment, offered a period of reflection about self, substance use, and behavioral changes. This suggests that drug-related hospitalizations may be a good opportunity for timely interventions. For example, hospitalization may be a good time to educate patients about drug use risks, as well as potential harm-reduction strategies and treatment offerings they can engage in to avoid life threatening infections and hospitalizations in the future.
Even in the absence of timely interventions, being in a hospital setting and receiving care for more serious and sometimes life-threatening health conditions was enough to change the behavior of many patients. Forty percent of patients stopped using drugs altogether after hospitalization, suggesting that the health event may have acted as a wakeup call for patients to dramatically change their substance use behaviors. Though most patients continued to use drugs after hospitalization (60%), nearly all had changed their drug use behaviors in some way that reduced their risk of experiencing drug-related harms in the future. For example, some reduced use (e.g., less frequent use) and others used in safer ways (e.g., not reusing needles). Some patients noted that they learned information during their hospital stay that allowed them to start using harm-reduction behaviors that reduced their risk when using drugs. This suggests that hospital visits offer an ideal time to educate patients about harm-reduction techniques they can use to avoid health risks, as some individuals may not be educated about these practices. Indeed, prior research suggests that provider-patient interactions in hospital settings can help educate patients about the risks and benefits of harm reduction and medication treatments, and may even help link patients to these services.
Interestingly, despite this sample of patients having prior extensive experience with opioid use disorder medication treatments, some patients still felt uncertain about taking opioid use disorder medication after hospitalization. The vast majority acknowledged the lifesaving benefits of medication treatments, but beliefs about being physiologically dependent on a medication and about medication treatment dispensing (e.g., daily clinic visits for dosing) deterred individuals from wanting to take medication treatment after hospitalization. Beliefs like this are common and can impact treatment seeking decisions. Studies suggest 20-40% of individuals who receive opioid use disorder detoxification do not want to take a medication; strategies to engage these individuals in treatment and recovery supports are needed. Moreover, for those who do want medications but worry about the impact of daily dosing needs, for example, increasing the ease with which patients can access treatment and still live an autonomous life may help. Offering take-home doses of medication at earlier stages of treatment and providing telehealth appointments that don’t require patients to attend clinics on a regular basis or interfere with their daily work/life schedules may help change perceptions about treatment willingness. Indeed, extended-release injectable naltrexone or buprenorphine is one option that provides patients with greater scheduling flexibility, as it requires less frequent clinic visits. Adapted approaches to harm-reduction and medication treatment, that meet patients where they are at and help to increase their convenient access to life-saving services may ultimately help reduce drug-related harms.
As harm-reduction, treatment, and recovery services continue to expand and evolve, hospital visits are an ideal venue for timely education and introduction of patients to these services, which they may not otherwise be exposed to.
This study cohort consisted of patients with an extensive history of opioid use disorder medication treatment and findings may not apply to those without medication treatment histories.
The sample received care at a hospital with extensive resources for medication treatment and support services. Findings may not apply to all hospital settings or systems.
This study did not ask patients about the harm-reduction and medication treatment education or opportunities they received while hospitalized, only their views about these services after hospitalization.
Participants reflected on their experiences after hospital stays that for many, occurred quite a long time before; the average time between hospital stay and study participation was 330 days.
BOTTOM LINE
When patients present to the hospital with drug-related infections, it constitutes a timely opportunity for healthcare providers to educate and offer patients interventions like harm-reduction, treatment, and recovery services. However, not all patients are willing or able to engage in these practices and services, requiring additional research and adapted approaches to harm-reduction and medication treatment, that “meet patients where they are” and help to increase their convenient access to life-saving services (e.g., not requiring daily clinic visits for medication treatment, offering best practice advice for sterile injection in non-sterile spaces).
For individuals and families seeking recovery: Individuals who experience drug-related hospitalizations and their families are encouraged to talk to their hospital providers about services or behaviors they can engage in to help reduce future drug-related consequences. For example, many harm-reduction techniques, medication treatments (e.g., buprenorphine for opioid use disorder), and recovery support services can help patients avoid physical health ailments, overdose, death, and even illicit drug use.
