A computerized training to inhibit desire for alcohol added benefit to residential treatment
Compared with lower risk drinking, alcohol use disorder may result, in part, from greater difficulty suppressing automatic responses (i.e., inhibitory control) to a desire for alcohol. Strategies that improve control over these automatic responses may improve treatment and recovery outcomes. This study tested computerized inhibition training interventions on drinking outcomes for individuals with alcohol use disorder attending residential treatment.
Computerized inhibition training interventions have been developed with these goals in mind. In such trainings, participants are instructed to press a button in response to stimuli (i.e., a “go” cue), unless a “no go” cue is presented, in which case they would be required to suppress their natural response to press the button. These trainings can be specific to alcohol, where alcohol-related pictures are consistently paired with “no go” cues, or they can be non-specific and paired with other types of pictures, such as water beverages or neutral stimuli.
The ratio of “go” trials to “no go” trials can also vary. To date, most studies investigating the effects of alcohol-specific inhibition trainings have used half “go” trials and half “no go” trials. However, it may be that more challenging trainings could produce greater improvements on one’s ability to inhibit automatic responses toward alcohol thereby improving alcohol use outcomes.
The reasons why alcohol-specific inhibition trainings may work are unclear, but 2 hypotheses have been proposed. The inhibitory control hypothesis suggests that the trainings work by enhancing someone’s ability to suppress automatic responses that make individuals more likely to choose to drink alcohol. The stimulus devaluation hypothesis suggests the trainings work by decreasing someone’s positive associations with alcohol use resulting from consistently pairing the stimulus with the “no go” cue. In other words, requiring someone to suppress an automatic pull toward alcohol may help them begin to associate alcohol with negative rather than positive attributes.
Researchers in this study compared the effects of a standard alcohol-specific inhibition training that used a 50/50 ratio of “go” to “no go” trials vs. an improved alcohol-specific inhibition training that used a more challenging ratio of “go” to “no-go” trials (75/25) vs. a control inhibition training that was not specific to alcohol. They also sought to investigate how the trainings worked if they were shown to be helpful. This research can help shed light on the benefits of inhibition trainings on treatment outcomes and help uncover potential mechanisms of action.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial comparing 2 alcohol-specific inhibition training interventions and a control training condition administered during residential treatment on drinking outcomes 3 months after treatment discharge in adults with alcohol use disorder. Potential working mechanisms were also assessed.
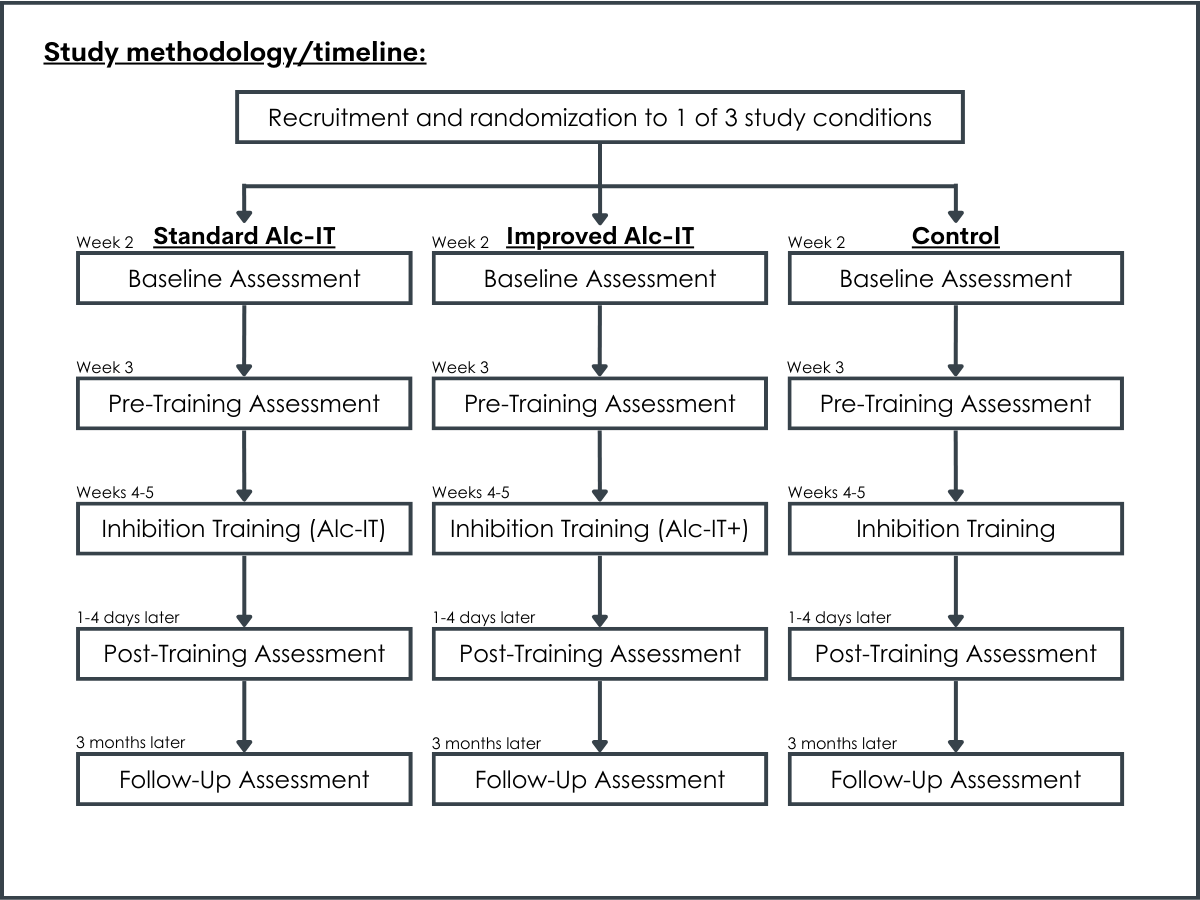
Participants were recruited during admission to the treatment program and, if eligible and willing to participate in the study, were administered baseline assessments during their second week of treatment. This baseline assessment consisted of questionnaires and a calendar-based assessment where they were asked to report their daily alcohol consumption during the previous 90 days.
