Co-use of opioid and methamphetamine among persons who inject drugs
The fourth wave of the opioid epidemic is characterized by a rise in opioid-related overdoses that also involve use of illicit stimulants. This study reveals rising trends in the use of methamphetamine and opioids together over time and examines differences by geographic location and individual characteristics.
The opioid overdose epidemic has been described as occurring in 4 waves. Morbidity and mortality were initially attributable to prescription opioid misuse, followed by heroin use, and more recently, the use of fentanyl and other synthetic opioids. The fourth and most recent wave includes a rise in both stimulant and opioid related deaths, suggesting increases in the concomitant use of these drugs. Methamphetamine use has increased substantially in the US over the past several years, with one study suggesting a 43% increase in use between 2015 and 2019. More recently, studies highlight the relationship between methamphetamine and opioid use prevalence that has developed with the modern drug supply and use patterns, showing simultaneous increases in methamphetamine and opioid use and overdose rates over time. When used alone, opioids and methamphetamine are each associated with a host of negative consequences. Co-use of these substances is associated with even greatermental and physicalhealth consequences, including greater risk of infection, greater use of acute care services (e.g., emergency department), and increased risk of overdose and related death.
While regional and national data show a general trend toward increased co-use of methamphetamines and opioids in recent years, many individuals are left out of these datasets. For example, individuals who do not seek treatment as well as people without stable residence or who are unhoused are left out of treatment-related datasets and/or national surveys like the National Survey on Drug Use and Health. As the overdose epidemic evolves, a better understanding of these drug-use trends in various populations are needed to inform novel public health approaches to the shifting epidemic.
To build on prior reports and enhance our knowledge of substance use trends, this study analyzed the prevalence of co-use of opioids and methamphetamine, over time and in different census regions within the US, among the population of people who inject drugs and are disproportionately affected by HIV.
HOW WAS THIS STUDY CONDUCTED?
This study used data from the 2012 (n=10,168), 2015 (n=10,483), and 2018 (n=11,432) cycles of the National HIV Behavioral Surveillance (NHBS) project, the CDC’s comprehensive surveillance dataset assessing populations disproportionately at risk for HIV.
All individuals included in analyses were identified in the database as adults who inject drugs. Analyses assessed changes in self-reported drug use prevalence over time, and compared drug-use rates between people who engaged in the concomitant use of opioids and methamphetamine, to those who engaged in the primary use of only one of these drugs. The role of census regions was also explored.
Prevalence data was examined at 3 timepoints: 2012, 2015, and 2018. Participants self-reported their past-year drug use. Use was defined as using a substance at a frequency of more than once per week at any time over the past 12 months. Eight drug categories were ultimately assessed in the current report, including (1) heroin, (2) prescription opioids (e.g., oxycontin), (3) powder cocaine, (4) crack cocaine, (5) methamphetamine, (6) cannabis, and (7) MDMA (ecstasy). These drug use categories were not mutually exclusive, and participants could report use of more than one drug. To assess ‘opioid use’, heroin and prescription opioid drug categories were combined.
Co-use of opioids and methamphetamines was defined as the endorsement of using both methamphetamine and opioids more than once per week. Two additional mutually-exclusive drug use categories were formed: (1) primary methamphetamine use: methamphetamine use more than once per week, with less frequent or absent opioid use; (2), primary opioid use: opioid use more than once per week, with less frequent or absent methamphetamine use.
Use trends were examined across the United States and in specific census regions, including:
(1) West: WA, OR, CA, CO
(2) Midwest: IL, MI
(3) South: TX, LA, TN, VA, NC, GA, FL, MD, DC, PR
(4) Northeast: MA, NY, PA, NJ
Models examining co-use controlled for age, race, ethnicity, and gender. Such statistical adjustments help to isolate the effect of interest – i.e. whether co-use is independently related to time/year and geographic region.
Participants (n=32,083) were primarily men (70%) in their mid-forties. At the time of the survey, about 45% of the sample did not have a permanent residence (i.e. houseless) and 7% were confirmed HIV positive.
WHAT DID THIS STUDY FIND?
