Health record data adds further support for the role of family history in youth substance use disorder
Prior research has shown that genes, family, friends, and neighborhoods all influence the potential for developing a substance use disorder during the teenage years. This evidence, however, has tended to come from small samples or contain only partial or limited information when sample sizes were large. In contrast, this study used a population-based sample of over 100,000 Canadian youth with more fully complete health record data and explored to what degree having a parent or a sibling with a substance use disorder increased the risk of developing a substance use disorder during adolescence.
Many factors influence the potential for developing a substance use disorder during the teenage years, including individual characteristics (e.g., genes), external influences (e.g., family, friends), and different contexts (e.g.,homes, neighborhoods). When considering the role of families, research has demonstrated that both the genetics shared among offspring as well as the situational characteristics and experiences shared from living together can be risk factors for developing a substance use disorder. For example, research suggests that adverse childhood experiences, co-occurring mental health conditions, and low socio-economic status are all strong risk factors for a substance use disorder. As well, research has demonstrated the strong influence of parenting behaviors and parent substance use on their child’s substance use behavior. For example, how parents respond to their children’s substance use and other risky behaviors (e.g., behavioral reinforcement) and the behaviors they model for their children (e.g., vicarious learning) are both associated with the likelihood of substance use disorder. Finally, living in a high stress or deprived area can be a risk factor for substance use and ultimately, for developing a substance use disorder.
Research using clinical health records to examine the risks of family addiction history on youth substance use disorder highlights the potentially real-world utility of using family health records to identify youth at risk for substance use disorder themselves. In this study, the researchers used data collected from several electronic health records to create a population-based dataset and explore whether having a parent or a sibling with a diagnosed substance use disorder increased the risk of developing a substance use disorder during adolescence. They also examined whether several factors influenced this risk such as child sex, the presence of ADHD, mood, or anxiety disorders, neighborhood location, and neighborhood income-level.
HOW WAS THIS STUDY CONDUCTED?
This study used the following administrative health-care databases in Manitoba, Canada, to create a population-based dataset for children born in Manitoba from April 1, 1984, through March 31, 2000: (1) Manitoba Health Insurance Registry; (2) Medical Services data set; (3) Hospital Abstract data set; (4) Hospital Newborn to Mother Link Registry data set; (5) Statistics Canada; (6) Manitoba Multigenerational Cohort. The research team selected all first- and second-born children to use in the population-based dataset.
The authors used (1) parental history of substance use disorder diagnosis and (2) sibling history of substance use disorder diagnosis during adolescence to predict a diagnosis of substance use disorder during adolescence. The substance use disorder diagnoses for all three groups (parent, sibling, child) were based on hospitalization or physician visit records. Adolescent SUD diagnosis was defined as having at least one hospitalization or one physician visit with a diagnosis of alcohol or drug psychoses, alcohol or drug dependence, or non-dependent abuse of drugs when the youth was between 13 and 18 years old.
The following factors were included as statistical controls in their models: mother’s age at first birth, sex, birth order, presence of an additional mental health condition (ADHD, conduct disorder, mood disorder, or anxiety disorder), geographic location of home, and income level of the neighborhood. In the models that examined the risk of diagnosis of substance use disorder during adolescence due to sibling history of substance use disorder diagnosis, the parental history of substance use disorder diagnosis was also included as a statistical control. As a form of sensitivity analysis, the authors also examined whether the child’s age when the service with parental substance use disorder occurred impacting the study findings. They used two developmental periods: (1) before the child was 5 years old or (2) when the child was between 5 and 13 years old.
Of the sample of 134,389 adolescents in the sample, about 2% had a diagnosis of substance use disorder during adolescence and 49% were male. About 10% of the total sample had a mother and 11% had a father with a history of a substance use disorder diagnosis. There were 31,307 sibling pairs included in the sample.
WHAT DID THIS STUDY FIND?