During the third week of treatment, participants were administered a pre-training assessment, which consisted of questionnaires and completion of experimental tasks assessing inhibitory control. During the fourth and fifth weeks of treatment, participants completed the 6 sessions of inhibition training. Finally, 1-4 days after the last training session, participants were administered a post-training assessment, in which they repeated the questionnaires and experimental tasks that were completed during the pre-training assessment. Participants then finished their 8- to 12-week inpatient stays. After discharge, participants were followed up with at 3, 6, and 12 months. However, the researchers chose to focus on the 3-month follow-up because this time period is an especially sensitive one for potential relapse and training effects are likely to be more salient since it is closer to when the trainings occurred.
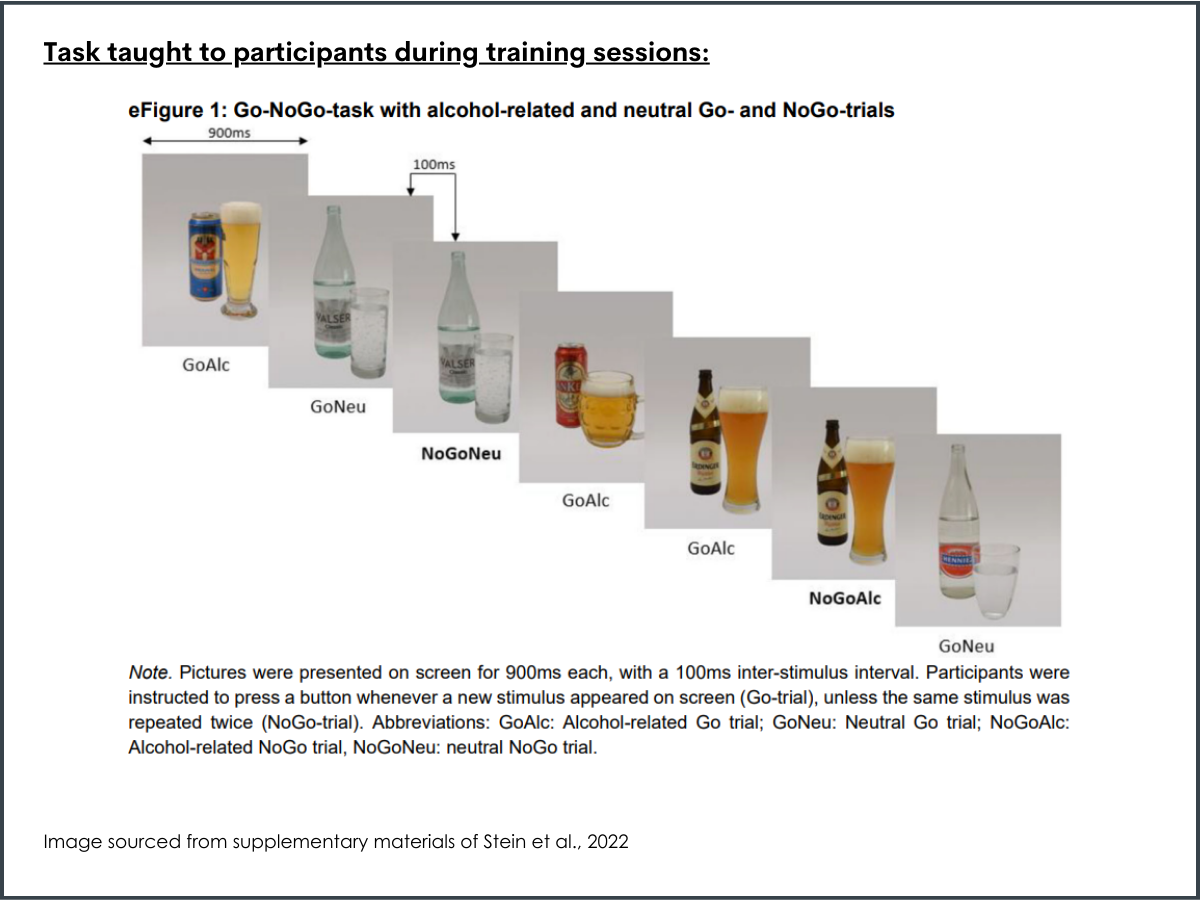
Participants were randomized into 3 training conditions, in which they were asked to complete different versions of a modified inhibitory task, called the Go/No Go Task, as an add-on to their residential treatment program. In all 3 training conditions, participants were presented with 320 trials. Eighty of these trials included pictures of alcoholic beverages that were tailored to the participant’s drink of choice (i.e., beer, wine, or spirits), 80 included pictures of water beverages, and 160 included pictures of neutral objects. Participants were instructed to press a button when the “go” cue appeared, but to withhold or inhibit their response when a “no go” cue appeared. The ”no go” cue in all trials was when the same picture was repeated twice.
The 2 training interventions included a standard inhibition training and an “improved” inhibition training. In the standard training, the ratio of “go” and “no go” trials was 50/50, whereas in the improved more challenging training, the ratio was 75/25.
The hypothesis was that, because there were more instances where participants pressed a button in response to the non-alcohol cue (“go”) it would be harder for them to inhibit this automatic response – i.e., not press the button – when an alcohol cue was on the screen (“no go”). Both training interventions were alcohol-specific, meaning that pictures of alcoholic beverages were consistently paired with a “no go” cue, which requires participants to inhibit automatic responses related to alcohol. In the “go” cues, however, the water and neutral pictures were distributed across them. In the control condition, alcohol, water, and neutral picture types were distributed evenly across the “go” and “no go” trials.