Methamphetamine use increased 3.5 times between 2012 and 2018
The use of all drugs increased from 2012 to 2018. Heroin remained the most prevalent drug used across all 3 timepoints assessed, while methamphetamine use showed the most substantial growth over the 6-year period (a medium-sized effect).
The co-use of methamphetamine and opioids increased, most prevalent in the Western US
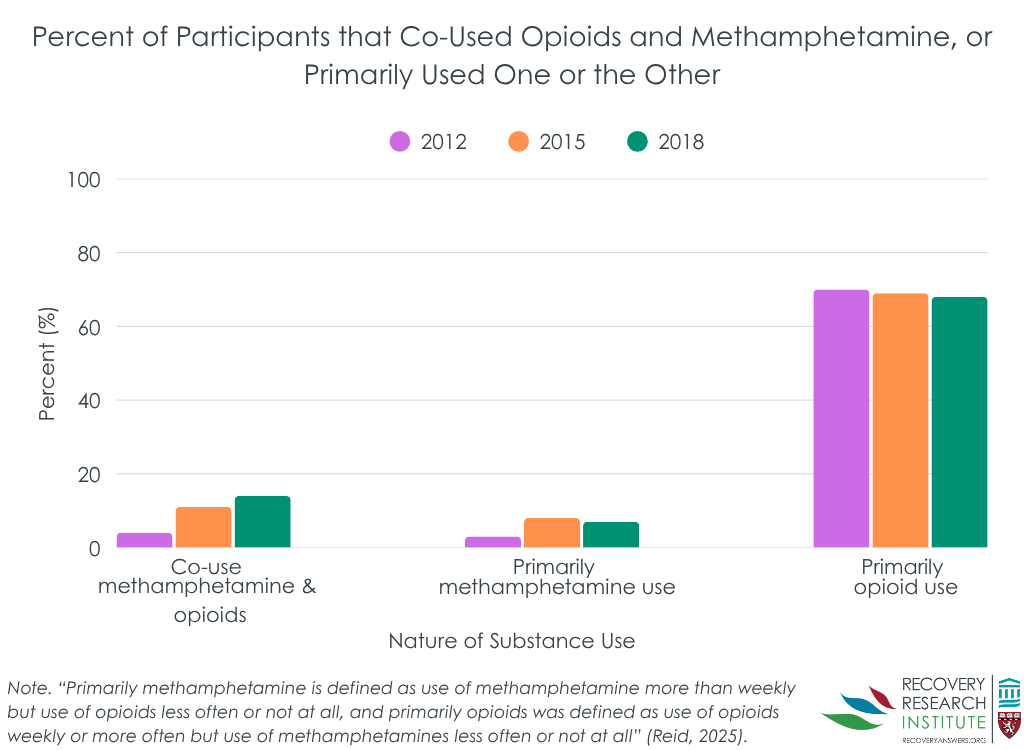
Between 2012 and 2018, the prevalence of individuals who primarily used methamphetamine increased by 2.5 times, and there was no significant change in rates of primary opioid use (see graph below). Regarding co-use, the prevalence of individuals who used both opioids and methamphetamine more than 1 time per week increased by nearly 3 times (small to moderate sized effect).
This increase in co-use prevalence was primarily driven by individuals residing in the Western part of the United States, where opioid-methamphetamine co-use increased to 40% by 2018. Other regions of the US also experienced substantial increases in co-use prevalence, with the Northeast increasing from 0.1% to 5.3% (a medium-sized effect) though the overall prevalence in these regions by 2018 was still low (i.e. ranging from 3% to 10%) relative to Western regions.
Younger adults were more likely to co-use
Individuals who co-used methamphetamine and opioids were more likely to be younger and recently incarcerated, to have overdosed on opioids within the past-year, to inject drugs multiple times per day and share injection equipment (e.g., syringes).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand national drug use trends among at-risk populations. This research is important because it can ultimately help inform novel approaches to address significant public health problems. This study found increased prevalence of the co-use of methamphetamine and opioids between 2012 and 2018, consistent with other national survey studies in broader populations. Methamphetamine use rates also increased independent of co-use, further supporting national trends observed in prior research. Though there were no significant changes in rates of primary opioid use, primary use of opioids was by far the most prevalent drug used across all timeframes assessed, consistent with what we know about the opioid epidemic to date.
