Genetic risk for substance use disorders associated with substance use transition points and symptom progression
Genetic studies often examine associations with the presence or absence of a disorder, but investigating genetic associations with transition points (e.g., age of first regular use) and symptom progression may provide a more comprehensive understanding of genetic risk for substance use disorder. Researchers in this study investigated the associations between genetic profiles with transition points and symptom progression for both alcohol and opioid use disorder.
Genetic studies investigate the extent to which genes contribute to risk for a disorder. Often, these studies examine genetic associations with the presence or absence of a disorder, rather than its progression. However, investigating genetic associations with transition points and symptom progression may provide a deeper and more comprehensive understanding of overall genetic risk for a disorder. Accordingly, researchers in this study were interested in examining the associations between polygenic risk for alcohol use disorder, opioid use disorder, and smoking trajectory with transition points and symptom progression among a treatment-seeking population.
Polygenic risk for a disorder reflects the contributions of thousands of genetic variants across the genome, each on its own accounting for a very small percentage of the risk for a given trait or disorder, but together providing information regarding genetic risk in total. This is in contrast to candidate gene studies that dominated the field during the 1990s and early 2000s. These studies searched for a single gene or polymorphism that increased risk for a disorder. While candidate gene studies are certainly useful in locating the genes responsible for single gene diseases, such as cystic fibrosis and Huntington’s disease, they are now understood to be less useful in understanding risk for complex diseases, such as substance use disorders. Complex diseases develop from a combination of polygenic and environmental influences and are studied using both twin studies and molecular genetic studies.
Twin and family studies, which estimate heritability based on correlations between pairs of relatives, have consistently demonstrated that genetic risk factors for substance use disorders account for approximately 50%, with the other 50% being accounted for by environmental factors. Molecular genetic studies, which aim to identify the genetic variants that account for this heritability, currently demonstrate that polygenic risk only accounts for 1-3% of the variance, but have still been able to predict risk for substance use problems. The apparent discrepancy arises because twin studies estimate broad heritability, encompassing all genetic influences, including rare variants, and gene-gene interactions. Molecular genetic studies, on the other hand, seek to uncover more identifiable specific genetic markers associated with a trait, often capturing only a small fraction of the variation in the occurrence of the disorder. Together, twin studies and molecular genetic studies provide complementary information about the genetic basis of substance use disorders. Twin studies estimate overall heritability, while molecular genetic studies identify specific genetic markers with small effect sizes. The polygenic nature of many complex traits reconciles these findings, highlighting the need for both approaches to gain a comprehensive understanding of the genetic contribution of complex disorders such as substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team investigated the associations between polygenic risk scores for substance use disorders with 4 substance use transition points and 2 progression symptoms. Polygenic risk scores are calculated from discovery samples of genome-wide association studies (GWAS) and then used to predict outcomes in an independent target sample.
The discovery samples used to calculate the polygenic risk scores in this study consisted of 3 genome-wide association studies of alcohol use disorder, opioid use disorder, and smoking trajectory (i.e., characterizing the path from first time smoking to regular smoking to potential dependence), with approximately 300,000 – 400,000 participants in each. Participants for the target sample were recruited for studies of the genetics of addiction from inpatient and outpatient settings, although there was not much more detail provided regarding the recruitment settings. Control participants without a substance use disorder were recruited from other medical facilities and advertisements.
The researchers were interested in the outcomes of substance use transition points and progression symptoms among participants with alcohol use disorder, opioid use disorder, and smoking trajectory. The 4 transition points included age of first substance use, regular use (not defined in the current study but often indicating weekly or more frequent use), reporting problems to a healthcare professional, and a DSM-IV substance dependence diagnosis (generally consistent with moderate/severe substance use disorder in the DSM-5). The 2 progression symptoms included progression from regular use to onset of problems and progression from regular use to a dependence diagnosis. These outcomes were assessed by the Semi-Structured Assessment for Drug Dependence and Alcoholism, which was administered by a trained interviewer.
In total, the study included 5692 participants of European ancestry and 4918 participants of African ancestry. Within the European sample, approximately 44% were women. Within the African sample, approximately 45% were women.
The researchers conducted the analyses separately for those of European ancestry and African ancestry. Of note, it is especially important to include non-European populations in genetic studies, given that 78% of these studies have currently been conducted with European populations. They first tested the associations between the polygenic risk scores with the substance use transition points and progression symptoms within each population, for which sex was included as a covariate. Then, they stratified the analyses by sex and age of first regular use (younger than 18 vs. 18 or older) to test other potential demographic differences.
WHAT DID THIS STUDY FIND?