The researchers were primarily interested in the outcome of the percentage of days abstinent from alcohol at the 3-month follow-up, as assessed by the Timeline Follow-Back Interview. The interview was conducted during the baseline assessment, which asked about participants’ daily alcohol consumption during the 90 days prior to entering treatment, and the 3-month follow-up assessment, which asked about participants daily alcohol consumption during the 90 days after being discharged from treatment.
The researchers were also interested in the percentage of heavy drinking days (defined as 4+ drinks in a day for women and 5+ for men) at the 3-month follow-up assessment and the number of days until participants had their first drink, as well as potential working mechanisms, which included inhibitory control and stimulus devaluation. Inhibitory control was measured by the number of alcohol-specific commission errors in the Go/NoGo Task (i.e., pressing the button incorrectly in response to the “no go” cues). Stimulus devaluation was assessed by the Implicit Association Test during the pre- and post-training assessments, which measured the strength of positive or negative implicit associations with alcohol.
To be eligible for the study, participants had to have a primary alcohol use disorder diagnosis, be between the ages of 18 and 60 years old, and not have consumed any alcohol for at least 4 weeks prior to the first training session. Participants were not eligible if they had any of the following: any other primary psychiatric diagnosis other than alcohol use disorder; another severe substance use disorder (excluding nicotine); neurocognitive problems; medical conditions that would prevent participation; and insufficient language skills. Of the 743 patients that were assessed for eligibility, 548 were determined to be eligible. Among these, 197 refused to participate and 109 were not able to participate. This resulted in a total of 242 participants in the study, of which 173 completed the 3-month follow-up assessment.
Of the 242 total participants, the majority were male (70%), with an average age of 45 years old and approximately 79 days in residential treatment. Almost half were single, 23% were married, and 27% were divorced. Most (93%) were not taking any medications for alcohol use disorder. Participants had an average of 3.7 prior detoxifications.
WHAT DID THIS STUDY FIND?
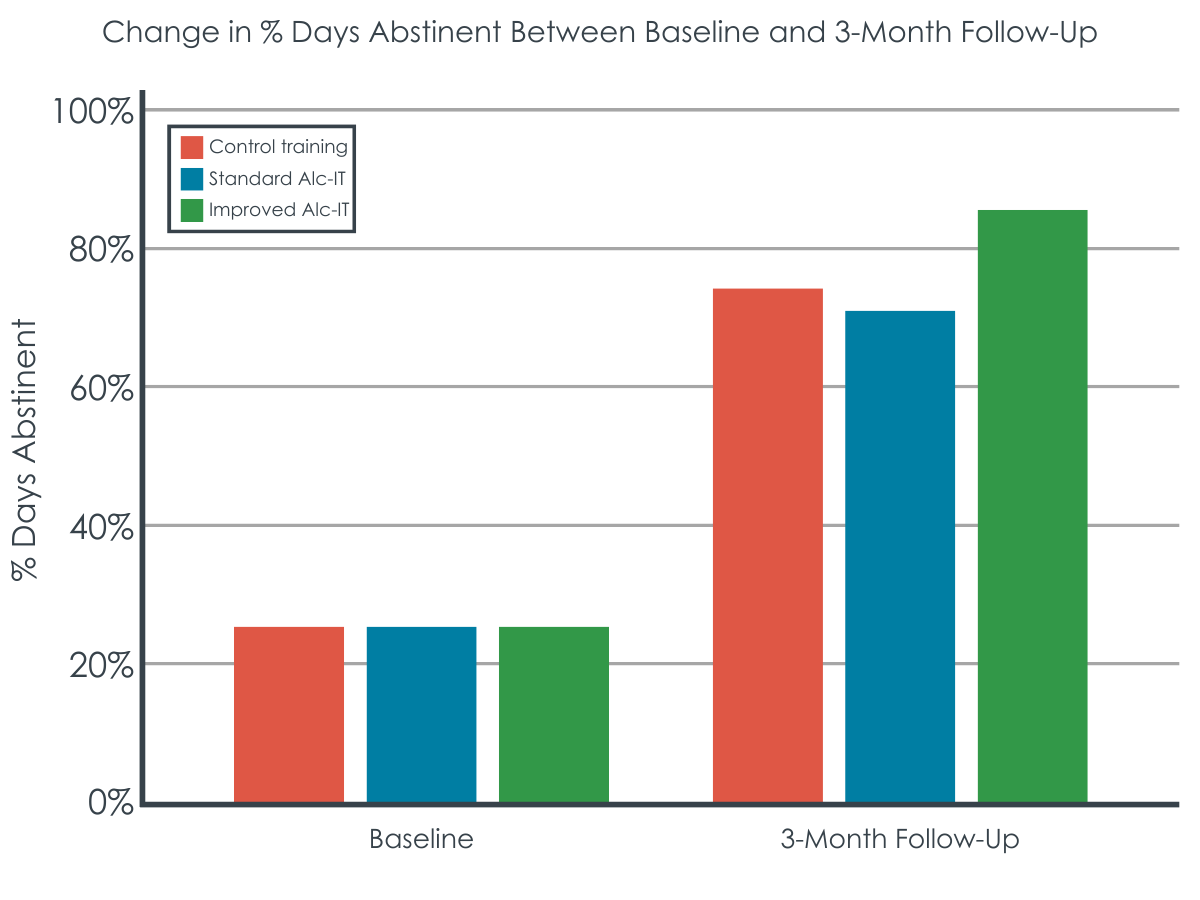
Improved inhibition training resulted in more days abstinent.
Participants who received the improved inhibition training had a higher percentage of days abstinent (86%) at the 3-month follow-up assessment than participants who were in the control group (74%) and the standard inhibition training group (71%). Conversely, participants who received the standard inhibition training did not differ in the percentage of days abstinent from the control group (71% vs. 74%). The benefits of the improved training versus standard training and control did not depend on time of day, age, gender, taking medications, and length of residential treatment stay.