This study also suggests that younger and recently incarcerated individuals may be more likely to co-use methamphetamines and opioids, offering a potential population-level target for public health campaigns and novel approaches to help mitigate co-use related harms. As would be expected, co-use was also more likely to be associated with risky drug use behaviors and histories, emphasizing the potential to mitigate co-use related harms alongside injection-related harms in at-risk populations. For example, providing educational resources on the increased risks of co-use, and methods to mitigate those risks, might be easily incorporated into harm reduction platforms like needle exchange programs. Additional research will help determine the best methods for reducing co-use and related overdose deaths over time.
Findings also emphasize the need to address rising rates of co-use across all regions of the United States. Though the Northeast showed the largest percent increase in methamphetamine-opioid co-use between 2012 and 2018 in this study, other research has revealed mixed results with greater time-related increases in co-use observed in the West or Midwest. Discrepancies may be driven by differences in the population studied (e.g., people who inject drugs vs. people starting treatment). Nonetheless, overall prevalence rates were still far higher in the Western region (40%) than any other region of the US (3% to 10%), which is consistent with prior research among treatment-seeking populations and emphasizes the need for ongoing and novel approaches to alarmingly high rates of risky co-use patterns in the Western United States. Efforts are also warranted for non-Western regions to ensure rates don’t approach or surpass Western levels as co-use trends rise over time.
This study used data from a survey that targets populations disproportionately affected by HIV, and therefore, may not be representative of the broader population. Given the sample consisted primarily of middle-aged men who inject drugs in urban regions, this study may not be representative of older and younger adults or of female populations in rural regions who use drugs through other means.
Use was defined as using a substance at a frequency of more than once per week and these data do not reflect individuals who may use substances or their combination less frequently (e.g., every other weekend, once per month).
In the context of this study, co-use of methamphetamine and opioids could mean the use of both drugs at the same time, or it could mean that the individual uses both drugs, but not at the same time or even in the same day. Additional research is needed to determine the potential simultaneous nature of co-use prevalence reported here and the increased risks associated with it.
BOTTOM LINE
Between 2012 and 2018, methamphetamine-opioid co-use increased from 4% to 14% among at-risk adults in the US who inject drugs. Western census regions had the highest prevalence of co-use across the board. When changes in co-use over time were examined, the most prominent increases occurred in the Northeast. Younger age, frequent injection of drugs, past-year opioid overdose, and sharing injection equipment (e.g., syringes) were associated with co-use of methamphetamines and opioids.
For individuals and families seeking recovery: Co-use of methamphetamine and opioids is becoming more common. Even when people don’t intend to use both, the drug supply can include opioids like fentanyl that increase risk of overdose and death. The use of both drugs alongside one another is associated with even greater mental and physical health risk than using one or the other alone. Families and individuals seeking recovery from opioid and methamphetamine use are encouraged to talk to their healthcare providers about their options for treatment, which can be more difficult with this combination and may require more intensive treatment and/or continued care.
For treatment professionals and treatment systems: The co-use of opioids and methamphetamine is becoming more common among the general population and among individuals who inject drugs, particularly among those who are younger and recently incarcerated. Systems in the Western US may see particularly high rates of co-use and rates in other geographical regions are also rising. Given the increased mental and physical health risks associated with co-use, treatment providers and systems are encouraged to screen patients for their polysubstance use patterns as part of their broader treatment plans and to address co-use in a way that acknowledges the greater clinical severity that can accompany it.
For scientists: It is essential to collect and analyze population-level data and longitudinal data concerning methamphetamine and opioid co-use patterns over time in the United States, as well as their influence on overdose, acute care use, and overdose deaths. Relationships between co-use, treatment and recovery pathways, and subsequent recovery outcomes are also warranted. Evaluation of additional subpopulations and vulnerable cohorts, as well as clinical and demographic moderators are also needed to enhance our understanding of the fourth wave of the opioid epidemic to inform public health approaches. The relatively small sample sizes in subgroups examining US census region also warrants purposeful recruitment of individuals representative of each region, which will yield more accurate estimates of regional trends in methamphetamine and opioid co-use.