For those of European ancestry, a higher risk score was associated with substance use transition points and alcohol-related progression symptoms.
Higher polygenic risk for alcohol use disorder, opioid use disorder, and smoking was associated with earlier onset to all 4 transition points: age of first substance use, regular use, reporting problems to a healthcare professional, and a dependence diagnosis. Higher polygenic risk for alcohol use disorder was also associated with the 2 progression symptoms of time from regular use to onset of problems and time from regular use to a dependence diagnosis. However, polygenic risk for opioid use disorder and smoking was not associated with progression symptoms.
When the analyses were stratified by sex, polygenic risk for alcohol use disorder showed a stronger association with alcohol-related transition points among women than men. Further, polygenic risk for alcohol use disorder was a stronger predictor of alcohol-related problems being raised with a health professional among women, but showed a stronger association with the progression from regular use to problems among men. Polygenic risk for smoking was associated with the progression from regular use to a dependence diagnosis only in women.
When the analyses were stratified by age of first regular use (< 18 vs. 18+), higher polygenic risk for alcohol use disorder was associated with progression to onset of problems and a dependence diagnosis, regardless of age of first regular use.
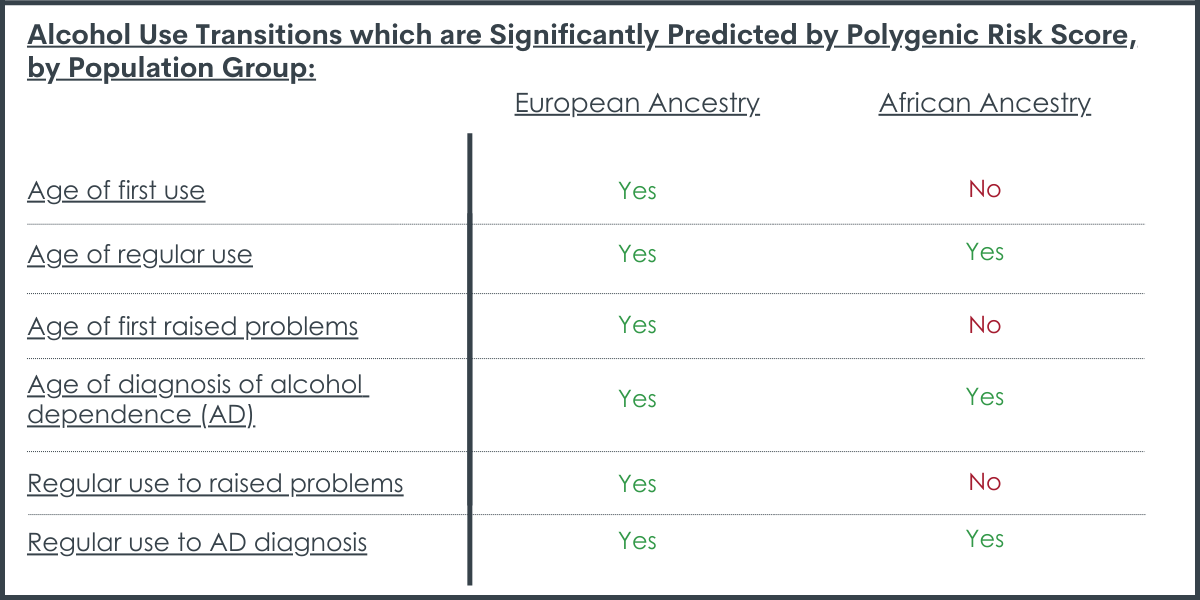
Among those of African ancestry, higher risk scores were associated with select substance use transition points and progression symptoms within specific populations.
Polygenic risk for alcohol use disorder was associated with age of regular alcohol use and dependence diagnosis, as well as progression from regular use to a dependence diagnosis. Polygenic risk for opioid use disorder was not associated with any of transition points or progression symptoms. Polygenic risk for smoking was associated with age of first use only, and neither of progression symptoms.
When the analyses were stratified by sex, polygenic risk for alcohol use disorder was only associated with the transition point of a dependence diagnosis, with a slightly stronger association between risk score and diagnosis among women. Polygenic risk for opioid use disorder was associated with onset of use among women only, while polygenic risk for smoking was associated with onset of use among men only.
When the analyses were stratified by age of first regular use (< 18 vs. 18+), higher polygenic risk for alcohol use disorder was associated with progression to a dependence diagnosis only among those who began drinking when they were older than 18 years old.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study investigated the associations between polygenic risk scores for substance use disorders with substance use transition points and progression symptoms.
