Closing the revolving door: How a treatment diversion program can help end the cycle of substance use and crime
Diversion programs, which refer people with substance use disorders to treatment instead of prison, have become increasingly widespread. However, due to the limitations of previous evaluations of such programs, it is unclear how effective they are. This study used a rigorous design to determine the impact of an alcohol and drug diversion program on health and legal outcomes among a sample of justice-involved individuals.
To date, the research suggests that diversion programs can be helpful at preventing drug related criminal offenses. However, this research has notable limitations which make it challenging to determine how effective such programs are. For example, although studies have examined how crime rates differ between those who entered the diversion programs and those who did not, they have often not accounted for individual characteristics including race and ethnicity. In a similar way, researchers have not matched participants on key variables (e.g., substance use severity) across treatment conditions which are likely to impact substance use and recidivism. Furthermore, research to date has often used smaller sample sizes which has made detecting differences between groups challenging. To address these limitations, the current study evaluated the recidivism and health outcomes of people who went through the Magistrates Early Referral into Treatment program, an ongoing voluntary alcohol and drug diversion program in New South Wales, Australia.
HOW WAS THIS STUDY CONDUCTED?
This study utilized retrospective matched cohort of adults with a first appearance in the New South Wales Local Court between 2012 and 2017. From the first date the defendants appeared in court records (the index date) the authors then examined court and health records from the following 2 years to monitor defendants’ criminal activity, healthcare use, and mortality. The health data were obtained by linking criminal justice records to multiple health databases. These databases included the New South Wales Emergency Department Data Collection, Ambulance Emergency Medical Record, and Admitted Patient Data Collection.
Records were included in the analysis if the defendants 1) did not have a conviction for a sexual offense, an indictable offense, or a driving offense, and 2) their charge(s) were not dismissed on mental health grounds. Those who met these criteria and were referred to Magistrates Early Referral into Treatment program at the time of their court appearance were designated as being in the treatment condition. Those who met the same criteria but lived in an area where the program was not offered (and were therefore not offered the program) were designated as being in control condition. The authors then matched those from the control condition to those in the treatment condition based on over 20 variables including pre-treatment substance use and hospital visits. For example, participants were matched on number of prior ambulance callouts in the 2 years before index date. They were also matched on individual factors like age, race and ethnicity, and rurality and socioeconomic conditions of the area in which they lived. This resulted in a sample of 19,302 records.
Defendants enter the Magistrates Early Referral into Treatment program via referral (e.g., via magistrates) at the time of their index date court appearance. While undergoing treatment in the program, criminal proceedings for the original offense(s) are paused. The program entails an intensive 12-week treatment regime tailored to meet the needs of the participants. Individual treatment regimens vary, but include case management, counseling, medically supervised detoxification, pharmacotherapy, and urinalysis. Presiding magistrates receive regular reports on the participant’s treatment progress and can consider this progress as part of final sentencing. This program is voluntary – referred defendants are not required to enter the program as part of a plea deal nor are they punished for not completing the program.
The present study measured several outcomes related to criminal activity, health, and mortality of the participants. To measure criminal activity, the authors assessed whether the current charge(s) led to the defendant receiving a prison sentence, as well as the number of convictions post-referral at both 1- and 2-year post index data. To measure health, the authors assessed hospital admissions for substance use and non-substance use related reasons. These included whether each participant was admitted to the hospital/emergency room or were the subject of an ambulance callout 2 years post-index data. Mortality was assessed by determining if the defendant died for any reason in the 2 years post-index date.
This study consisted of 19,302 matched defendants. The sample was majority male (79%). Most (62%) were between the ages of 18-34 years. Over 66% of defendants came from major cities (e.g., Sydney). Participants included in the analysis had been charged with a wide range of offenses including violent (e.g., assault [18%]), property (e.g., vandalism [23%]), drug (e.g., possession [29%]), breach (e.g., parole violation [14%]), and other (15%) offenses. On average, participants visited the emergency room over 5 times and been admitted to the hospital nearly twice in the 5 years preceding their index date.
WHAT DID THIS STUDY FIND?