For policy makers: Studies like these are essential for informing public health policies in the rapidly shifting modern era of illicit drug supply and use. Gaining a better understanding of trends in methamphetamine-opioid co-use can ultimately guide clinical and political approaches to help address the fourth wave of the opioid epidemic (i.e. the co-use of these substances and the deaths associated with it). Additional research funding will help identify more recent drug-use patterns, trajectories over time, and subpopulations driving the epidemic to better inform practice and policy recommendations with the goal of reducing individual and societal burden.
The opioid overdose epidemic has been described as occurring in 4 waves. Morbidity and mortality were initially attributable to prescription opioid misuse, followed by heroin use, and more recently, the use of fentanyl and other synthetic opioids. The fourth and most recent wave includes a rise in both stimulant and opioid related deaths, suggesting increases in the concomitant use of these drugs. Methamphetamine use has increased substantially in the US over the past several years, with one study suggesting a 43% increase in use between 2015 and 2019. More recently, studies highlight the relationship between methamphetamine and opioid use prevalence that has developed with the modern drug supply and use patterns, showing simultaneous increases in methamphetamine and opioid use and overdose rates over time. When used alone, opioids and methamphetamine are each associated with a host of negative consequences. Co-use of these substances is associated with even greatermental and physicalhealth consequences, including greater risk of infection, greater use of acute care services (e.g., emergency department), and increased risk of overdose and related death.
While regional and national data show a general trend toward increased co-use of methamphetamines and opioids in recent years, many individuals are left out of these datasets. For example, individuals who do not seek treatment as well as people without stable residence or who are unhoused are left out of treatment-related datasets and/or national surveys like the National Survey on Drug Use and Health. As the overdose epidemic evolves, a better understanding of these drug-use trends in various populations are needed to inform novel public health approaches to the shifting epidemic.
To build on prior reports and enhance our knowledge of substance use trends, this study analyzed the prevalence of co-use of opioids and methamphetamine, over time and in different census regions within the US, among the population of people who inject drugs and are disproportionately affected by HIV.
HOW WAS THIS STUDY CONDUCTED?
This study used data from the 2012 (n=10,168), 2015 (n=10,483), and 2018 (n=11,432) cycles of the National HIV Behavioral Surveillance (NHBS) project, the CDC’s comprehensive surveillance dataset assessing populations disproportionately at risk for HIV.
All individuals included in analyses were identified in the database as adults who inject drugs. Analyses assessed changes in self-reported drug use prevalence over time, and compared drug-use rates between people who engaged in the concomitant use of opioids and methamphetamine, to those who engaged in the primary use of only one of these drugs. The role of census regions was also explored.
Prevalence data was examined at 3 timepoints: 2012, 2015, and 2018. Participants self-reported their past-year drug use. Use was defined as using a substance at a frequency of more than once per week at any time over the past 12 months. Eight drug categories were ultimately assessed in the current report, including (1) heroin, (2) prescription opioids (e.g., oxycontin), (3) powder cocaine, (4) crack cocaine, (5) methamphetamine, (6) cannabis, and (7) MDMA (ecstasy). These drug use categories were not mutually exclusive, and participants could report use of more than one drug. To assess ‘opioid use’, heroin and prescription opioid drug categories were combined.
Co-use of opioids and methamphetamines was defined as the endorsement of using both methamphetamine and opioids more than once per week. Two additional mutually-exclusive drug use categories were formed: (1) primary methamphetamine use: methamphetamine use more than once per week, with less frequent or absent opioid use; (2), primary opioid use: opioid use more than once per week, with less frequent or absent methamphetamine use.
Use trends were examined across the United States and in specific census regions, including:
(1) West: WA, OR, CA, CO
(2) Midwest: IL, MI
(3) South: TX, LA, TN, VA, NC, GA, FL, MD, DC, PR
(4) Northeast: MA, NY, PA, NJ
Models examining co-use controlled for age, race, ethnicity, and gender. Such statistical adjustments help to isolate the effect of interest – i.e. whether co-use is independently related to time/year and geographic region.
Participants (n=32,083) were primarily men (70%) in their mid-forties. At the time of the survey, about 45% of the sample did not have a permanent residence (i.e. houseless) and 7% were confirmed HIV positive.