Overall, results showed that polygenic risk for substance use disorders appears to be associated with transition points and progression symptoms among those of European ancestry and, to a lesser extent, those of African ancestry. However, polygenic risk contributed minimally, accounting for less than 3% of the variance.
One possible explanation for fewer associations among those of African ancestry is that there was lower ability to detect effects because of smaller discovery samples. This speaks to the larger problem regarding a lack of adequate data from non-European populations, since the majority of genomic studies have been conducted with European populations. The lack of diversity in genomic studies further contributes to the broader problem of health disparities and underscores the need to include non-European populations in genomic and health studies.
The findings showing that the polygenic risk scores account for less than 3% of the total variance in substance use transition points and progression symptoms are entirely consistent with other studies demonstrating that polygenic risk only accounts for 1-3% of the variance in substance use-related traits. This reflects that much of the heritability for substance use disorder demonstrated by twin studies has not yet been captured in molecular studies.
However, both types of studies are critically important for demonstrating the modest role of genetics in risk for substance use disorders, which are not currently modifiable, and the large role of the environment, which has the potential to be modified by prevention and early intervention efforts.
Beyond this high-level implication, the clinical utility of polygenic risk scores for informing treatment and identifying individuals at an increased risk remains limited, despite growing interest.
A recent review identified 4 bottlenecks to translating genetic studies of psychiatric disorders like this one into practice and suggested some potential solutions. These include a focus on family history rather than overreliance on molecular genetic studies (e.g., the number of first-degree relatives with substance use disorder) and a call for researchers to conduct more experimental studies addressing the translation of psychiatric genetic studies rather than reviews. These experiments may, for instance, examine whether providing information about genetic risk to individuals influences their behavior or whether particular genetic markers influence one’s response to therapy or medication.
The study was conducted only among those of European and African ancestry. Thus, results may not generalize to individuals with other ancestral backgrounds.
Similarly, the study was conducted with treatment-seeking populations from 5 treatment centers in the eastern United States over 20 years. Results may not generalize to people who are not seeking treatment or from other parts of the United States.
The discovery samples used to create the polygenic risk scores were from a sample that predominately consisted of men. This suggests the results may be biased towards men and reduces the reliability for which they can be interpreted among women.
Effect sizes were very small, accounting for less than 3% of the total variance in substance use transition points and progression symptoms.
The alcohol and opioid use disorder outcomes were based on the criteria outlined in the 4th edition of the Diagnostic and Statistical Manual, while the smoking outcome was based on trajectories. Therefore, there may be more variability within this trajectory outcome than the disorder categories, which can diminish the associations with the polygenic risk scores.
BOTTOM LINE
Polygenic risk for substance use disorders is associated with substance use transition points and progression symptoms, but explains small proportions of these markers of substance use risks, accounting for less than 3% of the variance. While twin studies suggest that this percentage may be closer to 50%, both types of studies are critically important for demonstrating that environmental factors are at least as influential, which have the potential to be modified by prevention and early intervention efforts.
For individuals and families seeking recovery: This study showed that risk for markers of risky alcohol use and alcohol use disorders is predicted by genetics, but to a relatively modest degree. The findings here suggest that environmental factors play a large role. This knowledge can empower individuals to make informed decisions regarding substance use if they have a family history, which reflects both genetic and environmental factors. Importantly, environmental factors can increase risk but may also be protective.
For treatment professionals and treatment systems: This study demonstrated that polygenic risk for substance use disorders appears to be at least minimally associated with substance use transition points and progression symptoms. While the clinical utility of polygenic risk scores is currently limited, these findings, coupled with findings from twin studies, suggest that family history is an important risk factor for substance use disorders. Family history, however, likely reflects a complex interplay of both genetic and environmental factors. Accordingly, treatment professionals who consider family history when evaluating and treating individuals with substance use disorders are likely to gain a more comprehensive understanding of the person’s risk and protective factors.
For scientists: Because genetic studies have historically focused on individuals of European ancestry, future genetic and health research that includes individuals with non-European ancestries will help to increase diversity in these studies, thereby potentially reducing health disparities. Additionally, research that examines the clinical utility and how polygenic research can be translated into practice and policy can help to address some of the bottlenecks to effective translation.
For policy makers: Results from this study, and other findings from the field of psychiatric genetics, consistently demonstrate that genetic risk factors, which cannot be modified at this time, play only a modest role in risk for the development of substance use disorders, indicating that they are biologically influenced, but not biologically determined. Conversely, environmental factors, which can be modified, appear to play a much larger role. Accordingly, policy makers who support policies that promote prevention and early intervention efforts may contribute to protective environmental factors and community-level policies (e.g., regulating the number of alcohol outlets in a given area) that reduce risk for substance use disorders and other types of hazardous substance use. Additionally, given that the majority of genetic studies have been conducted with European populations, funding for research that includes non-European populations can help to reduce existing health disparities.