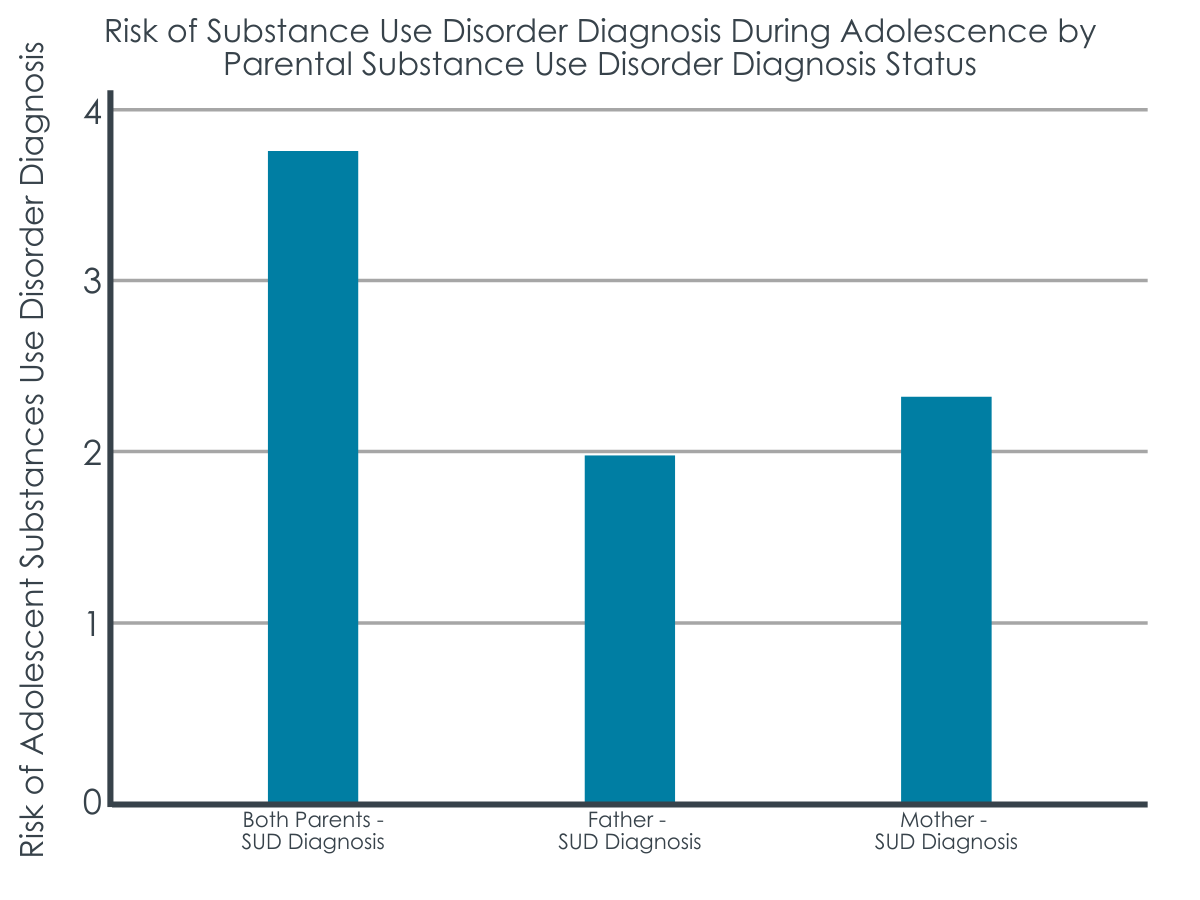
Parental substance use disorder diagnosis increased risk for substance use disorder diagnosis during adolescence.