WHAT DID THIS STUDY FIND?
Methamphetamine use increased 3.5 times between 2012 and 2018
The use of all drugs increased from 2012 to 2018. Heroin remained the most prevalent drug used across all 3 timepoints assessed, while methamphetamine use showed the most substantial growth over the 6-year period (a medium-sized effect).
The co-use of methamphetamine and opioids increased, most prevalent in the Western US
Between 2012 and 2018, the prevalence of individuals who primarily used methamphetamine increased by 2.5 times, and there was no significant change in rates of primary opioid use (see graph below). Regarding co-use, the prevalence of individuals who used both opioids and methamphetamine more than 1 time per week increased by nearly 3 times (small to moderate sized effect).
This increase in co-use prevalence was primarily driven by individuals residing in the Western part of the United States, where opioid-methamphetamine co-use increased to 40% by 2018. Other regions of the US also experienced substantial increases in co-use prevalence, with the Northeast increasing from 0.1% to 5.3% (a medium-sized effect) though the overall prevalence in these regions by 2018 was still low (i.e. ranging from 3% to 10%) relative to Western regions.
Younger adults were more likely to co-use
Individuals who co-used methamphetamine and opioids were more likely to be younger and recently incarcerated, to have overdosed on opioids within the past-year, to inject drugs multiple times per day and share injection equipment (e.g., syringes).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand national drug use trends among at-risk populations. This research is important because it can ultimately help inform novel approaches to address significant public health problems. This study found increased prevalence of the co-use of methamphetamine and opioids between 2012 and 2018, consistent with other national survey studies in broader populations. Methamphetamine use rates also increased independent of co-use, further supporting national trends observed in prior research. Though there were no significant changes in rates of primary opioid use, primary use of opioids was by far the most prevalent drug used across all timeframes assessed, consistent with what we know about the opioid epidemic to date.
This study also suggests that younger and recently incarcerated individuals may be more likely to co-use methamphetamines and opioids, offering a potential population-level target for public health campaigns and novel approaches to help mitigate co-use related harms. As would be expected, co-use was also more likely to be associated with risky drug use behaviors and histories, emphasizing the potential to mitigate co-use related harms alongside injection-related harms in at-risk populations. For example, providing educational resources on the increased risks of co-use, and methods to mitigate those risks, might be easily incorporated into harm reduction platforms like needle exchange programs. Additional research will help determine the best methods for reducing co-use and related overdose deaths over time.
Findings also emphasize the need to address rising rates of co-use across all regions of the United States. Though the Northeast showed the largest percent increase in methamphetamine-opioid co-use between 2012 and 2018 in this study, other research has revealed mixed results with greater time-related increases in co-use observed in the West or Midwest. Discrepancies may be driven by differences in the population studied (e.g., people who inject drugs vs. people starting treatment). Nonetheless, overall prevalence rates were still far higher in the Western region (40%) than any other region of the US (3% to 10%), which is consistent with prior research among treatment-seeking populations and emphasizes the need for ongoing and novel approaches to alarmingly high rates of risky co-use patterns in the Western United States. Efforts are also warranted for non-Western regions to ensure rates don’t approach or surpass Western levels as co-use trends rise over time.
This study used data from a survey that targets populations disproportionately affected by HIV, and therefore, may not be representative of the broader population. Given the sample consisted primarily of middle-aged men who inject drugs in urban regions, this study may not be representative of older and younger adults or of female populations in rural regions who use drugs through other means.
Use was defined as using a substance at a frequency of more than once per week and these data do not reflect individuals who may use substances or their combination less frequently (e.g., every other weekend, once per month).
In the context of this study, co-use of methamphetamine and opioids could mean the use of both drugs at the same time, or it could mean that the individual uses both drugs, but not at the same time or even in the same day. Additional research is needed to determine the potential simultaneous nature of co-use prevalence reported here and the increased risks associated with it.
BOTTOM LINE
Between 2012 and 2018, methamphetamine-opioid co-use increased from 4% to 14% among at-risk adults in the US who inject drugs. Western census regions had the highest prevalence of co-use across the board. When changes in co-use over time were examined, the most prominent increases occurred in the Northeast. Younger age, frequent injection of drugs, past-year opioid overdose, and sharing injection equipment (e.g., syringes) were associated with co-use of methamphetamines and opioids.