There were no differences, however, between groups for the percentage of heavy drinking days at the 3-month follow-up assessment and the number of days until participants had their first drink.
The new training may have worked through stronger effects on inhibitory control.
In all 3 inhibition training groups, alcohol-related commission errors on the Go/NoGo Task decreased from the pre-assessment to the post-assessment. In the standard inhibition training, errors decreased from a median of 14 to 11. In the improved inhibition training, errors decreased from a median of 14 to 10. In the control inhibition training, errors decreased from 14 to 12.
Alcohol-related commission errors decreased more strongly than neutral errors in the improved inhibition training condition. This effect was not observed in the standard inhibition training condition or in the control inhibition training.
On the other hand, there were no differences between groups on the contrast between positive and negative alcohol associations, consistent with no effect on the value one places on alcohol (i.e., stimulus devaluation).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study investigated the effects of a standard and more challenging (i.e., improved) alcohol-specific inhibition training intervention as compared to a control inhibition training condition on drinking outcomes. Results showed that participants who received the improved inhibition training had more days abstinent at the 3-month follow-up than the standard inhibition training and non-specific control inhibition training, but there were no differences between trainings on the percentage of heavy drinking days and the number of days until participants had their first drink. Accordingly, the training’s main value may be in helping to prevent any alcohol use, but once people start consuming alcohol, this training does not seem to help reduce how much someone may drink. This makes sense given the explicit nature of the trainings used in the intervention that caters more to avoiding any drinking rather reducing consumption once started. The modest effects overall also highlight the need for treatment and recovery approaches to take a comprehensive approach in order to maximize improvements over time, as well as for researchers to investigate further which types of alcohol patients in particular this specific type of inhibitory control training may be particularly helpful.
There were greater decreases in the amount of times someone pressed the bar in response to an alcohol cue (i.e., alcohol-related commission errors), on average, in the improved training group compared to both the standard training and control groups. This provides some support for the inhibitory control hypotheses that suggests that alcohol-specific inhibition training works by enhancing the ability to suppress automatic responses toward choosing to drink alcohol. This is in contrast to the stimulus devaluation hypothesis, which was not supported, that suggests that the working mechanism operates through the development of negative implicit associations with alcohol.
The control training differed from the “improved” training in 2 ways (the ratio of “go” trials to “no go” trials and specificity). This makes the control training more similar to the standard training than the improved version. Thus, the researchers cannot conclude that a training like the control, but with a higher ratio of “go”/”no go” trials, would result in similar effects as the improved training.
The study was conducted with patients who had more severe alcohol use disorder, were in a specialized inpatient treatment program in Switzerland, and had been abstinent for 4+ weeks. Therefore, the results may not generalize to other settings or to people with alcohol use disorder who are not seeking treatment or to those in other types of treatment.
BOTTOM LINE
A more challenging alcohol-specific inhibition training than has been tested in the past resulted in more days abstinent than standard, less challenging, inhibition training and non-specific control inhibition training, which may be a result of improving inhibitory control. However, there were no beneficial effects on other drinking outcomes, suggesting that inhibition training may be a helpful add-on to prevent any drinking at all but less helpful in reducing the amount of drinking once people start. All in all, the intervention might be added to standard care as an add-on and could be most beneficial when administered in combination with a comprehensive treatment and recovery approach.
For individuals and families seeking recovery: This study showed that, on average, patients in residential treatment for alcohol use disorder may benefit from participating in an alcohol-specific inhibition training by increasing post-treatment abstinence. However, because the effects did not extend to other outcomes (e.g., percentage of heavy drinking days), other interventions are needed to reduce harms associated with those particular outcomes.
For treatment professionals and treatment systems: This study demonstrated beneficial effects of an alcohol-specific inhibition training intervention with a high degree of inhibition, when administered during an inpatient treatment program for alcohol use disorder, on the percentage of days abstinent following treatment. Treatment professionals who administer this type of inhibition training interventions as an add-on to inpatient treatment may be able to produce similar effects. However, because effects were isolated to the abstinence outcome only, additional measures may need to be taken in most cases to reduce other kinds of harms related to heavy drinking. Also, professionals who support patients following treatment in comprehensive ways (e.g., linking to employment and housing services) may produce better treatment outcomes.
For scientists: Because the control training in the current study was more similar to the standard training than the improved training, future research that tests an inhibition training non-specific to alcohol with a higher ratio of “go”/”no go” trials would shed light on whether such an intervention can result in similar effects as the improved inhibition training. In addition, future research that tests inhibition training interventions in different treatment contexts (e.g., outpatient settings) and with non-treatment seeking people would help us understand whether results in this study extend to other populations and contexts. Finally, given the beneficial effects on the outcome of days abstinent only, and not on percentage of heavy drinking days and days until first drink, future research may test whether different variations of the training and a different number of sessions results in larger effects on different types of drinking outcomes, as well as which types of patients with alcohol use disorder (or other drug disorder) in particular may be more or less helped by this approach.
For policy makers: Results from this study demonstrated beneficial effects of an alcohol-specific inhibition training intervention with a high degree of inhibition, when administered during an inpatient treatment program for alcohol use disorder, on the percentage of days abstinent following treatment. Such research, however, is limited. Support for scalable, easy-to-administer computerized trainings as an add-on to residential treatment like the one tested here may help improve clinical outcomes.
Computerized inhibition training interventions have been developed with these goals in mind. In such trainings, participants are instructed to press a button in response to stimuli (i.e., a “go” cue), unless a “no go” cue is presented, in which case they would be required to suppress their natural response to press the button. These trainings can be specific to alcohol, where alcohol-related pictures are consistently paired with “no go” cues, or they can be non-specific and paired with other types of pictures, such as water beverages or neutral stimuli.