In models that account for all included factors, children who had both parents diagnosed with a substance use disorder were 3.74 times more likely to be diagnosed with a substance use disorder during adolescence. This risk was slightly increased for female compared to male children. The risk was reduced when only one of the two parents were diagnosed. For families where the father had a diagnosis, the risk was 1.98 greater than if no parent had a diagnosis, whereas for families where the mother had a diagnosis, the risk was 2.37 greater than if no parent had a diagnosis. The child’s age at the time of parent substance use disorder diagnosis (5 or younger versus 5 or older) did not influence the risk of developing a substance use disorder during adolescence.
Having an older sibling with substance use disorder also increased risk for substance use disorder diagnosis during adolescence.
In models that account for all factors including have a parent with a substance use disorder diagnosis, less than 2% of the sample had a sibling with a substance use disorder diagnosed during adolescence. Among youth that had an older sibling with the same mother and father, their risk of a substance use disorder diagnosis during adolescence was 3.85 higher than youth whose older sibling did not have a diagnosed substance use disorder. When siblings were defined by having the same mother only, the risk remained – 2.73 times greater – albeit to a lesser degree.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This population-based study shows that family health records can be used to identify the risk of substance use disorder for adolescents. Studies like this can ultimately help health care systems understand where prevention, treatment, and recovery efforts could be targeted for at-risk youth and families.
In this study which used electronic health record data of a population-based sample ofover 100,000 youth in Canada, the risk of developing a substance use disorder during adolescence substantially increased if a parent or sibling was diagnosed with a substance use disorder. This risk was highest when both parents were diagnosed with a substance use disorder or when an older sibling was diagnosed.Yet, the findings, while significant, still leave room for a variety of other known contributing factors to developing a substance use disorder during adolescence, including, for example, adverse childhood experiences, genetic vulnerability, parenting style and monitoring, and friends and peers social influence.
Of note, the 2% prevalence of substance use disorder in this population study of Manitoba, Canada is lower than the 6-7% which is typically found in the annual USNational Survey of Drug Use and Health among 12–17-yearold’s. This could be due to the fact that rather than self-report, the substance use diagnosis in this study is dependent on youth and their families toengage in the healthcare system and have a diagnosis recorded as part of that engagement. Despite universal healthcare in Canada, there are many reasons why an adolescent might not have adiagnosis of substance use disorder in their health record although they might meet the criteria for one. For example, if substance use is not the focus of the healthcare visit, if there is a reluctance to make a substance use history part of the formal clinical record due to privacy or stigma concerns, orif there is no systemic attempt at screening, milder forms of substance usedisorders might not be identified, diagnosed, or documented. Thus, the sample of 2% in this study is likelyindicative of those youth who have severe and obvious substance use disorder.
Although the study identified the relationship between family history of substance use disorder and the risk of developing a substance use disorder during adolescence, it did not examine mechanisms of this relationship (e.g., whether the increased risk was due to genetic or environmental influences). Future research should examine the relative contribution of these different factors as well as the processes of risk in order to determine the dynamic nature of the key driving factors of increased risk.
The study did not account for treatment of family members or for history of substance use disorders prior to the birth of the child, so could be missing additional key risk factors. As well, it primarily focused on individual- and family-level characteristics but ignored additional key environmental factors (e.g., alcohol/drug availability).
Use of the electronic health record data is a strength of this study in that it provides an objective diagnosis of substance use disorder in youth and their families. Yet, these data might be missing individuals who meet substance use disorder criteria but are not screened during a healthcare encounter or if providers failed to document this in their chart due to stigma, or for other reasons.
BOTTOM LINE
In this large-scale and population-based study using electronic health records of Manitoba, Canada residents, the researchers found that the risk of developing a substance use disorder during adolescence was at least 2-3 times higher if a parent or sibling was diagnosed with a substance use disorder. While this highlights the utility of family health record data in the identification of adolescent substance use disorder risk, it’s important to remember that there are other risk factors to developing a substance use disorder during adolescence, some of which confer greater risk than the relationships reported here.