Genetic studies investigate the extent to which genes contribute to risk for a disorder. Often, these studies examine genetic associations with the presence or absence of a disorder, rather than its progression. However, investigating genetic associations with transition points and symptom progression may provide a deeper and more comprehensive understanding of overall genetic risk for a disorder. Accordingly, researchers in this study were interested in examining the associations between polygenic risk for alcohol use disorder, opioid use disorder, and smoking trajectory with transition points and symptom progression among a treatment-seeking population.
Polygenic risk for a disorder reflects the contributions of thousands of genetic variants across the genome, each on its own accounting for a very small percentage of the risk for a given trait or disorder, but together providing information regarding genetic risk in total. This is in contrast to candidate gene studies that dominated the field during the 1990s and early 2000s. These studies searched for a single gene or polymorphism that increased risk for a disorder. While candidate gene studies are certainly useful in locating the genes responsible for single gene diseases, such as cystic fibrosis and Huntington’s disease, they are now understood to be less useful in understanding risk for complex diseases, such as substance use disorders. Complex diseases develop from a combination of polygenic and environmental influences and are studied using both twin studies and molecular genetic studies.
Twin and family studies, which estimate heritability based on correlations between pairs of relatives, have consistently demonstrated that genetic risk factors for substance use disorders account for approximately 50%, with the other 50% being accounted for by environmental factors. Molecular genetic studies, which aim to identify the genetic variants that account for this heritability, currently demonstrate that polygenic risk only accounts for 1-3% of the variance, but have still been able to predict risk for substance use problems. The apparent discrepancy arises because twin studies estimate broad heritability, encompassing all genetic influences, including rare variants, and gene-gene interactions. Molecular genetic studies, on the other hand, seek to uncover more identifiable specific genetic markers associated with a trait, often capturing only a small fraction of the variation in the occurrence of the disorder. Together, twin studies and molecular genetic studies provide complementary information about the genetic basis of substance use disorders. Twin studies estimate overall heritability, while molecular genetic studies identify specific genetic markers with small effect sizes. The polygenic nature of many complex traits reconciles these findings, highlighting the need for both approaches to gain a comprehensive understanding of the genetic contribution of complex disorders such as substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team investigated the associations between polygenic risk scores for substance use disorders with 4 substance use transition points and 2 progression symptoms. Polygenic risk scores are calculated from discovery samples of genome-wide association studies (GWAS) and then used to predict outcomes in an independent target sample.
The discovery samples used to calculate the polygenic risk scores in this study consisted of 3 genome-wide association studies of alcohol use disorder, opioid use disorder, and smoking trajectory (i.e., characterizing the path from first time smoking to regular smoking to potential dependence), with approximately 300,000 – 400,000 participants in each. Participants for the target sample were recruited for studies of the genetics of addiction from inpatient and outpatient settings, although there was not much more detail provided regarding the recruitment settings. Control participants without a substance use disorder were recruited from other medical facilities and advertisements.
The researchers were interested in the outcomes of substance use transition points and progression symptoms among participants with alcohol use disorder, opioid use disorder, and smoking trajectory. The 4 transition points included age of first substance use, regular use (not defined in the current study but often indicating weekly or more frequent use), reporting problems to a healthcare professional, and a DSM-IV substance dependence diagnosis (generally consistent with moderate/severe substance use disorder in the DSM-5). The 2 progression symptoms included progression from regular use to onset of problems and progression from regular use to a dependence diagnosis. These outcomes were assessed by the Semi-Structured Assessment for Drug Dependence and Alcoholism, which was administered by a trained interviewer.
In total, the study included 5692 participants of European ancestry and 4918 participants of African ancestry. Within the European sample, approximately 44% were women. Within the African sample, approximately 45% were women.
The researchers conducted the analyses separately for those of European ancestry and African ancestry. Of note, it is especially important to include non-European populations in genetic studies, given that 78% of these studies have currently been conducted with European populations. They first tested the associations between the polygenic risk scores with the substance use transition points and progression symptoms within each population, for which sex was included as a covariate. Then, they stratified the analyses by sex and age of first regular use (younger than 18 vs. 18 or older) to test other potential demographic differences.
WHAT DID THIS STUDY FIND?
For those of European ancestry, a higher risk score was associated with substance use transition points and alcohol-related progression symptoms.