The ratio of “go” trials to “no go” trials can also vary. To date, most studies investigating the effects of alcohol-specific inhibition trainings have used half “go” trials and half “no go” trials. However, it may be that more challenging trainings could produce greater improvements on one’s ability to inhibit automatic responses toward alcohol thereby improving alcohol use outcomes.
The reasons why alcohol-specific inhibition trainings may work are unclear, but 2 hypotheses have been proposed. The inhibitory control hypothesis suggests that the trainings work by enhancing someone’s ability to suppress automatic responses that make individuals more likely to choose to drink alcohol. The stimulus devaluation hypothesis suggests the trainings work by decreasing someone’s positive associations with alcohol use resulting from consistently pairing the stimulus with the “no go” cue. In other words, requiring someone to suppress an automatic pull toward alcohol may help them begin to associate alcohol with negative rather than positive attributes.
Researchers in this study compared the effects of a standard alcohol-specific inhibition training that used a 50/50 ratio of “go” to “no go” trials vs. an improved alcohol-specific inhibition training that used a more challenging ratio of “go” to “no-go” trials (75/25) vs. a control inhibition training that was not specific to alcohol. They also sought to investigate how the trainings worked if they were shown to be helpful. This research can help shed light on the benefits of inhibition trainings on treatment outcomes and help uncover potential mechanisms of action.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial comparing 2 alcohol-specific inhibition training interventions and a control training condition administered during residential treatment on drinking outcomes 3 months after treatment discharge in adults with alcohol use disorder. Potential working mechanisms were also assessed.
Participants were recruited during admission to the treatment program and, if eligible and willing to participate in the study, were administered baseline assessments during their second week of treatment. This baseline assessment consisted of questionnaires and a calendar-based assessment where they were asked to report their daily alcohol consumption during the previous 90 days.
During the third week of treatment, participants were administered a pre-training assessment, which consisted of questionnaires and completion of experimental tasks assessing inhibitory control. During the fourth and fifth weeks of treatment, participants completed the 6 sessions of inhibition training. Finally, 1-4 days after the last training session, participants were administered a post-training assessment, in which they repeated the questionnaires and experimental tasks that were completed during the pre-training assessment. Participants then finished their 8- to 12-week inpatient stays. After discharge, participants were followed up with at 3, 6, and 12 months. However, the researchers chose to focus on the 3-month follow-up because this time period is an especially sensitive one for potential relapse and training effects are likely to be more salient since it is closer to when the trainings occurred.
Participants were randomized into 3 training conditions, in which they were asked to complete different versions of a modified inhibitory task, called the Go/No Go Task, as an add-on to their residential treatment program. In all 3 training conditions, participants were presented with 320 trials. Eighty of these trials included pictures of alcoholic beverages that were tailored to the participant’s drink of choice (i.e., beer, wine, or spirits), 80 included pictures of water beverages, and 160 included pictures of neutral objects. Participants were instructed to press a button when the “go” cue appeared, but to withhold or inhibit their response when a “no go” cue appeared. The ”no go” cue in all trials was when the same picture was repeated twice.
The 2 training interventions included a standard inhibition training and an “improved” inhibition training. In the standard training, the ratio of “go” and “no go” trials was 50/50, whereas in the improved more challenging training, the ratio was 75/25.
The hypothesis was that, because there were more instances where participants pressed a button in response to the non-alcohol cue (“go”) it would be harder for them to inhibit this automatic response – i.e., not press the button – when an alcohol cue was on the screen (“no go”). Both training interventions were alcohol-specific, meaning that pictures of alcoholic beverages were consistently paired with a “no go” cue, which requires participants to inhibit automatic responses related to alcohol. In the “go” cues, however, the water and neutral pictures were distributed across them. In the control condition, alcohol, water, and neutral picture types were distributed evenly across the “go” and “no go” trials.
The researchers were primarily interested in the outcome of the percentage of days abstinent from alcohol at the 3-month follow-up, as assessed by the Timeline Follow-Back Interview. The interview was conducted during the baseline assessment, which asked about participants’ daily alcohol consumption during the 90 days prior to entering treatment, and the 3-month follow-up assessment, which asked about participants daily alcohol consumption during the 90 days after being discharged from treatment.
The researchers were also interested in the percentage of heavy drinking days (defined as 4+ drinks in a day for women and 5+ for men) at the 3-month follow-up assessment and the number of days until participants had their first drink, as well as potential working mechanisms, which included inhibitory control and stimulus devaluation. Inhibitory control was measured by the number of alcohol-specific commission errors in the Go/NoGo Task (i.e., pressing the button incorrectly in response to the “no go” cues). Stimulus devaluation was assessed by the Implicit Association Test during the pre- and post-training assessments, which measured the strength of positive or negative implicit associations with alcohol.
To be eligible for the study, participants had to have a primary alcohol use disorder diagnosis, be between the ages of 18 and 60 years old, and not have consumed any alcohol for at least 4 weeks prior to the first training session. Participants were not eligible if they had any of the following: any other primary psychiatric diagnosis other than alcohol use disorder; another severe substance use disorder (excluding nicotine); neurocognitive problems; medical conditions that would prevent participation; and insufficient language skills. Of the 743 patients that were assessed for eligibility, 548 were determined to be eligible. Among these, 197 refused to participate and 109 were not able to participate. This resulted in a total of 242 participants in the study, of which 173 completed the 3-month follow-up assessment.
Of the 242 total participants, the majority were male (70%), with an average age of 45 years old and approximately 79 days in residential treatment. Almost half were single, 23% were married, and 27% were divorced. Most (93%) were not taking any medications for alcohol use disorder. Participants had an average of 3.7 prior detoxifications.
WHAT DID THIS STUDY FIND?
Improved inhibition training resulted in more days abstinent.