For individuals and families seeking recovery: Knowing youth’sfamily history around substance use disorders may help alert providersso they canengage in proper screening, help identify and address problematic family dynamics, and engage necessary supports for all affected family members. Youth-serving recovery programs such as recovery high schools and alternative peer groupsoften work to incorporate all family members in recovery support activities and there may be other opportunities in the clinical care setting to intervene with youth and their family members.
For treatment professionals and treatment systems: All patients enter clinical encounters with unique protective and risk factorsrelated to their potential to use substances. Knowing someone’s family history around substance use disorders may help alert providersso they canhelp to address family dynamics and engage supports for all affected family members. Some community–based programs that serve youth (e.g., recovery high schools and alternative peer groups) often provide outreach and programming for all family members in recovery support activities and there may be other opportunities in the clinical care setting to intervene with youth and their family members.
For scientists:Research is needed to better identify the mechanisms by which family history of substance use disorders increase the risk of developing a substance use disorder among offspring during adolescence and how these same factors can best be addressed in prevention and treatment programs. Studies that measure a wider array of factors related to the different sources of influence – individual, interindividual, and community – and that measure these with greater precision, are also needed to tease out these complex and intersecting relationships.
For policy makers: Family experience with substance use disorder can have repercussions on many outcomes (i.e., education/income mobility, health, mental health) for future generations. Infrastructure to support policy and programs that help to identify, prevent, and address substance use disorders and their consequences for the entire family might help break the generational impact of a substance use disorder history.
Many factors influence the potential for developing a substance use disorder during the teenage years, including individual characteristics (e.g., genes), external influences (e.g., family, friends), and different contexts (e.g.,homes, neighborhoods). When considering the role of families, research has demonstrated that both the genetics shared among offspring as well as the situational characteristics and experiences shared from living together can be risk factors for developing a substance use disorder. For example, research suggests that adverse childhood experiences, co-occurring mental health conditions, and low socio-economic status are all strong risk factors for a substance use disorder. As well, research has demonstrated the strong influence of parenting behaviors and parent substance use on their child’s substance use behavior. For example, how parents respond to their children’s substance use and other risky behaviors (e.g., behavioral reinforcement) and the behaviors they model for their children (e.g., vicarious learning) are both associated with the likelihood of substance use disorder. Finally, living in a high stress or deprived area can be a risk factor for substance use and ultimately, for developing a substance use disorder.
Research using clinical health records to examine the risks of family addiction history on youth substance use disorder highlights the potentially real-world utility of using family health records to identify youth at risk for substance use disorder themselves. In this study, the researchers used data collected from several electronic health records to create a population-based dataset and explore whether having a parent or a sibling with a diagnosed substance use disorder increased the risk of developing a substance use disorder during adolescence. They also examined whether several factors influenced this risk such as child sex, the presence of ADHD, mood, or anxiety disorders, neighborhood location, and neighborhood income-level.
HOW WAS THIS STUDY CONDUCTED?
This study used the following administrative health-care databases in Manitoba, Canada, to create a population-based dataset for children born in Manitoba from April 1, 1984, through March 31, 2000: (1) Manitoba Health Insurance Registry; (2) Medical Services data set; (3) Hospital Abstract data set; (4) Hospital Newborn to Mother Link Registry data set; (5) Statistics Canada; (6) Manitoba Multigenerational Cohort. The research team selected all first- and second-born children to use in the population-based dataset.
The authors used (1) parental history of substance use disorder diagnosis and (2) sibling history of substance use disorder diagnosis during adolescence to predict a diagnosis of substance use disorder during adolescence. The substance use disorder diagnoses for all three groups (parent, sibling, child) were based on hospitalization or physician visit records. Adolescent SUD diagnosis was defined as having at least one hospitalization or one physician visit with a diagnosis of alcohol or drug psychoses, alcohol or drug dependence, or non-dependent abuse of drugs when the youth was between 13 and 18 years old.