For individuals and families seeking recovery: Co-use of methamphetamine and opioids is becoming more common. Even when people don’t intend to use both, the drug supply can include opioids like fentanyl that increase risk of overdose and death. The use of both drugs alongside one another is associated with even greater mental and physical health risk than using one or the other alone. Families and individuals seeking recovery from opioid and methamphetamine use are encouraged to talk to their healthcare providers about their options for treatment, which can be more difficult with this combination and may require more intensive treatment and/or continued care.
For treatment professionals and treatment systems: The co-use of opioids and methamphetamine is becoming more common among the general population and among individuals who inject drugs, particularly among those who are younger and recently incarcerated. Systems in the Western US may see particularly high rates of co-use and rates in other geographical regions are also rising. Given the increased mental and physical health risks associated with co-use, treatment providers and systems are encouraged to screen patients for their polysubstance use patterns as part of their broader treatment plans and to address co-use in a way that acknowledges the greater clinical severity that can accompany it.
For scientists: It is essential to collect and analyze population-level data and longitudinal data concerning methamphetamine and opioid co-use patterns over time in the United States, as well as their influence on overdose, acute care use, and overdose deaths. Relationships between co-use, treatment and recovery pathways, and subsequent recovery outcomes are also warranted. Evaluation of additional subpopulations and vulnerable cohorts, as well as clinical and demographic moderators are also needed to enhance our understanding of the fourth wave of the opioid epidemic to inform public health approaches. The relatively small sample sizes in subgroups examining US census region also warrants purposeful recruitment of individuals representative of each region, which will yield more accurate estimates of regional trends in methamphetamine and opioid co-use.
For policy makers: Studies like these are essential for informing public health policies in the rapidly shifting modern era of illicit drug supply and use. Gaining a better understanding of trends in methamphetamine-opioid co-use can ultimately guide clinical and political approaches to help address the fourth wave of the opioid epidemic (i.e. the co-use of these substances and the deaths associated with it). Additional research funding will help identify more recent drug-use patterns, trajectories over time, and subpopulations driving the epidemic to better inform practice and policy recommendations with the goal of reducing individual and societal burden.
The opioid overdose epidemic has been described as occurring in 4 waves. Morbidity and mortality were initially attributable to prescription opioid misuse, followed by heroin use, and more recently, the use of fentanyl and other synthetic opioids. The fourth and most recent wave includes a rise in both stimulant and opioid related deaths, suggesting increases in the concomitant use of these drugs. Methamphetamine use has increased substantially in the US over the past several years, with one study suggesting a 43% increase in use between 2015 and 2019. More recently, studies highlight the relationship between methamphetamine and opioid use prevalence that has developed with the modern drug supply and use patterns, showing simultaneous increases in methamphetamine and opioid use and overdose rates over time. When used alone, opioids and methamphetamine are each associated with a host of negative consequences. Co-use of these substances is associated with even greatermental and physicalhealth consequences, including greater risk of infection, greater use of acute care services (e.g., emergency department), and increased risk of overdose and related death.
While regional and national data show a general trend toward increased co-use of methamphetamines and opioids in recent years, many individuals are left out of these datasets. For example, individuals who do not seek treatment as well as people without stable residence or who are unhoused are left out of treatment-related datasets and/or national surveys like the National Survey on Drug Use and Health. As the overdose epidemic evolves, a better understanding of these drug-use trends in various populations are needed to inform novel public health approaches to the shifting epidemic.
To build on prior reports and enhance our knowledge of substance use trends, this study analyzed the prevalence of co-use of opioids and methamphetamine, over time and in different census regions within the US, among the population of people who inject drugs and are disproportionately affected by HIV.
HOW WAS THIS STUDY CONDUCTED?
This study used data from the 2012 (n=10,168), 2015 (n=10,483), and 2018 (n=11,432) cycles of the National HIV Behavioral Surveillance (NHBS) project, the CDC’s comprehensive surveillance dataset assessing populations disproportionately at risk for HIV.