Participants who received the improved inhibition training had a higher percentage of days abstinent (86%) at the 3-month follow-up assessment than participants who were in the control group (74%) and the standard inhibition training group (71%). Conversely, participants who received the standard inhibition training did not differ in the percentage of days abstinent from the control group (71% vs. 74%). The benefits of the improved training versus standard training and control did not depend on time of day, age, gender, taking medications, and length of residential treatment stay.
There were no differences, however, between groups for the percentage of heavy drinking days at the 3-month follow-up assessment and the number of days until participants had their first drink.
The new training may have worked through stronger effects on inhibitory control.
In all 3 inhibition training groups, alcohol-related commission errors on the Go/NoGo Task decreased from the pre-assessment to the post-assessment. In the standard inhibition training, errors decreased from a median of 14 to 11. In the improved inhibition training, errors decreased from a median of 14 to 10. In the control inhibition training, errors decreased from 14 to 12.
Alcohol-related commission errors decreased more strongly than neutral errors in the improved inhibition training condition. This effect was not observed in the standard inhibition training condition or in the control inhibition training.
On the other hand, there were no differences between groups on the contrast between positive and negative alcohol associations, consistent with no effect on the value one places on alcohol (i.e., stimulus devaluation).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study investigated the effects of a standard and more challenging (i.e., improved) alcohol-specific inhibition training intervention as compared to a control inhibition training condition on drinking outcomes. Results showed that participants who received the improved inhibition training had more days abstinent at the 3-month follow-up than the standard inhibition training and non-specific control inhibition training, but there were no differences between trainings on the percentage of heavy drinking days and the number of days until participants had their first drink. Accordingly, the training’s main value may be in helping to prevent any alcohol use, but once people start consuming alcohol, this training does not seem to help reduce how much someone may drink. This makes sense given the explicit nature of the trainings used in the intervention that caters more to avoiding any drinking rather reducing consumption once started. The modest effects overall also highlight the need for treatment and recovery approaches to take a comprehensive approach in order to maximize improvements over time, as well as for researchers to investigate further which types of alcohol patients in particular this specific type of inhibitory control training may be particularly helpful.
There were greater decreases in the amount of times someone pressed the bar in response to an alcohol cue (i.e., alcohol-related commission errors), on average, in the improved training group compared to both the standard training and control groups. This provides some support for the inhibitory control hypotheses that suggests that alcohol-specific inhibition training works by enhancing the ability to suppress automatic responses toward choosing to drink alcohol. This is in contrast to the stimulus devaluation hypothesis, which was not supported, that suggests that the working mechanism operates through the development of negative implicit associations with alcohol.
The control training differed from the “improved” training in 2 ways (the ratio of “go” trials to “no go” trials and specificity). This makes the control training more similar to the standard training than the improved version. Thus, the researchers cannot conclude that a training like the control, but with a higher ratio of “go”/”no go” trials, would result in similar effects as the improved training.
The study was conducted with patients who had more severe alcohol use disorder, were in a specialized inpatient treatment program in Switzerland, and had been abstinent for 4+ weeks. Therefore, the results may not generalize to other settings or to people with alcohol use disorder who are not seeking treatment or to those in other types of treatment.
BOTTOM LINE
A more challenging alcohol-specific inhibition training than has been tested in the past resulted in more days abstinent than standard, less challenging, inhibition training and non-specific control inhibition training, which may be a result of improving inhibitory control. However, there were no beneficial effects on other drinking outcomes, suggesting that inhibition training may be a helpful add-on to prevent any drinking at all but less helpful in reducing the amount of drinking once people start. All in all, the intervention might be added to standard care as an add-on and could be most beneficial when administered in combination with a comprehensive treatment and recovery approach.
For individuals and families seeking recovery: This study showed that, on average, patients in residential treatment for alcohol use disorder may benefit from participating in an alcohol-specific inhibition training by increasing post-treatment abstinence. However, because the effects did not extend to other outcomes (e.g., percentage of heavy drinking days), other interventions are needed to reduce harms associated with those particular outcomes.
For treatment professionals and treatment systems: This study demonstrated beneficial effects of an alcohol-specific inhibition training intervention with a high degree of inhibition, when administered during an inpatient treatment program for alcohol use disorder, on the percentage of days abstinent following treatment. Treatment professionals who administer this type of inhibition training interventions as an add-on to inpatient treatment may be able to produce similar effects. However, because effects were isolated to the abstinence outcome only, additional measures may need to be taken in most cases to reduce other kinds of harms related to heavy drinking. Also, professionals who support patients following treatment in comprehensive ways (e.g., linking to employment and housing services) may produce better treatment outcomes.
For scientists: Because the control training in the current study was more similar to the standard training than the improved training, future research that tests an inhibition training non-specific to alcohol with a higher ratio of “go”/”no go” trials would shed light on whether such an intervention can result in similar effects as the improved inhibition training. In addition, future research that tests inhibition training interventions in different treatment contexts (e.g., outpatient settings) and with non-treatment seeking people would help us understand whether results in this study extend to other populations and contexts. Finally, given the beneficial effects on the outcome of days abstinent only, and not on percentage of heavy drinking days and days until first drink, future research may test whether different variations of the training and a different number of sessions results in larger effects on different types of drinking outcomes, as well as which types of patients with alcohol use disorder (or other drug disorder) in particular may be more or less helped by this approach.
For policy makers: Results from this study demonstrated beneficial effects of an alcohol-specific inhibition training intervention with a high degree of inhibition, when administered during an inpatient treatment program for alcohol use disorder, on the percentage of days abstinent following treatment. Such research, however, is limited. Support for scalable, easy-to-administer computerized trainings as an add-on to residential treatment like the one tested here may help improve clinical outcomes.