The following factors were included as statistical controls in their models: mother’s age at first birth, sex, birth order, presence of an additional mental health condition (ADHD, conduct disorder, mood disorder, or anxiety disorder), geographic location of home, and income level of the neighborhood. In the models that examined the risk of diagnosis of substance use disorder during adolescence due to sibling history of substance use disorder diagnosis, the parental history of substance use disorder diagnosis was also included as a statistical control. As a form of sensitivity analysis, the authors also examined whether the child’s age when the service with parental substance use disorder occurred impacting the study findings. They used two developmental periods: (1) before the child was 5 years old or (2) when the child was between 5 and 13 years old.
Of the sample of 134,389 adolescents in the sample, about 2% had a diagnosis of substance use disorder during adolescence and 49% were male. About 10% of the total sample had a mother and 11% had a father with a history of a substance use disorder diagnosis. There were 31,307 sibling pairs included in the sample.
WHAT DID THIS STUDY FIND?
Parental substance use disorder diagnosis increased risk for substance use disorder diagnosis during adolescence.
In models that account for all included factors, children who had both parents diagnosed with a substance use disorder were 3.74 times more likely to be diagnosed with a substance use disorder during adolescence. This risk was slightly increased for female compared to male children. The risk was reduced when only one of the two parents were diagnosed. For families where the father had a diagnosis, the risk was 1.98 greater than if no parent had a diagnosis, whereas for families where the mother had a diagnosis, the risk was 2.37 greater than if no parent had a diagnosis. The child’s age at the time of parent substance use disorder diagnosis (5 or younger versus 5 or older) did not influence the risk of developing a substance use disorder during adolescence.
Having an older sibling with substance use disorder also increased risk for substance use disorder diagnosis during adolescence.
In models that account for all factors including have a parent with a substance use disorder diagnosis, less than 2% of the sample had a sibling with a substance use disorder diagnosed during adolescence. Among youth that had an older sibling with the same mother and father, their risk of a substance use disorder diagnosis during adolescence was 3.85 higher than youth whose older sibling did not have a diagnosed substance use disorder. When siblings were defined by having the same mother only, the risk remained – 2.73 times greater – albeit to a lesser degree.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This population-based study shows that family health records can be used to identify the risk of substance use disorder for adolescents. Studies like this can ultimately help health care systems understand where prevention, treatment, and recovery efforts could be targeted for at-risk youth and families.
In this study which used electronic health record data of a population-based sample ofover 100,000 youth in Canada, the risk of developing a substance use disorder during adolescence substantially increased if a parent or sibling was diagnosed with a substance use disorder. This risk was highest when both parents were diagnosed with a substance use disorder or when an older sibling was diagnosed.Yet, the findings, while significant, still leave room for a variety of other known contributing factors to developing a substance use disorder during adolescence, including, for example, adverse childhood experiences, genetic vulnerability, parenting style and monitoring, and friends and peers social influence.
Of note, the 2% prevalence of substance use disorder in this population study of Manitoba, Canada is lower than the 6-7% which is typically found in the annual USNational Survey of Drug Use and Health among 12–17-yearold’s. This could be due to the fact that rather than self-report, the substance use diagnosis in this study is dependent on youth and their families toengage in the healthcare system and have a diagnosis recorded as part of that engagement. Despite universal healthcare in Canada, there are many reasons why an adolescent might not have adiagnosis of substance use disorder in their health record although they might meet the criteria for one. For example, if substance use is not the focus of the healthcare visit, if there is a reluctance to make a substance use history part of the formal clinical record due to privacy or stigma concerns, orif there is no systemic attempt at screening, milder forms of substance usedisorders might not be identified, diagnosed, or documented. Thus, the sample of 2% in this study is likelyindicative of those youth who have severe and obvious substance use disorder.