For treatment professionals and treatment systems: Healthcare providers and systems are encouraged to educate their patients about harm-reduction techniques that can reduce drug-related harms, as well as medication treatments and places that they can receive these treatments in a way that is convenient for them. It is also important to educate patients about a variety of options for help seeking, including recovery support services like mutual help groups and recovery community centers that patients can have the option to engage in alongside or as an alternative to medication treatment or harm reduction services, as not all patients are able or willing to engage in certain pathways.
For scientists: Additional qualitative studies are needed in additional hospitals offering a range of services to better understand how hospital setting and personnel influence patient behaviors after injection-related hospitalization. Quantitative investigations and randomized trials of novel interventions for enhancing patient education about harm reduction, medication treatment, as well as recovery support services are needed to assess methods that enhance beneficial outcomes for patients after drug-related hospitalizations.
For policy makers: Harm reduction services and medication treatments have been shown to reduce criminal activity, overdose deaths, and the spread of infectious diseases. Hospitalization for drug injection-related infections presents an ideal opportunity for timely interventions that help educate patients and link them to services like harm reduction and medication treatment, that can ultimately help reduce individual and societal harm. Funding for research that develops and tests novel hospitalization and post-hospitalization programs to promote patient use of harm-reduction behaviors and treatment/recovery services will help enhance hospital programs and patient outcomes.
Individuals who inject drugs are at risk of injection-related infections and the rate of serious, life-threatening infections from drug injection are on the rise. These infections typically require a hospital stay with antibiotic treatment. It is also now standard practice to provide medication treatments for opioid use disorder (e.g., buprenorphine) onsite for people who are hospitalized for opioid-related reasons, such as an injection-related infection. However, even in states with greater availability of medication treatment, only half of individuals who present to the hospital with serious injection-related infections actually receive medication treatment for opioid use disorder (we do not know whether this is because they offered it and refused it, or were not offered it). Given buprenorphine/naloxone (commonly prescribed under the brand name, “Suboxone”) is considered the gold standard in opioid use disorder treatment and can help prevent overdose, this finding highlights an important treatment gap.
Hospitals offer an ideal location to educate patients about harm-reduction behaviors, deliver services (e.g., medication treatment), and link individuals to outpatient treatment and recovery support services that can help reduce drug-related harms and deaths. Yet, little is known about how serious injection-related hospitalizations affect patient’s substance use and willingness to engage in such services.
To help fill this knowledge gap, this study aimed to characterize patients’ perspectives on substance use, harm reduction, and medication treatments for opioid use disorder after hospitalization for injection-related infection. Gaining a better understanding of how individuals who had a hospital stay for an injection-related infection think about treatment and recovery could inform optimal clinical approaches that might better engage them with a helpful medication like buprenorphine/naloxone or some other harm reduction or recovery support service.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of adults hospitalized for a serious injection-related infection between 2020 and 2023, in which 30 patients completed questionnaires and interviews about their substance use, opinions on harm reduction and opioid use disorder medication treatments. Individuals were recruited from Boston Medical Center, an urban hospital in Massachusetts with comprehensive addiction and infection disease resources.
Eligible participants were recruited from hospital records and the community. All participants had experienced a serious infection related to injection drug use at least 2 weeks, and no more than 3 years, prior to study enrollment (median duration from infection to interview = 330 days). Infections related to injection drug use considered in this study required hospitalization and included, for example, endocarditis and bloodstream infection. At the time of infection, all participants also had diagnosed opioid use disorder.
Participants completed questionnaires about their demographics, substance use, and infection histories. During the semi-structured qualitative interviews, participants answered questions about the timeframe just before, during, and after hospitalization for a serious injection-related infection. Interviews asked about patient perspectives on their hospitalization experience and potential ways to improve care. Qualitative interviews were analyzed for themes related to the impact of hospitalization on subsequent substance use, perspectives on harm reduction, and perspectives on medication treatments for opioid use disorder.
The majority of participants were White Non-Hispanic (70.0%), men (63%), with a high-school or equivalent education (43%) and an average age of 39 years old. Thirty percent of participants were receiving disability income and 60% were living in their own home, alone or with other people, at the time of study participation. Patients experienced an average of 3 infections over their lifetime and were asked about the following types of infections that occurred most recently: endocarditis (33%), bacteremia (17%), osteomyelitis (30%), epidural abscess (13%), and septic arthritis (7%). Most patients reported finishing their prescribed antibiotic regimens for their infections, as instructed by their doctors (80%).