Higher polygenic risk for alcohol use disorder, opioid use disorder, and smoking was associated with earlier onset to all 4 transition points: age of first substance use, regular use, reporting problems to a healthcare professional, and a dependence diagnosis. Higher polygenic risk for alcohol use disorder was also associated with the 2 progression symptoms of time from regular use to onset of problems and time from regular use to a dependence diagnosis. However, polygenic risk for opioid use disorder and smoking was not associated with progression symptoms.
When the analyses were stratified by sex, polygenic risk for alcohol use disorder showed a stronger association with alcohol-related transition points among women than men. Further, polygenic risk for alcohol use disorder was a stronger predictor of alcohol-related problems being raised with a health professional among women, but showed a stronger association with the progression from regular use to problems among men. Polygenic risk for smoking was associated with the progression from regular use to a dependence diagnosis only in women.
When the analyses were stratified by age of first regular use (< 18 vs. 18+), higher polygenic risk for alcohol use disorder was associated with progression to onset of problems and a dependence diagnosis, regardless of age of first regular use.
Among those of African ancestry, higher risk scores were associated with select substance use transition points and progression symptoms within specific populations.
Polygenic risk for alcohol use disorder was associated with age of regular alcohol use and dependence diagnosis, as well as progression from regular use to a dependence diagnosis. Polygenic risk for opioid use disorder was not associated with any of transition points or progression symptoms. Polygenic risk for smoking was associated with age of first use only, and neither of progression symptoms.
When the analyses were stratified by sex, polygenic risk for alcohol use disorder was only associated with the transition point of a dependence diagnosis, with a slightly stronger association between risk score and diagnosis among women. Polygenic risk for opioid use disorder was associated with onset of use among women only, while polygenic risk for smoking was associated with onset of use among men only.
When the analyses were stratified by age of first regular use (< 18 vs. 18+), higher polygenic risk for alcohol use disorder was associated with progression to a dependence diagnosis only among those who began drinking when they were older than 18 years old.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study investigated the associations between polygenic risk scores for substance use disorders with substance use transition points and progression symptoms.
Overall, results showed that polygenic risk for substance use disorders appears to be associated with transition points and progression symptoms among those of European ancestry and, to a lesser extent, those of African ancestry. However, polygenic risk contributed minimally, accounting for less than 3% of the variance.
One possible explanation for fewer associations among those of African ancestry is that there was lower ability to detect effects because of smaller discovery samples. This speaks to the larger problem regarding a lack of adequate data from non-European populations, since the majority of genomic studies have been conducted with European populations. The lack of diversity in genomic studies further contributes to the broader problem of health disparities and underscores the need to include non-European populations in genomic and health studies.
The findings showing that the polygenic risk scores account for less than 3% of the total variance in substance use transition points and progression symptoms are entirely consistent with other studies demonstrating that polygenic risk only accounts for 1-3% of the variance in substance use-related traits. This reflects that much of the heritability for substance use disorder demonstrated by twin studies has not yet been captured in molecular studies.
However, both types of studies are critically important for demonstrating the modest role of genetics in risk for substance use disorders, which are not currently modifiable, and the large role of the environment, which has the potential to be modified by prevention and early intervention efforts.
Beyond this high-level implication, the clinical utility of polygenic risk scores for informing treatment and identifying individuals at an increased risk remains limited, despite growing interest.
A recent review identified 4 bottlenecks to translating genetic studies of psychiatric disorders like this one into practice and suggested some potential solutions. These include a focus on family history rather than overreliance on molecular genetic studies (e.g., the number of first-degree relatives with substance use disorder) and a call for researchers to conduct more experimental studies addressing the translation of psychiatric genetic studies rather than reviews. These experiments may, for instance, examine whether providing information about genetic risk to individuals influences their behavior or whether particular genetic markers influence one’s response to therapy or medication.
The study was conducted only among those of European and African ancestry. Thus, results may not generalize to individuals with other ancestral backgrounds.
Similarly, the study was conducted with treatment-seeking populations from 5 treatment centers in the eastern United States over 20 years. Results may not generalize to people who are not seeking treatment or from other parts of the United States.
The discovery samples used to create the polygenic risk scores were from a sample that predominately consisted of men. This suggests the results may be biased towards men and reduces the reliability for which they can be interpreted among women.
Effect sizes were very small, accounting for less than 3% of the total variance in substance use transition points and progression symptoms.
The alcohol and opioid use disorder outcomes were based on the criteria outlined in the 4th edition of the Diagnostic and Statistical Manual, while the smoking outcome was based on trajectories. Therefore, there may be more variability within this trajectory outcome than the disorder categories, which can diminish the associations with the polygenic risk scores.