Although the study identified the relationship between family history of substance use disorder and the risk of developing a substance use disorder during adolescence, it did not examine mechanisms of this relationship (e.g., whether the increased risk was due to genetic or environmental influences). Future research should examine the relative contribution of these different factors as well as the processes of risk in order to determine the dynamic nature of the key driving factors of increased risk.
The study did not account for treatment of family members or for history of substance use disorders prior to the birth of the child, so could be missing additional key risk factors. As well, it primarily focused on individual- and family-level characteristics but ignored additional key environmental factors (e.g., alcohol/drug availability).
Use of the electronic health record data is a strength of this study in that it provides an objective diagnosis of substance use disorder in youth and their families. Yet, these data might be missing individuals who meet substance use disorder criteria but are not screened during a healthcare encounter or if providers failed to document this in their chart due to stigma, or for other reasons.
BOTTOM LINE
In this large-scale and population-based study using electronic health records of Manitoba, Canada residents, the researchers found that the risk of developing a substance use disorder during adolescence was at least 2-3 times higher if a parent or sibling was diagnosed with a substance use disorder. While this highlights the utility of family health record data in the identification of adolescent substance use disorder risk, it’s important to remember that there are other risk factors to developing a substance use disorder during adolescence, some of which confer greater risk than the relationships reported here.
For individuals and families seeking recovery: Knowing youth’sfamily history around substance use disorders may help alert providersso they canengage in proper screening, help identify and address problematic family dynamics, and engage necessary supports for all affected family members. Youth-serving recovery programs such as recovery high schools and alternative peer groupsoften work to incorporate all family members in recovery support activities and there may be other opportunities in the clinical care setting to intervene with youth and their family members.
For treatment professionals and treatment systems: All patients enter clinical encounters with unique protective and risk factorsrelated to their potential to use substances. Knowing someone’s family history around substance use disorders may help alert providersso they canhelp to address family dynamics and engage supports for all affected family members. Some community–based programs that serve youth (e.g., recovery high schools and alternative peer groups) often provide outreach and programming for all family members in recovery support activities and there may be other opportunities in the clinical care setting to intervene with youth and their family members.
For scientists:Research is needed to better identify the mechanisms by which family history of substance use disorders increase the risk of developing a substance use disorder among offspring during adolescence and how these same factors can best be addressed in prevention and treatment programs. Studies that measure a wider array of factors related to the different sources of influence – individual, interindividual, and community – and that measure these with greater precision, are also needed to tease out these complex and intersecting relationships.
For policy makers: Family experience with substance use disorder can have repercussions on many outcomes (i.e., education/income mobility, health, mental health) for future generations. Infrastructure to support policy and programs that help to identify, prevent, and address substance use disorders and their consequences for the entire family might help break the generational impact of a substance use disorder history.
Many factors influence the potential for developing a substance use disorder during the teenage years, including individual characteristics (e.g., genes), external influences (e.g., family, friends), and different contexts (e.g.,homes, neighborhoods). When considering the role of families, research has demonstrated that both the genetics shared among offspring as well as the situational characteristics and experiences shared from living together can be risk factors for developing a substance use disorder. For example, research suggests that adverse childhood experiences, co-occurring mental health conditions, and low socio-economic status are all strong risk factors for a substance use disorder. As well, research has demonstrated the strong influence of parenting behaviors and parent substance use on their child’s substance use behavior. For example, how parents respond to their children’s substance use and other risky behaviors (e.g., behavioral reinforcement) and the behaviors they model for their children (e.g., vicarious learning) are both associated with the likelihood of substance use disorder. Finally, living in a high stress or deprived area can be a risk factor for substance use and ultimately, for developing a substance use disorder.
Research using clinical health records to examine the risks of family addiction history on youth substance use disorder highlights the potentially real-world utility of using family health records to identify youth at risk for substance use disorder themselves. In this study, the researchers used data collected from several electronic health records to create a population-based dataset and explore whether having a parent or a sibling with a diagnosed substance use disorder increased the risk of developing a substance use disorder during adolescence. They also examined whether several factors influenced this risk such as child sex, the presence of ADHD, mood, or anxiety disorders, neighborhood location, and neighborhood income-level.