Computerized inhibition training interventions have been developed with these goals in mind. In such trainings, participants are instructed to press a button in response to stimuli (i.e., a “go” cue), unless a “no go” cue is presented, in which case they would be required to suppress their natural response to press the button. These trainings can be specific to alcohol, where alcohol-related pictures are consistently paired with “no go” cues, or they can be non-specific and paired with other types of pictures, such as water beverages or neutral stimuli.
The ratio of “go” trials to “no go” trials can also vary. To date, most studies investigating the effects of alcohol-specific inhibition trainings have used half “go” trials and half “no go” trials. However, it may be that more challenging trainings could produce greater improvements on one’s ability to inhibit automatic responses toward alcohol thereby improving alcohol use outcomes.
The reasons why alcohol-specific inhibition trainings may work are unclear, but 2 hypotheses have been proposed. The inhibitory control hypothesis suggests that the trainings work by enhancing someone’s ability to suppress automatic responses that make individuals more likely to choose to drink alcohol. The stimulus devaluation hypothesis suggests the trainings work by decreasing someone’s positive associations with alcohol use resulting from consistently pairing the stimulus with the “no go” cue. In other words, requiring someone to suppress an automatic pull toward alcohol may help them begin to associate alcohol with negative rather than positive attributes.
Researchers in this study compared the effects of a standard alcohol-specific inhibition training that used a 50/50 ratio of “go” to “no go” trials vs. an improved alcohol-specific inhibition training that used a more challenging ratio of “go” to “no-go” trials (75/25) vs. a control inhibition training that was not specific to alcohol. They also sought to investigate how the trainings worked if they were shown to be helpful. This research can help shed light on the benefits of inhibition trainings on treatment outcomes and help uncover potential mechanisms of action.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled trial comparing 2 alcohol-specific inhibition training interventions and a control training condition administered during residential treatment on drinking outcomes 3 months after treatment discharge in adults with alcohol use disorder. Potential working mechanisms were also assessed.
Participants were recruited during admission to the treatment program and, if eligible and willing to participate in the study, were administered baseline assessments during their second week of treatment. This baseline assessment consisted of questionnaires and a calendar-based assessment where they were asked to report their daily alcohol consumption during the previous 90 days.
During the third week of treatment, participants were administered a pre-training assessment, which consisted of questionnaires and completion of experimental tasks assessing inhibitory control. During the fourth and fifth weeks of treatment, participants completed the 6 sessions of inhibition training. Finally, 1-4 days after the last training session, participants were administered a post-training assessment, in which they repeated the questionnaires and experimental tasks that were completed during the pre-training assessment. Participants then finished their 8- to 12-week inpatient stays. After discharge, participants were followed up with at 3, 6, and 12 months. However, the researchers chose to focus on the 3-month follow-up because this time period is an especially sensitive one for potential relapse and training effects are likely to be more salient since it is closer to when the trainings occurred.
Participants were randomized into 3 training conditions, in which they were asked to complete different versions of a modified inhibitory task, called the Go/No Go Task, as an add-on to their residential treatment program. In all 3 training conditions, participants were presented with 320 trials. Eighty of these trials included pictures of alcoholic beverages that were tailored to the participant’s drink of choice (i.e., beer, wine, or spirits), 80 included pictures of water beverages, and 160 included pictures of neutral objects. Participants were instructed to press a button when the “go” cue appeared, but to withhold or inhibit their response when a “no go” cue appeared. The ”no go” cue in all trials was when the same picture was repeated twice.
The 2 training interventions included a standard inhibition training and an “improved” inhibition training. In the standard training, the ratio of “go” and “no go” trials was 50/50, whereas in the improved more challenging training, the ratio was 75/25.
The hypothesis was that, because there were more instances where participants pressed a button in response to the non-alcohol cue (“go”) it would be harder for them to inhibit this automatic response – i.e., not press the button – when an alcohol cue was on the screen (“no go”). Both training interventions were alcohol-specific, meaning that pictures of alcoholic beverages were consistently paired with a “no go” cue, which requires participants to inhibit automatic responses related to alcohol. In the “go” cues, however, the water and neutral pictures were distributed across them. In the control condition, alcohol, water, and neutral picture types were distributed evenly across the “go” and “no go” trials.
The researchers were primarily interested in the outcome of the percentage of days abstinent from alcohol at the 3-month follow-up, as assessed by the Timeline Follow-Back Interview. The interview was conducted during the baseline assessment, which asked about participants’ daily alcohol consumption during the 90 days prior to entering treatment, and the 3-month follow-up assessment, which asked about participants daily alcohol consumption during the 90 days after being discharged from treatment.
The researchers were also interested in the percentage of heavy drinking days (defined as 4+ drinks in a day for women and 5+ for men) at the 3-month follow-up assessment and the number of days until participants had their first drink, as well as potential working mechanisms, which included inhibitory control and stimulus devaluation. Inhibitory control was measured by the number of alcohol-specific commission errors in the Go/NoGo Task (i.e., pressing the button incorrectly in response to the “no go” cues). Stimulus devaluation was assessed by the Implicit Association Test during the pre- and post-training assessments, which measured the strength of positive or negative implicit associations with alcohol.
To be eligible for the study, participants had to have a primary alcohol use disorder diagnosis, be between the ages of 18 and 60 years old, and not have consumed any alcohol for at least 4 weeks prior to the first training session. Participants were not eligible if they had any of the following: any other primary psychiatric diagnosis other than alcohol use disorder; another severe substance use disorder (excluding nicotine); neurocognitive problems; medical conditions that would prevent participation; and insufficient language skills. Of the 743 patients that were assessed for eligibility, 548 were determined to be eligible. Among these, 197 refused to participate and 109 were not able to participate. This resulted in a total of 242 participants in the study, of which 173 completed the 3-month follow-up assessment.
Of the 242 total participants, the majority were male (70%), with an average age of 45 years old and approximately 79 days in residential treatment. Almost half were single, 23% were married, and 27% were divorced. Most (93%) were not taking any medications for alcohol use disorder. Participants had an average of 3.7 prior detoxifications.