Opioids were reported as the preferred drug of choice for all but 1 participant (98%), who reported a stimulant preference. Fifty-seven percent of those who reported opioids as their preferred drug, also reported stimulant use. Nearly all patients had prior treatment experience with methadone (90%) and buprenorphine (87%), and 27% had been previously treated with extended-release injectable naltrexone, though not necessarily coinciding with when they were hospitalized. At the time of study participation, most patients were actively receiving treatment with methadone (50%), buprenorphine (27%), or extended-release naltrexone (7%); 16% of participants were not receiving any medication treatment.
WHAT DID THIS STUDY FIND?
Ongoing drug use after hospitalization was common, but many implemented harm-reduction techniques
After hospitalization for injection-related infection, 60% of patients continued to use drugs. Among the patients who continued to use drugs, 83% adopted harm reduction practices, including using less often or using in a safer way.
When asked about awareness and usefulness of harm-reduction practices, several patients noted that they started to use harm reduction practices following hospitalization to prevent future infections and related complications. Some patients said they were previously unaware of simple behavioral changes they could have made to prevent infection, while others were educated about harm reduction practices but weren’t always able to implement them prior to or after hospitalization, with some noting logistical barriers (e.g., finding a sterile space to inject).
Patients had mixed opinions on opioid use disorder medication treatments after hospitalization
Patients broadly recognized the health benefits of opioid use disorder medication treatments and some noted gratitude for their lifesaving effects and ability to improve daily functioning. However, some patients still had concerns about medication treatment, noting the challenges associated with treatments requiring daily dosing (e.g., ‘liquid handcuffs’) and negative patient perceptions around physiological dependence on medications.
Hospitalization was often seen as an opportunity for patient reflection and behavior change
The majority of patients noted that being hospitalized for their infection led them to significantly reconsider their drug use and overall health. Many patients discussed how hospitalization acted as an interruption to their usual substance use patterns, with some opting to reduce drug use or start treatment as a result. Some noted hospitalization served as a meaningful warning and made them more aware of the severity of their disorder and worsening health. Patients with unstable housing at the time of hospitalization also noted the impact that environment had on their substance use, and how hospitalization offered a more stable environment for reflection on unhealthy behaviors.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand the experiences and opinions of adults after a drug-related hospitalization, which can help inform and improve clinical approaches to engage patients with interventions during and post hospitalization. More specifically, this study of patients who were, on average, 330 days removed from the index hospital stay, provides a better understanding of patients’ willingness to engage in medication treatments and harm-reduction techniques after hospitalization for a serious drug injection-related infection. These findings can help inform procedures and approaches that may be more acceptable to patients and that could promote patient recovery and wellbeing after an injection-related infection.
Patients in this study saw hospitalization as an opportunity for reflection, with some noting that the environmental shift from chaotic day-to-day life and drug use to a more stable hospital environment, offered a period of reflection about self, substance use, and behavioral changes. This suggests that drug-related hospitalizations may be a good opportunity for timely interventions. For example, hospitalization may be a good time to educate patients about drug use risks, as well as potential harm-reduction strategies and treatment offerings they can engage in to avoid life threatening infections and hospitalizations in the future.
Even in the absence of timely interventions, being in a hospital setting and receiving care for more serious and sometimes life-threatening health conditions was enough to change the behavior of many patients. Forty percent of patients stopped using drugs altogether after hospitalization, suggesting that the health event may have acted as a wakeup call for patients to dramatically change their substance use behaviors. Though most patients continued to use drugs after hospitalization (60%), nearly all had changed their drug use behaviors in some way that reduced their risk of experiencing drug-related harms in the future. For example, some reduced use (e.g., less frequent use) and others used in safer ways (e.g., not reusing needles). Some patients noted that they learned information during their hospital stay that allowed them to start using harm-reduction behaviors that reduced their risk when using drugs. This suggests that hospital visits offer an ideal time to educate patients about harm-reduction techniques they can use to avoid health risks, as some individuals may not be educated about these practices. Indeed, prior research suggests that provider-patient interactions in hospital settings can help educate patients about the risks and benefits of harm reduction and medication treatments, and may even help link patients to these services.