HOW WAS THIS STUDY CONDUCTED?
This study used the following administrative health-care databases in Manitoba, Canada, to create a population-based dataset for children born in Manitoba from April 1, 1984, through March 31, 2000: (1) Manitoba Health Insurance Registry; (2) Medical Services data set; (3) Hospital Abstract data set; (4) Hospital Newborn to Mother Link Registry data set; (5) Statistics Canada; (6) Manitoba Multigenerational Cohort. The research team selected all first- and second-born children to use in the population-based dataset.
The authors used (1) parental history of substance use disorder diagnosis and (2) sibling history of substance use disorder diagnosis during adolescence to predict a diagnosis of substance use disorder during adolescence. The substance use disorder diagnoses for all three groups (parent, sibling, child) were based on hospitalization or physician visit records. Adolescent SUD diagnosis was defined as having at least one hospitalization or one physician visit with a diagnosis of alcohol or drug psychoses, alcohol or drug dependence, or non-dependent abuse of drugs when the youth was between 13 and 18 years old.
The following factors were included as statistical controls in their models: mother’s age at first birth, sex, birth order, presence of an additional mental health condition (ADHD, conduct disorder, mood disorder, or anxiety disorder), geographic location of home, and income level of the neighborhood. In the models that examined the risk of diagnosis of substance use disorder during adolescence due to sibling history of substance use disorder diagnosis, the parental history of substance use disorder diagnosis was also included as a statistical control. As a form of sensitivity analysis, the authors also examined whether the child’s age when the service with parental substance use disorder occurred impacting the study findings. They used two developmental periods: (1) before the child was 5 years old or (2) when the child was between 5 and 13 years old.
Of the sample of 134,389 adolescents in the sample, about 2% had a diagnosis of substance use disorder during adolescence and 49% were male. About 10% of the total sample had a mother and 11% had a father with a history of a substance use disorder diagnosis. There were 31,307 sibling pairs included in the sample.
WHAT DID THIS STUDY FIND?
Parental substance use disorder diagnosis increased risk for substance use disorder diagnosis during adolescence.
In models that account for all included factors, children who had both parents diagnosed with a substance use disorder were 3.74 times more likely to be diagnosed with a substance use disorder during adolescence. This risk was slightly increased for female compared to male children. The risk was reduced when only one of the two parents were diagnosed. For families where the father had a diagnosis, the risk was 1.98 greater than if no parent had a diagnosis, whereas for families where the mother had a diagnosis, the risk was 2.37 greater than if no parent had a diagnosis. The child’s age at the time of parent substance use disorder diagnosis (5 or younger versus 5 or older) did not influence the risk of developing a substance use disorder during adolescence.
Having an older sibling with substance use disorder also increased risk for substance use disorder diagnosis during adolescence.
In models that account for all factors including have a parent with a substance use disorder diagnosis, less than 2% of the sample had a sibling with a substance use disorder diagnosed during adolescence. Among youth that had an older sibling with the same mother and father, their risk of a substance use disorder diagnosis during adolescence was 3.85 higher than youth whose older sibling did not have a diagnosed substance use disorder. When siblings were defined by having the same mother only, the risk remained – 2.73 times greater – albeit to a lesser degree.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This population-based study shows that family health records can be used to identify the risk of substance use disorder for adolescents. Studies like this can ultimately help health care systems understand where prevention, treatment, and recovery efforts could be targeted for at-risk youth and families.
In this study which used electronic health record data of a population-based sample ofover 100,000 youth in Canada, the risk of developing a substance use disorder during adolescence substantially increased if a parent or sibling was diagnosed with a substance use disorder. This risk was highest when both parents were diagnosed with a substance use disorder or when an older sibling was diagnosed.Yet, the findings, while significant, still leave room for a variety of other known contributing factors to developing a substance use disorder during adolescence, including, for example, adverse childhood experiences, genetic vulnerability, parenting style and monitoring, and friends and peers social influence.