Criminal offenses were lower among those referred to the diversion program
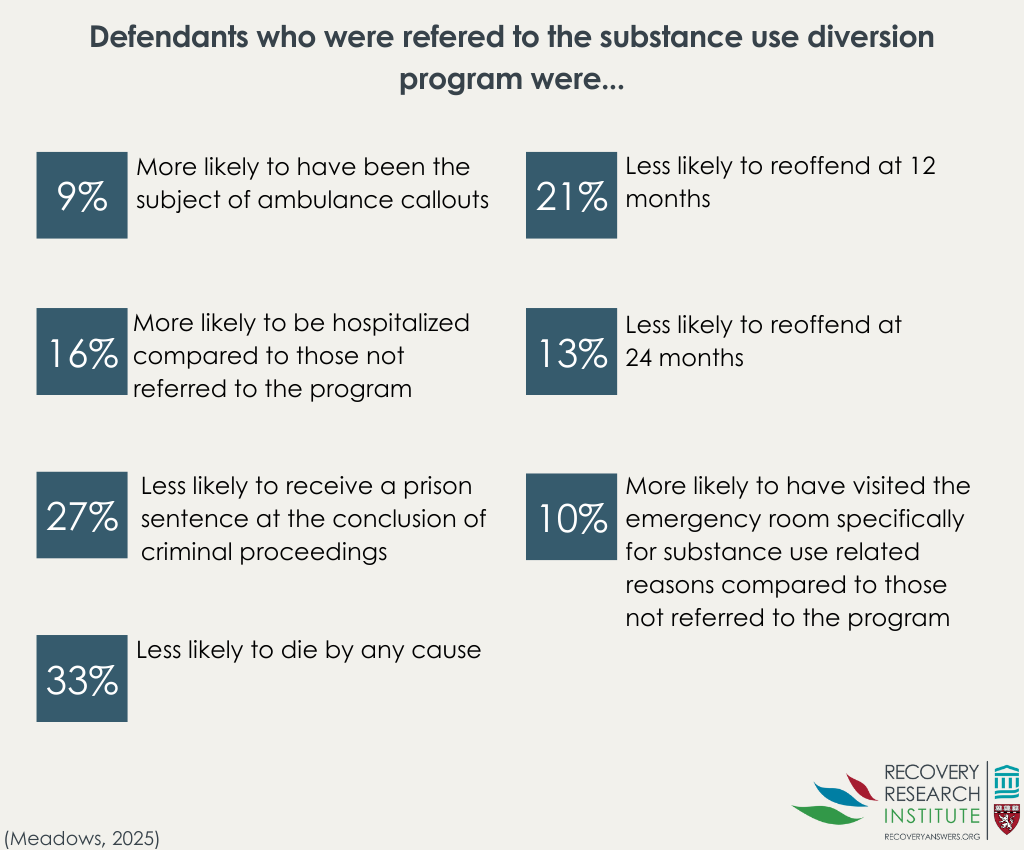
Participants who were referred to the diversion program were 21% and 13% less likely to reoffend at 1 year and 2 years post-referral respectively compared to those who were not referred to the program. In addition, the odds that defendants in the diversion program received a prison sentence at the end of criminal proceedings were 27% lower compared to defendants who had not been referred to the program.
Hospital care usage was higher among those referred to the diversion program
Participants who were referred to the diversion program were 9% more likely to have been the subject of ambulance callouts and 16% more likely to be hospitalized compared to those not referred to the program. In addition, they were 10% more likely to have visited the emergency room specifically for substance use related reasons compared to those not referred to the program.
Mortality rates were lower among defendants in the diversion program
Participants who were referred to the diversion program were 33% less likely to have died for any reason 2 years post-index data than those who were not referred to the program.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study showed that a diversion program could be an effective strategy for reducing future crime. Defendants who were referred to the Magistrates Early Referral into Treatment program were less likely to have reoffended up to 2 years post-referral compared to defendants who were not referred. In addition, those referred to the diversion program had lower odds of being sentenced to prison compared to those who had not been referred to the program. However, the impact of this program on defendants’ health was mixed. Compared to participants who were not referred to the program, those who were referred were more likely to be the subject of an ambulance callout, visit the emergency room, and be admitted to hospitals for treatment. Conversely, mortality among defendants who were referred to the program was lower 2 years after initial court appearance compared to those who had not been referred to the program. It is unknown why these seemingly opposed sets of results were found but may suggest that the experience of substance use treatment increased the likelihood of seeking healthcare. This is somewhat supported by the structure of the Magistrates Early Referral into Treatment program: at the beginning of the program, clients are screened for various health conditions (e.g., viruses and mental health conditions) with healthcare for such conditions becoming part of their care planning. Treatment regimens and needs were then transferred to care providers at exit from the program. In this case, more treatment utilization would be a positive outcome for the diversion program.