BOTTOM LINE
Polygenic risk for substance use disorders is associated with substance use transition points and progression symptoms, but explains small proportions of these markers of substance use risks, accounting for less than 3% of the variance. While twin studies suggest that this percentage may be closer to 50%, both types of studies are critically important for demonstrating that environmental factors are at least as influential, which have the potential to be modified by prevention and early intervention efforts.
For individuals and families seeking recovery: This study showed that risk for markers of risky alcohol use and alcohol use disorders is predicted by genetics, but to a relatively modest degree. The findings here suggest that environmental factors play a large role. This knowledge can empower individuals to make informed decisions regarding substance use if they have a family history, which reflects both genetic and environmental factors. Importantly, environmental factors can increase risk but may also be protective.
For treatment professionals and treatment systems: This study demonstrated that polygenic risk for substance use disorders appears to be at least minimally associated with substance use transition points and progression symptoms. While the clinical utility of polygenic risk scores is currently limited, these findings, coupled with findings from twin studies, suggest that family history is an important risk factor for substance use disorders. Family history, however, likely reflects a complex interplay of both genetic and environmental factors. Accordingly, treatment professionals who consider family history when evaluating and treating individuals with substance use disorders are likely to gain a more comprehensive understanding of the person’s risk and protective factors.
For scientists: Because genetic studies have historically focused on individuals of European ancestry, future genetic and health research that includes individuals with non-European ancestries will help to increase diversity in these studies, thereby potentially reducing health disparities. Additionally, research that examines the clinical utility and how polygenic research can be translated into practice and policy can help to address some of the bottlenecks to effective translation.
For policy makers: Results from this study, and other findings from the field of psychiatric genetics, consistently demonstrate that genetic risk factors, which cannot be modified at this time, play only a modest role in risk for the development of substance use disorders, indicating that they are biologically influenced, but not biologically determined. Conversely, environmental factors, which can be modified, appear to play a much larger role. Accordingly, policy makers who support policies that promote prevention and early intervention efforts may contribute to protective environmental factors and community-level policies (e.g., regulating the number of alcohol outlets in a given area) that reduce risk for substance use disorders and other types of hazardous substance use. Additionally, given that the majority of genetic studies have been conducted with European populations, funding for research that includes non-European populations can help to reduce existing health disparities.
Genetic studies investigate the extent to which genes contribute to risk for a disorder. Often, these studies examine genetic associations with the presence or absence of a disorder, rather than its progression. However, investigating genetic associations with transition points and symptom progression may provide a deeper and more comprehensive understanding of overall genetic risk for a disorder. Accordingly, researchers in this study were interested in examining the associations between polygenic risk for alcohol use disorder, opioid use disorder, and smoking trajectory with transition points and symptom progression among a treatment-seeking population.
Polygenic risk for a disorder reflects the contributions of thousands of genetic variants across the genome, each on its own accounting for a very small percentage of the risk for a given trait or disorder, but together providing information regarding genetic risk in total. This is in contrast to candidate gene studies that dominated the field during the 1990s and early 2000s. These studies searched for a single gene or polymorphism that increased risk for a disorder. While candidate gene studies are certainly useful in locating the genes responsible for single gene diseases, such as cystic fibrosis and Huntington’s disease, they are now understood to be less useful in understanding risk for complex diseases, such as substance use disorders. Complex diseases develop from a combination of polygenic and environmental influences and are studied using both twin studies and molecular genetic studies.
Twin and family studies, which estimate heritability based on correlations between pairs of relatives, have consistently demonstrated that genetic risk factors for substance use disorders account for approximately 50%, with the other 50% being accounted for by environmental factors. Molecular genetic studies, which aim to identify the genetic variants that account for this heritability, currently demonstrate that polygenic risk only accounts for 1-3% of the variance, but have still been able to predict risk for substance use problems. The apparent discrepancy arises because twin studies estimate broad heritability, encompassing all genetic influences, including rare variants, and gene-gene interactions. Molecular genetic studies, on the other hand, seek to uncover more identifiable specific genetic markers associated with a trait, often capturing only a small fraction of the variation in the occurrence of the disorder. Together, twin studies and molecular genetic studies provide complementary information about the genetic basis of substance use disorders. Twin studies estimate overall heritability, while molecular genetic studies identify specific genetic markers with small effect sizes. The polygenic nature of many complex traits reconciles these findings, highlighting the need for both approaches to gain a comprehensive understanding of the genetic contribution of complex disorders such as substance use disorder.