All individuals included in analyses were identified in the database as adults who inject drugs. Analyses assessed changes in self-reported drug use prevalence over time, and compared drug-use rates between people who engaged in the concomitant use of opioids and methamphetamine, to those who engaged in the primary use of only one of these drugs. The role of census regions was also explored.
Prevalence data was examined at 3 timepoints: 2012, 2015, and 2018. Participants self-reported their past-year drug use. Use was defined as using a substance at a frequency of more than once per week at any time over the past 12 months. Eight drug categories were ultimately assessed in the current report, including (1) heroin, (2) prescription opioids (e.g., oxycontin), (3) powder cocaine, (4) crack cocaine, (5) methamphetamine, (6) cannabis, and (7) MDMA (ecstasy). These drug use categories were not mutually exclusive, and participants could report use of more than one drug. To assess ‘opioid use’, heroin and prescription opioid drug categories were combined.
Co-use of opioids and methamphetamines was defined as the endorsement of using both methamphetamine and opioids more than once per week. Two additional mutually-exclusive drug use categories were formed: (1) primary methamphetamine use: methamphetamine use more than once per week, with less frequent or absent opioid use; (2), primary opioid use: opioid use more than once per week, with less frequent or absent methamphetamine use.
Use trends were examined across the United States and in specific census regions, including:
(1) West: WA, OR, CA, CO
(2) Midwest: IL, MI
(3) South: TX, LA, TN, VA, NC, GA, FL, MD, DC, PR
(4) Northeast: MA, NY, PA, NJ
Models examining co-use controlled for age, race, ethnicity, and gender. Such statistical adjustments help to isolate the effect of interest – i.e. whether co-use is independently related to time/year and geographic region.
Participants (n=32,083) were primarily men (70%) in their mid-forties. At the time of the survey, about 45% of the sample did not have a permanent residence (i.e. houseless) and 7% were confirmed HIV positive.
WHAT DID THIS STUDY FIND?
Methamphetamine use increased 3.5 times between 2012 and 2018
The use of all drugs increased from 2012 to 2018. Heroin remained the most prevalent drug used across all 3 timepoints assessed, while methamphetamine use showed the most substantial growth over the 6-year period (a medium-sized effect).
The co-use of methamphetamine and opioids increased, most prevalent in the Western US
Between 2012 and 2018, the prevalence of individuals who primarily used methamphetamine increased by 2.5 times, and there was no significant change in rates of primary opioid use (see graph below). Regarding co-use, the prevalence of individuals who used both opioids and methamphetamine more than 1 time per week increased by nearly 3 times (small to moderate sized effect).
This increase in co-use prevalence was primarily driven by individuals residing in the Western part of the United States, where opioid-methamphetamine co-use increased to 40% by 2018. Other regions of the US also experienced substantial increases in co-use prevalence, with the Northeast increasing from 0.1% to 5.3% (a medium-sized effect) though the overall prevalence in these regions by 2018 was still low (i.e. ranging from 3% to 10%) relative to Western regions.
Younger adults were more likely to co-use
Individuals who co-used methamphetamine and opioids were more likely to be younger and recently incarcerated, to have overdosed on opioids within the past-year, to inject drugs multiple times per day and share injection equipment (e.g., syringes).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand national drug use trends among at-risk populations. This research is important because it can ultimately help inform novel approaches to address significant public health problems. This study found increased prevalence of the co-use of methamphetamine and opioids between 2012 and 2018, consistent with other national survey studies in broader populations. Methamphetamine use rates also increased independent of co-use, further supporting national trends observed in prior research. Though there were no significant changes in rates of primary opioid use, primary use of opioids was by far the most prevalent drug used across all timeframes assessed, consistent with what we know about the opioid epidemic to date.
This study also suggests that younger and recently incarcerated individuals may be more likely to co-use methamphetamines and opioids, offering a potential population-level target for public health campaigns and novel approaches to help mitigate co-use related harms. As would be expected, co-use was also more likely to be associated with risky drug use behaviors and histories, emphasizing the potential to mitigate co-use related harms alongside injection-related harms in at-risk populations. For example, providing educational resources on the increased risks of co-use, and methods to mitigate those risks, might be easily incorporated into harm reduction platforms like needle exchange programs. Additional research will help determine the best methods for reducing co-use and related overdose deaths over time.