Interestingly, despite this sample of patients having prior extensive experience with opioid use disorder medication treatments, some patients still felt uncertain about taking opioid use disorder medication after hospitalization. The vast majority acknowledged the lifesaving benefits of medication treatments, but beliefs about being physiologically dependent on a medication and about medication treatment dispensing (e.g., daily clinic visits for dosing) deterred individuals from wanting to take medication treatment after hospitalization. Beliefs like this are common and can impact treatment seeking decisions. Studies suggest 20-40% of individuals who receive opioid use disorder detoxification do not want to take a medication; strategies to engage these individuals in treatment and recovery supports are needed. Moreover, for those who do want medications but worry about the impact of daily dosing needs, for example, increasing the ease with which patients can access treatment and still live an autonomous life may help. Offering take-home doses of medication at earlier stages of treatment and providing telehealth appointments that don’t require patients to attend clinics on a regular basis or interfere with their daily work/life schedules may help change perceptions about treatment willingness. Indeed, extended-release injectable naltrexone or buprenorphine is one option that provides patients with greater scheduling flexibility, as it requires less frequent clinic visits. Adapted approaches to harm-reduction and medication treatment, that meet patients where they are at and help to increase their convenient access to life-saving services may ultimately help reduce drug-related harms.
As harm-reduction, treatment, and recovery services continue to expand and evolve, hospital visits are an ideal venue for timely education and introduction of patients to these services, which they may not otherwise be exposed to.
This study cohort consisted of patients with an extensive history of opioid use disorder medication treatment and findings may not apply to those without medication treatment histories.
The sample received care at a hospital with extensive resources for medication treatment and support services. Findings may not apply to all hospital settings or systems.
This study did not ask patients about the harm-reduction and medication treatment education or opportunities they received while hospitalized, only their views about these services after hospitalization.
Participants reflected on their experiences after hospital stays that for many, occurred quite a long time before; the average time between hospital stay and study participation was 330 days.
BOTTOM LINE
When patients present to the hospital with drug-related infections, it constitutes a timely opportunity for healthcare providers to educate and offer patients interventions like harm-reduction, treatment, and recovery services. However, not all patients are willing or able to engage in these practices and services, requiring additional research and adapted approaches to harm-reduction and medication treatment, that “meet patients where they are” and help to increase their convenient access to life-saving services (e.g., not requiring daily clinic visits for medication treatment, offering best practice advice for sterile injection in non-sterile spaces).
For individuals and families seeking recovery: Individuals who experience drug-related hospitalizations and their families are encouraged to talk to their hospital providers about services or behaviors they can engage in to help reduce future drug-related consequences. For example, many harm-reduction techniques, medication treatments (e.g., buprenorphine for opioid use disorder), and recovery support services can help patients avoid physical health ailments, overdose, death, and even illicit drug use.
For treatment professionals and treatment systems: Healthcare providers and systems are encouraged to educate their patients about harm-reduction techniques that can reduce drug-related harms, as well as medication treatments and places that they can receive these treatments in a way that is convenient for them. It is also important to educate patients about a variety of options for help seeking, including recovery support services like mutual help groups and recovery community centers that patients can have the option to engage in alongside or as an alternative to medication treatment or harm reduction services, as not all patients are able or willing to engage in certain pathways.
For scientists: Additional qualitative studies are needed in additional hospitals offering a range of services to better understand how hospital setting and personnel influence patient behaviors after injection-related hospitalization. Quantitative investigations and randomized trials of novel interventions for enhancing patient education about harm reduction, medication treatment, as well as recovery support services are needed to assess methods that enhance beneficial outcomes for patients after drug-related hospitalizations.
For policy makers: Harm reduction services and medication treatments have been shown to reduce criminal activity, overdose deaths, and the spread of infectious diseases. Hospitalization for drug injection-related infections presents an ideal opportunity for timely interventions that help educate patients and link them to services like harm reduction and medication treatment, that can ultimately help reduce individual and societal harm. Funding for research that develops and tests novel hospitalization and post-hospitalization programs to promote patient use of harm-reduction behaviors and treatment/recovery services will help enhance hospital programs and patient outcomes.