HOW WAS THIS STUDY CONDUCTED?
The research team investigated the associations between polygenic risk scores for substance use disorders with 4 substance use transition points and 2 progression symptoms. Polygenic risk scores are calculated from discovery samples of genome-wide association studies (GWAS) and then used to predict outcomes in an independent target sample.
The discovery samples used to calculate the polygenic risk scores in this study consisted of 3 genome-wide association studies of alcohol use disorder, opioid use disorder, and smoking trajectory (i.e., characterizing the path from first time smoking to regular smoking to potential dependence), with approximately 300,000 – 400,000 participants in each. Participants for the target sample were recruited for studies of the genetics of addiction from inpatient and outpatient settings, although there was not much more detail provided regarding the recruitment settings. Control participants without a substance use disorder were recruited from other medical facilities and advertisements.
The researchers were interested in the outcomes of substance use transition points and progression symptoms among participants with alcohol use disorder, opioid use disorder, and smoking trajectory. The 4 transition points included age of first substance use, regular use (not defined in the current study but often indicating weekly or more frequent use), reporting problems to a healthcare professional, and a DSM-IV substance dependence diagnosis (generally consistent with moderate/severe substance use disorder in the DSM-5). The 2 progression symptoms included progression from regular use to onset of problems and progression from regular use to a dependence diagnosis. These outcomes were assessed by the Semi-Structured Assessment for Drug Dependence and Alcoholism, which was administered by a trained interviewer.
In total, the study included 5692 participants of European ancestry and 4918 participants of African ancestry. Within the European sample, approximately 44% were women. Within the African sample, approximately 45% were women.
The researchers conducted the analyses separately for those of European ancestry and African ancestry. Of note, it is especially important to include non-European populations in genetic studies, given that 78% of these studies have currently been conducted with European populations. They first tested the associations between the polygenic risk scores with the substance use transition points and progression symptoms within each population, for which sex was included as a covariate. Then, they stratified the analyses by sex and age of first regular use (younger than 18 vs. 18 or older) to test other potential demographic differences.
WHAT DID THIS STUDY FIND?
For those of European ancestry, a higher risk score was associated with substance use transition points and alcohol-related progression symptoms.
Higher polygenic risk for alcohol use disorder, opioid use disorder, and smoking was associated with earlier onset to all 4 transition points: age of first substance use, regular use, reporting problems to a healthcare professional, and a dependence diagnosis. Higher polygenic risk for alcohol use disorder was also associated with the 2 progression symptoms of time from regular use to onset of problems and time from regular use to a dependence diagnosis. However, polygenic risk for opioid use disorder and smoking was not associated with progression symptoms.
When the analyses were stratified by sex, polygenic risk for alcohol use disorder showed a stronger association with alcohol-related transition points among women than men. Further, polygenic risk for alcohol use disorder was a stronger predictor of alcohol-related problems being raised with a health professional among women, but showed a stronger association with the progression from regular use to problems among men. Polygenic risk for smoking was associated with the progression from regular use to a dependence diagnosis only in women.
When the analyses were stratified by age of first regular use (< 18 vs. 18+), higher polygenic risk for alcohol use disorder was associated with progression to onset of problems and a dependence diagnosis, regardless of age of first regular use.
Among those of African ancestry, higher risk scores were associated with select substance use transition points and progression symptoms within specific populations.
Polygenic risk for alcohol use disorder was associated with age of regular alcohol use and dependence diagnosis, as well as progression from regular use to a dependence diagnosis. Polygenic risk for opioid use disorder was not associated with any of transition points or progression symptoms. Polygenic risk for smoking was associated with age of first use only, and neither of progression symptoms.
When the analyses were stratified by sex, polygenic risk for alcohol use disorder was only associated with the transition point of a dependence diagnosis, with a slightly stronger association between risk score and diagnosis among women. Polygenic risk for opioid use disorder was associated with onset of use among women only, while polygenic risk for smoking was associated with onset of use among men only.
When the analyses were stratified by age of first regular use (< 18 vs. 18+), higher polygenic risk for alcohol use disorder was associated with progression to a dependence diagnosis only among those who began drinking when they were older than 18 years old.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study investigated the associations between polygenic risk scores for substance use disorders with substance use transition points and progression symptoms.
Overall, results showed that polygenic risk for substance use disorders appears to be associated with transition points and progression symptoms among those of European ancestry and, to a lesser extent, those of African ancestry. However, polygenic risk contributed minimally, accounting for less than 3% of the variance.