Findings also emphasize the need to address rising rates of co-use across all regions of the United States. Though the Northeast showed the largest percent increase in methamphetamine-opioid co-use between 2012 and 2018 in this study, other research has revealed mixed results with greater time-related increases in co-use observed in the West or Midwest. Discrepancies may be driven by differences in the population studied (e.g., people who inject drugs vs. people starting treatment). Nonetheless, overall prevalence rates were still far higher in the Western region (40%) than any other region of the US (3% to 10%), which is consistent with prior research among treatment-seeking populations and emphasizes the need for ongoing and novel approaches to alarmingly high rates of risky co-use patterns in the Western United States. Efforts are also warranted for non-Western regions to ensure rates don’t approach or surpass Western levels as co-use trends rise over time.
This study used data from a survey that targets populations disproportionately affected by HIV, and therefore, may not be representative of the broader population. Given the sample consisted primarily of middle-aged men who inject drugs in urban regions, this study may not be representative of older and younger adults or of female populations in rural regions who use drugs through other means.
Use was defined as using a substance at a frequency of more than once per week and these data do not reflect individuals who may use substances or their combination less frequently (e.g., every other weekend, once per month).
In the context of this study, co-use of methamphetamine and opioids could mean the use of both drugs at the same time, or it could mean that the individual uses both drugs, but not at the same time or even in the same day. Additional research is needed to determine the potential simultaneous nature of co-use prevalence reported here and the increased risks associated with it.
BOTTOM LINE
Between 2012 and 2018, methamphetamine-opioid co-use increased from 4% to 14% among at-risk adults in the US who inject drugs. Western census regions had the highest prevalence of co-use across the board. When changes in co-use over time were examined, the most prominent increases occurred in the Northeast. Younger age, frequent injection of drugs, past-year opioid overdose, and sharing injection equipment (e.g., syringes) were associated with co-use of methamphetamines and opioids.
For individuals and families seeking recovery: Co-use of methamphetamine and opioids is becoming more common. Even when people don’t intend to use both, the drug supply can include opioids like fentanyl that increase risk of overdose and death. The use of both drugs alongside one another is associated with even greater mental and physical health risk than using one or the other alone. Families and individuals seeking recovery from opioid and methamphetamine use are encouraged to talk to their healthcare providers about their options for treatment, which can be more difficult with this combination and may require more intensive treatment and/or continued care.
For treatment professionals and treatment systems: The co-use of opioids and methamphetamine is becoming more common among the general population and among individuals who inject drugs, particularly among those who are younger and recently incarcerated. Systems in the Western US may see particularly high rates of co-use and rates in other geographical regions are also rising. Given the increased mental and physical health risks associated with co-use, treatment providers and systems are encouraged to screen patients for their polysubstance use patterns as part of their broader treatment plans and to address co-use in a way that acknowledges the greater clinical severity that can accompany it.
For scientists: It is essential to collect and analyze population-level data and longitudinal data concerning methamphetamine and opioid co-use patterns over time in the United States, as well as their influence on overdose, acute care use, and overdose deaths. Relationships between co-use, treatment and recovery pathways, and subsequent recovery outcomes are also warranted. Evaluation of additional subpopulations and vulnerable cohorts, as well as clinical and demographic moderators are also needed to enhance our understanding of the fourth wave of the opioid epidemic to inform public health approaches. The relatively small sample sizes in subgroups examining US census region also warrants purposeful recruitment of individuals representative of each region, which will yield more accurate estimates of regional trends in methamphetamine and opioid co-use.
For policy makers: Studies like these are essential for informing public health policies in the rapidly shifting modern era of illicit drug supply and use. Gaining a better understanding of trends in methamphetamine-opioid co-use can ultimately guide clinical and political approaches to help address the fourth wave of the opioid epidemic (i.e. the co-use of these substances and the deaths associated with it). Additional research funding will help identify more recent drug-use patterns, trajectories over time, and subpopulations driving the epidemic to better inform practice and policy recommendations with the goal of reducing individual and societal burden.