It is also possible that despite the matching of treatment and comparison groups, participants still differed meaningfully across conditions in some way. For example, since the control condition was comprised of those who lived in areas where the program was not offered there may be some important differences between the populations. For example, areas where the program was offered may have also had limited access to outpatient treatment for example, making them more dependent on emergency services. This could explain why those in the program were more likely to receive healthcare in acute medical settings. While speculative, it is possible that endemic environmental differences between the groups accounted for this unexpected pattern of results.
Finally, the study did not differentiate between those who completed the program and those who did not. It is likely that those who were referred to the program but did not complete (or start) it had different outcomes than those who successfully completed the program which may partially explain the mixed health results.
Overall, these results suggest that diversion programs like the one tested here may help reduce crime and mortality. The study did not explicitly examine substance use but, given the lower levels of reoffending and likelihood of receiving a prison sentence, it is likely that the program also helped reduce substance use.
There is no way for the researchers to differentiate between those who completed the program and those who did not. The present study only differentiates between those who were referred to the Magistrates Early Referral into Treatment program and those who were not. It seems likely that those who were referred to the program but did not complete (or start) it had different outcomes than those who successfully completed the program which may partially explain the mixed health results. This is somewhat supported by evidence that those who complete similar programs had a positive experience and presumably experience more treatment success.
Administrative data limits the authors’ ability to observe specific health outcomes. For example, the authors could not directly measure rates of substance use related healthcare access (e.g., outpatient treatment). Rather they had to rely on hospitalization records which measured emergency healthcare access. Similarly, the use of such data precluded the authors’ ability to compare rates of substance use between the conditions. Had the authors been able to prospectively track defendants, they may have been able to more accurately measure substance use and treatment access/usage.
The present study sample was derived from defendants in Australia, which may limit the applicability of findings to those in the US. Australia, like most wealthy nations, has universal health coverage, obviating a significant care barrier experienced by those in the US: lack of health coverage. In the US, receiving substance use disorder treatment can be challenging, and it is likely even more difficult for those concurrently navigating the criminal justice system.
BOTTOM LINE
This matched-control study suggests that a diversion program may be effective at reducing crime and recidivism among those with substance use issues in the criminal justice system. Defendants who were referred to the program had lower odds of being sentenced to prison and were less likely to have reoffended up to 2 years post-referral compared to those who were not. The diversion program group’s greater use of emergency medical services may be related to more healthcare utilization, a positive outcome given that they also had lower mortality relative to those who were not referred.
For individuals and families seeking recovery: The present study suggests that treatment-oriented alternatives to incarceration can be helpful in reducing future legal involvement and lowering the risk of early death. Although people referred to the diversion programs used emergency health services more often than others, this may reflect increased healthcare seeking/utilization rather than worsening health. Families can view these programs as opportunities for their loved ones to enter treatment and connect with supportive services. Overall, diversion programs such as the Magistrates Early Referral into Treatment program underscore that treatment-focused approaches can support recovery more effectively than punishment.
For treatment professionals and treatment systems: The present study suggests that diversion programs can reduce recidivism and improve survival among clients. The increased use of emergency and hospital services among referred individuals may signal unmet health needs coming to light, highlighting the importance of coordinated, continuous care during and after program participation. These results suggest that early screening, linkage to care, and structured discharge planning are critical components of effective diversion-based treatment. Strengthening collaboration between courts, community providers, and healthcare systems may further enhance outcomes for justice-involved defendants with substance use disorders.
For scientists: The present study had its limitations, but points to the utility of the studied diversion program, suggesting that there is a need for more rigorous evaluation of diversion programs, including prospective designs that can directly measure substance use patterns, treatment engagement, and longer-term health outcomes. The mixed healthcare findings highlight knowledge gaps about whether increased service use reflects greater need, better access, or changes in health. Future studies should prioritize examining program completion, implementation fidelity, and contextual factors (e.g., endemic resource availability) that may shape outcomes.
For policy makers: The present study suggests that diversion programs can be a promising alternative to punitive approaches to substance use. Referral to the diversion program was associated with reduced recidivism and lower mortality among defendants. The mixed healthcare results, however, may point to the importance of ensuring adequate local resources (e.g., accessible recovery support services) so that diversion programs can function as intended. Investing in robust implementation, monitoring, and evaluation systems could help ensure programs are equitable and effective across regions.