One possible explanation for fewer associations among those of African ancestry is that there was lower ability to detect effects because of smaller discovery samples. This speaks to the larger problem regarding a lack of adequate data from non-European populations, since the majority of genomic studies have been conducted with European populations. The lack of diversity in genomic studies further contributes to the broader problem of health disparities and underscores the need to include non-European populations in genomic and health studies.
The findings showing that the polygenic risk scores account for less than 3% of the total variance in substance use transition points and progression symptoms are entirely consistent with other studies demonstrating that polygenic risk only accounts for 1-3% of the variance in substance use-related traits. This reflects that much of the heritability for substance use disorder demonstrated by twin studies has not yet been captured in molecular studies.
However, both types of studies are critically important for demonstrating the modest role of genetics in risk for substance use disorders, which are not currently modifiable, and the large role of the environment, which has the potential to be modified by prevention and early intervention efforts.
Beyond this high-level implication, the clinical utility of polygenic risk scores for informing treatment and identifying individuals at an increased risk remains limited, despite growing interest.
A recent review identified 4 bottlenecks to translating genetic studies of psychiatric disorders like this one into practice and suggested some potential solutions. These include a focus on family history rather than overreliance on molecular genetic studies (e.g., the number of first-degree relatives with substance use disorder) and a call for researchers to conduct more experimental studies addressing the translation of psychiatric genetic studies rather than reviews. These experiments may, for instance, examine whether providing information about genetic risk to individuals influences their behavior or whether particular genetic markers influence one’s response to therapy or medication.
The study was conducted only among those of European and African ancestry. Thus, results may not generalize to individuals with other ancestral backgrounds.
Similarly, the study was conducted with treatment-seeking populations from 5 treatment centers in the eastern United States over 20 years. Results may not generalize to people who are not seeking treatment or from other parts of the United States.
The discovery samples used to create the polygenic risk scores were from a sample that predominately consisted of men. This suggests the results may be biased towards men and reduces the reliability for which they can be interpreted among women.
Effect sizes were very small, accounting for less than 3% of the total variance in substance use transition points and progression symptoms.
The alcohol and opioid use disorder outcomes were based on the criteria outlined in the 4th edition of the Diagnostic and Statistical Manual, while the smoking outcome was based on trajectories. Therefore, there may be more variability within this trajectory outcome than the disorder categories, which can diminish the associations with the polygenic risk scores.
BOTTOM LINE
Polygenic risk for substance use disorders is associated with substance use transition points and progression symptoms, but explains small proportions of these markers of substance use risks, accounting for less than 3% of the variance. While twin studies suggest that this percentage may be closer to 50%, both types of studies are critically important for demonstrating that environmental factors are at least as influential, which have the potential to be modified by prevention and early intervention efforts.
For individuals and families seeking recovery: This study showed that risk for markers of risky alcohol use and alcohol use disorders is predicted by genetics, but to a relatively modest degree. The findings here suggest that environmental factors play a large role. This knowledge can empower individuals to make informed decisions regarding substance use if they have a family history, which reflects both genetic and environmental factors. Importantly, environmental factors can increase risk but may also be protective.
For treatment professionals and treatment systems: This study demonstrated that polygenic risk for substance use disorders appears to be at least minimally associated with substance use transition points and progression symptoms. While the clinical utility of polygenic risk scores is currently limited, these findings, coupled with findings from twin studies, suggest that family history is an important risk factor for substance use disorders. Family history, however, likely reflects a complex interplay of both genetic and environmental factors. Accordingly, treatment professionals who consider family history when evaluating and treating individuals with substance use disorders are likely to gain a more comprehensive understanding of the person’s risk and protective factors.
For scientists: Because genetic studies have historically focused on individuals of European ancestry, future genetic and health research that includes individuals with non-European ancestries will help to increase diversity in these studies, thereby potentially reducing health disparities. Additionally, research that examines the clinical utility and how polygenic research can be translated into practice and policy can help to address some of the bottlenecks to effective translation.
For policy makers: Results from this study, and other findings from the field of psychiatric genetics, consistently demonstrate that genetic risk factors, which cannot be modified at this time, play only a modest role in risk for the development of substance use disorders, indicating that they are biologically influenced, but not biologically determined. Conversely, environmental factors, which can be modified, appear to play a much larger role. Accordingly, policy makers who support policies that promote prevention and early intervention efforts may contribute to protective environmental factors and community-level policies (e.g., regulating the number of alcohol outlets in a given area) that reduce risk for substance use disorders and other types of hazardous substance use. Additionally, given that the majority of genetic studies have been conducted with European populations, funding for research that includes non-European populations can help to reduce existing health disparities.