WHAT DID THIS STUDY FIND?
Improved inhibition training resulted in more days abstinent.
Participants who received the improved inhibition training had a higher percentage of days abstinent (86%) at the 3-month follow-up assessment than participants who were in the control group (74%) and the standard inhibition training group (71%). Conversely, participants who received the standard inhibition training did not differ in the percentage of days abstinent from the control group (71% vs. 74%). The benefits of the improved training versus standard training and control did not depend on time of day, age, gender, taking medications, and length of residential treatment stay.
There were no differences, however, between groups for the percentage of heavy drinking days at the 3-month follow-up assessment and the number of days until participants had their first drink.
The new training may have worked through stronger effects on inhibitory control.
In all 3 inhibition training groups, alcohol-related commission errors on the Go/NoGo Task decreased from the pre-assessment to the post-assessment. In the standard inhibition training, errors decreased from a median of 14 to 11. In the improved inhibition training, errors decreased from a median of 14 to 10. In the control inhibition training, errors decreased from 14 to 12.
Alcohol-related commission errors decreased more strongly than neutral errors in the improved inhibition training condition. This effect was not observed in the standard inhibition training condition or in the control inhibition training.
On the other hand, there were no differences between groups on the contrast between positive and negative alcohol associations, consistent with no effect on the value one places on alcohol (i.e., stimulus devaluation).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study investigated the effects of a standard and more challenging (i.e., improved) alcohol-specific inhibition training intervention as compared to a control inhibition training condition on drinking outcomes. Results showed that participants who received the improved inhibition training had more days abstinent at the 3-month follow-up than the standard inhibition training and non-specific control inhibition training, but there were no differences between trainings on the percentage of heavy drinking days and the number of days until participants had their first drink. Accordingly, the training’s main value may be in helping to prevent any alcohol use, but once people start consuming alcohol, this training does not seem to help reduce how much someone may drink. This makes sense given the explicit nature of the trainings used in the intervention that caters more to avoiding any drinking rather reducing consumption once started. The modest effects overall also highlight the need for treatment and recovery approaches to take a comprehensive approach in order to maximize improvements over time, as well as for researchers to investigate further which types of alcohol patients in particular this specific type of inhibitory control training may be particularly helpful.
There were greater decreases in the amount of times someone pressed the bar in response to an alcohol cue (i.e., alcohol-related commission errors), on average, in the improved training group compared to both the standard training and control groups. This provides some support for the inhibitory control hypotheses that suggests that alcohol-specific inhibition training works by enhancing the ability to suppress automatic responses toward choosing to drink alcohol. This is in contrast to the stimulus devaluation hypothesis, which was not supported, that suggests that the working mechanism operates through the development of negative implicit associations with alcohol.
The control training differed from the “improved” training in 2 ways (the ratio of “go” trials to “no go” trials and specificity). This makes the control training more similar to the standard training than the improved version. Thus, the researchers cannot conclude that a training like the control, but with a higher ratio of “go”/”no go” trials, would result in similar effects as the improved training.
The study was conducted with patients who had more severe alcohol use disorder, were in a specialized inpatient treatment program in Switzerland, and had been abstinent for 4+ weeks. Therefore, the results may not generalize to other settings or to people with alcohol use disorder who are not seeking treatment or to those in other types of treatment.
BOTTOM LINE
A more challenging alcohol-specific inhibition training than has been tested in the past resulted in more days abstinent than standard, less challenging, inhibition training and non-specific control inhibition training, which may be a result of improving inhibitory control. However, there were no beneficial effects on other drinking outcomes, suggesting that inhibition training may be a helpful add-on to prevent any drinking at all but less helpful in reducing the amount of drinking once people start. All in all, the intervention might be added to standard care as an add-on and could be most beneficial when administered in combination with a comprehensive treatment and recovery approach.
For individuals and families seeking recovery: This study showed that, on average, patients in residential treatment for alcohol use disorder may benefit from participating in an alcohol-specific inhibition training by increasing post-treatment abstinence. However, because the effects did not extend to other outcomes (e.g., percentage of heavy drinking days), other interventions are needed to reduce harms associated with those particular outcomes.
For treatment professionals and treatment systems: This study demonstrated beneficial effects of an alcohol-specific inhibition training intervention with a high degree of inhibition, when administered during an inpatient treatment program for alcohol use disorder, on the percentage of days abstinent following treatment. Treatment professionals who administer this type of inhibition training interventions as an add-on to inpatient treatment may be able to produce similar effects. However, because effects were isolated to the abstinence outcome only, additional measures may need to be taken in most cases to reduce other kinds of harms related to heavy drinking. Also, professionals who support patients following treatment in comprehensive ways (e.g., linking to employment and housing services) may produce better treatment outcomes.
For scientists: Because the control training in the current study was more similar to the standard training than the improved training, future research that tests an inhibition training non-specific to alcohol with a higher ratio of “go”/”no go” trials would shed light on whether such an intervention can result in similar effects as the improved inhibition training. In addition, future research that tests inhibition training interventions in different treatment contexts (e.g., outpatient settings) and with non-treatment seeking people would help us understand whether results in this study extend to other populations and contexts. Finally, given the beneficial effects on the outcome of days abstinent only, and not on percentage of heavy drinking days and days until first drink, future research may test whether different variations of the training and a different number of sessions results in larger effects on different types of drinking outcomes, as well as which types of patients with alcohol use disorder (or other drug disorder) in particular may be more or less helped by this approach.
For policy makers: Results from this study demonstrated beneficial effects of an alcohol-specific inhibition training intervention with a high degree of inhibition, when administered during an inpatient treatment program for alcohol use disorder, on the percentage of days abstinent following treatment. Such research, however, is limited. Support for scalable, easy-to-administer computerized trainings as an add-on to residential treatment like the one tested here may help improve clinical outcomes.