To date, the research suggests that diversion programs can be helpful at preventing drug related criminal offenses. However, this research has notable limitations which make it challenging to determine how effective such programs are. For example, although studies have examined how crime rates differ between those who entered the diversion programs and those who did not, they have often not accounted for individual characteristics including race and ethnicity. In a similar way, researchers have not matched participants on key variables (e.g., substance use severity) across treatment conditions which are likely to impact substance use and recidivism. Furthermore, research to date has often used smaller sample sizes which has made detecting differences between groups challenging. To address these limitations, the current study evaluated the recidivism and health outcomes of people who went through the Magistrates Early Referral into Treatment program, an ongoing voluntary alcohol and drug diversion program in New South Wales, Australia.
HOW WAS THIS STUDY CONDUCTED?
This study utilized retrospective matched cohort of adults with a first appearance in the New South Wales Local Court between 2012 and 2017. From the first date the defendants appeared in court records (the index date) the authors then examined court and health records from the following 2 years to monitor defendants’ criminal activity, healthcare use, and mortality. The health data were obtained by linking criminal justice records to multiple health databases. These databases included the New South Wales Emergency Department Data Collection, Ambulance Emergency Medical Record, and Admitted Patient Data Collection.
Records were included in the analysis if the defendants 1) did not have a conviction for a sexual offense, an indictable offense, or a driving offense, and 2) their charge(s) were not dismissed on mental health grounds. Those who met these criteria and were referred to Magistrates Early Referral into Treatment program at the time of their court appearance were designated as being in the treatment condition. Those who met the same criteria but lived in an area where the program was not offered (and were therefore not offered the program) were designated as being in control condition. The authors then matched those from the control condition to those in the treatment condition based on over 20 variables including pre-treatment substance use and hospital visits. For example, participants were matched on number of prior ambulance callouts in the 2 years before index date. They were also matched on individual factors like age, race and ethnicity, and rurality and socioeconomic conditions of the area in which they lived. This resulted in a sample of 19,302 records.
Defendants enter the Magistrates Early Referral into Treatment program via referral (e.g., via magistrates) at the time of their index date court appearance. While undergoing treatment in the program, criminal proceedings for the original offense(s) are paused. The program entails an intensive 12-week treatment regime tailored to meet the needs of the participants. Individual treatment regimens vary, but include case management, counseling, medically supervised detoxification, pharmacotherapy, and urinalysis. Presiding magistrates receive regular reports on the participant’s treatment progress and can consider this progress as part of final sentencing. This program is voluntary – referred defendants are not required to enter the program as part of a plea deal nor are they punished for not completing the program.
The present study measured several outcomes related to criminal activity, health, and mortality of the participants. To measure criminal activity, the authors assessed whether the current charge(s) led to the defendant receiving a prison sentence, as well as the number of convictions post-referral at both 1- and 2-year post index data. To measure health, the authors assessed hospital admissions for substance use and non-substance use related reasons. These included whether each participant was admitted to the hospital/emergency room or were the subject of an ambulance callout 2 years post-index data. Mortality was assessed by determining if the defendant died for any reason in the 2 years post-index date.
This study consisted of 19,302 matched defendants. The sample was majority male (79%). Most (62%) were between the ages of 18-34 years. Over 66% of defendants came from major cities (e.g., Sydney). Participants included in the analysis had been charged with a wide range of offenses including violent (e.g., assault [18%]), property (e.g., vandalism [23%]), drug (e.g., possession [29%]), breach (e.g., parole violation [14%]), and other (15%) offenses. On average, participants visited the emergency room over 5 times and been admitted to the hospital nearly twice in the 5 years preceding their index date.
WHAT DID THIS STUDY FIND?
Criminal offenses were lower among those referred to the diversion program
Participants who were referred to the diversion program were 21% and 13% less likely to reoffend at 1 year and 2 years post-referral respectively compared to those who were not referred to the program. In addition, the odds that defendants in the diversion program received a prison sentence at the end of criminal proceedings were 27% lower compared to defendants who had not been referred to the program.
Hospital care usage was higher among those referred to the diversion program
Participants who were referred to the diversion program were 9% more likely to have been the subject of ambulance callouts and 16% more likely to be hospitalized compared to those not referred to the program. In addition, they were 10% more likely to have visited the emergency room specifically for substance use related reasons compared to those not referred to the program.