Of note, the 2% prevalence of substance use disorder in this population study of Manitoba, Canada is lower than the 6-7% which is typically found in the annual USNational Survey of Drug Use and Health among 12–17-yearold’s. This could be due to the fact that rather than self-report, the substance use diagnosis in this study is dependent on youth and their families toengage in the healthcare system and have a diagnosis recorded as part of that engagement. Despite universal healthcare in Canada, there are many reasons why an adolescent might not have adiagnosis of substance use disorder in their health record although they might meet the criteria for one. For example, if substance use is not the focus of the healthcare visit, if there is a reluctance to make a substance use history part of the formal clinical record due to privacy or stigma concerns, orif there is no systemic attempt at screening, milder forms of substance usedisorders might not be identified, diagnosed, or documented. Thus, the sample of 2% in this study is likelyindicative of those youth who have severe and obvious substance use disorder.
Although the study identified the relationship between family history of substance use disorder and the risk of developing a substance use disorder during adolescence, it did not examine mechanisms of this relationship (e.g., whether the increased risk was due to genetic or environmental influences). Future research should examine the relative contribution of these different factors as well as the processes of risk in order to determine the dynamic nature of the key driving factors of increased risk.
The study did not account for treatment of family members or for history of substance use disorders prior to the birth of the child, so could be missing additional key risk factors. As well, it primarily focused on individual- and family-level characteristics but ignored additional key environmental factors (e.g., alcohol/drug availability).
Use of the electronic health record data is a strength of this study in that it provides an objective diagnosis of substance use disorder in youth and their families. Yet, these data might be missing individuals who meet substance use disorder criteria but are not screened during a healthcare encounter or if providers failed to document this in their chart due to stigma, or for other reasons.
BOTTOM LINE
In this large-scale and population-based study using electronic health records of Manitoba, Canada residents, the researchers found that the risk of developing a substance use disorder during adolescence was at least 2-3 times higher if a parent or sibling was diagnosed with a substance use disorder. While this highlights the utility of family health record data in the identification of adolescent substance use disorder risk, it’s important to remember that there are other risk factors to developing a substance use disorder during adolescence, some of which confer greater risk than the relationships reported here.
For individuals and families seeking recovery: Knowing youth’sfamily history around substance use disorders may help alert providersso they canengage in proper screening, help identify and address problematic family dynamics, and engage necessary supports for all affected family members. Youth-serving recovery programs such as recovery high schools and alternative peer groupsoften work to incorporate all family members in recovery support activities and there may be other opportunities in the clinical care setting to intervene with youth and their family members.
For treatment professionals and treatment systems: All patients enter clinical encounters with unique protective and risk factorsrelated to their potential to use substances. Knowing someone’s family history around substance use disorders may help alert providersso they canhelp to address family dynamics and engage supports for all affected family members. Some community–based programs that serve youth (e.g., recovery high schools and alternative peer groups) often provide outreach and programming for all family members in recovery support activities and there may be other opportunities in the clinical care setting to intervene with youth and their family members.
For scientists:Research is needed to better identify the mechanisms by which family history of substance use disorders increase the risk of developing a substance use disorder among offspring during adolescence and how these same factors can best be addressed in prevention and treatment programs. Studies that measure a wider array of factors related to the different sources of influence – individual, interindividual, and community – and that measure these with greater precision, are also needed to tease out these complex and intersecting relationships.
For policy makers: Family experience with substance use disorder can have repercussions on many outcomes (i.e., education/income mobility, health, mental health) for future generations. Infrastructure to support policy and programs that help to identify, prevent, and address substance use disorders and their consequences for the entire family might help break the generational impact of a substance use disorder history.