Mortality rates were lower among defendants in the diversion program
Participants who were referred to the diversion program were 33% less likely to have died for any reason 2 years post-index data than those who were not referred to the program.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study showed that a diversion program could be an effective strategy for reducing future crime. Defendants who were referred to the Magistrates Early Referral into Treatment program were less likely to have reoffended up to 2 years post-referral compared to defendants who were not referred. In addition, those referred to the diversion program had lower odds of being sentenced to prison compared to those who had not been referred to the program. However, the impact of this program on defendants’ health was mixed. Compared to participants who were not referred to the program, those who were referred were more likely to be the subject of an ambulance callout, visit the emergency room, and be admitted to hospitals for treatment. Conversely, mortality among defendants who were referred to the program was lower 2 years after initial court appearance compared to those who had not been referred to the program. It is unknown why these seemingly opposed sets of results were found but may suggest that the experience of substance use treatment increased the likelihood of seeking healthcare. This is somewhat supported by the structure of the Magistrates Early Referral into Treatment program: at the beginning of the program, clients are screened for various health conditions (e.g., viruses and mental health conditions) with healthcare for such conditions becoming part of their care planning. Treatment regimens and needs were then transferred to care providers at exit from the program. In this case, more treatment utilization would be a positive outcome for the diversion program.
It is also possible that despite the matching of treatment and comparison groups, participants still differed meaningfully across conditions in some way. For example, since the control condition was comprised of those who lived in areas where the program was not offered there may be some important differences between the populations. For example, areas where the program was offered may have also had limited access to outpatient treatment for example, making them more dependent on emergency services. This could explain why those in the program were more likely to receive healthcare in acute medical settings. While speculative, it is possible that endemic environmental differences between the groups accounted for this unexpected pattern of results.
Finally, the study did not differentiate between those who completed the program and those who did not. It is likely that those who were referred to the program but did not complete (or start) it had different outcomes than those who successfully completed the program which may partially explain the mixed health results.
Overall, these results suggest that diversion programs like the one tested here may help reduce crime and mortality. The study did not explicitly examine substance use but, given the lower levels of reoffending and likelihood of receiving a prison sentence, it is likely that the program also helped reduce substance use.
There is no way for the researchers to differentiate between those who completed the program and those who did not. The present study only differentiates between those who were referred to the Magistrates Early Referral into Treatment program and those who were not. It seems likely that those who were referred to the program but did not complete (or start) it had different outcomes than those who successfully completed the program which may partially explain the mixed health results. This is somewhat supported by evidence that those who complete similar programs had a positive experience and presumably experience more treatment success.
Administrative data limits the authors’ ability to observe specific health outcomes. For example, the authors could not directly measure rates of substance use related healthcare access (e.g., outpatient treatment). Rather they had to rely on hospitalization records which measured emergency healthcare access. Similarly, the use of such data precluded the authors’ ability to compare rates of substance use between the conditions. Had the authors been able to prospectively track defendants, they may have been able to more accurately measure substance use and treatment access/usage.
The present study sample was derived from defendants in Australia, which may limit the applicability of findings to those in the US. Australia, like most wealthy nations, has universal health coverage, obviating a significant care barrier experienced by those in the US: lack of health coverage. In the US, receiving substance use disorder treatment can be challenging, and it is likely even more difficult for those concurrently navigating the criminal justice system.
BOTTOM LINE
This matched-control study suggests that a diversion program may be effective at reducing crime and recidivism among those with substance use issues in the criminal justice system. Defendants who were referred to the program had lower odds of being sentenced to prison and were less likely to have reoffended up to 2 years post-referral compared to those who were not. The diversion program group’s greater use of emergency medical services may be related to more healthcare utilization, a positive outcome given that they also had lower mortality relative to those who were not referred.
For individuals and families seeking recovery: The present study suggests that treatment-oriented alternatives to incarceration can be helpful in reducing future legal involvement and lowering the risk of early death. Although people referred to the diversion programs used emergency health services more often than others, this may reflect increased healthcare seeking/utilization rather than worsening health. Families can view these programs as opportunities for their loved ones to enter treatment and connect with supportive services. Overall, diversion programs such as the Magistrates Early Referral into Treatment program underscore that treatment-focused approaches can support recovery more effectively than punishment.
For treatment professionals and treatment systems: The present study suggests that diversion programs can reduce recidivism and improve survival among clients. The increased use of emergency and hospital services among referred individuals may signal unmet health needs coming to light, highlighting the importance of coordinated, continuous care during and after program participation. These results suggest that early screening, linkage to care, and structured discharge planning are critical components of effective diversion-based treatment. Strengthening collaboration between courts, community providers, and healthcare systems may further enhance outcomes for justice-involved defendants with substance use disorders.
For scientists: The present study had its limitations, but points to the utility of the studied diversion program, suggesting that there is a need for more rigorous evaluation of diversion programs, including prospective designs that can directly measure substance use patterns, treatment engagement, and longer-term health outcomes. The mixed healthcare findings highlight knowledge gaps about whether increased service use reflects greater need, better access, or changes in health. Future studies should prioritize examining program completion, implementation fidelity, and contextual factors (e.g., endemic resource availability) that may shape outcomes.
For policy makers: The present study suggests that diversion programs can be a promising alternative to punitive approaches to substance use. Referral to the diversion program was associated with reduced recidivism and lower mortality among defendants. The mixed healthcare results, however, may point to the importance of ensuring adequate local resources (e.g., accessible recovery support services) so that diversion programs can function as intended. Investing in robust implementation, monitoring, and evaluation systems could help ensure programs are equitable and effective across regions.
To date, the research suggests that diversion programs can be helpful at preventing drug related criminal offenses. However, this research has notable limitations which make it challenging to determine how effective such programs are. For example, although studies have examined how crime rates differ between those who entered the diversion programs and those who did not, they have often not accounted for individual characteristics including race and ethnicity. In a similar way, researchers have not matched participants on key variables (e.g., substance use severity) across treatment conditions which are likely to impact substance use and recidivism. Furthermore, research to date has often used smaller sample sizes which has made detecting differences between groups challenging. To address these limitations, the current study evaluated the recidivism and health outcomes of people who went through the Magistrates Early Referral into Treatment program, an ongoing voluntary alcohol and drug diversion program in New South Wales, Australia.
HOW WAS THIS STUDY CONDUCTED?
This study utilized retrospective matched cohort of adults with a first appearance in the New South Wales Local Court between 2012 and 2017. From the first date the defendants appeared in court records (the index date) the authors then examined court and health records from the following 2 years to monitor defendants’ criminal activity, healthcare use, and mortality. The health data were obtained by linking criminal justice records to multiple health databases. These databases included the New South Wales Emergency Department Data Collection, Ambulance Emergency Medical Record, and Admitted Patient Data Collection.
Records were included in the analysis if the defendants 1) did not have a conviction for a sexual offense, an indictable offense, or a driving offense, and 2) their charge(s) were not dismissed on mental health grounds. Those who met these criteria and were referred to Magistrates Early Referral into Treatment program at the time of their court appearance were designated as being in the treatment condition. Those who met the same criteria but lived in an area where the program was not offered (and were therefore not offered the program) were designated as being in control condition. The authors then matched those from the control condition to those in the treatment condition based on over 20 variables including pre-treatment substance use and hospital visits. For example, participants were matched on number of prior ambulance callouts in the 2 years before index date. They were also matched on individual factors like age, race and ethnicity, and rurality and socioeconomic conditions of the area in which they lived. This resulted in a sample of 19,302 records.
Defendants enter the Magistrates Early Referral into Treatment program via referral (e.g., via magistrates) at the time of their index date court appearance. While undergoing treatment in the program, criminal proceedings for the original offense(s) are paused. The program entails an intensive 12-week treatment regime tailored to meet the needs of the participants. Individual treatment regimens vary, but include case management, counseling, medically supervised detoxification, pharmacotherapy, and urinalysis. Presiding magistrates receive regular reports on the participant’s treatment progress and can consider this progress as part of final sentencing. This program is voluntary – referred defendants are not required to enter the program as part of a plea deal nor are they punished for not completing the program.
The present study measured several outcomes related to criminal activity, health, and mortality of the participants. To measure criminal activity, the authors assessed whether the current charge(s) led to the defendant receiving a prison sentence, as well as the number of convictions post-referral at both 1- and 2-year post index data. To measure health, the authors assessed hospital admissions for substance use and non-substance use related reasons. These included whether each participant was admitted to the hospital/emergency room or were the subject of an ambulance callout 2 years post-index data. Mortality was assessed by determining if the defendant died for any reason in the 2 years post-index date.
This study consisted of 19,302 matched defendants. The sample was majority male (79%). Most (62%) were between the ages of 18-34 years. Over 66% of defendants came from major cities (e.g., Sydney). Participants included in the analysis had been charged with a wide range of offenses including violent (e.g., assault [18%]), property (e.g., vandalism [23%]), drug (e.g., possession [29%]), breach (e.g., parole violation [14%]), and other (15%) offenses. On average, participants visited the emergency room over 5 times and been admitted to the hospital nearly twice in the 5 years preceding their index date.
WHAT DID THIS STUDY FIND?
Criminal offenses were lower among those referred to the diversion program
Participants who were referred to the diversion program were 21% and 13% less likely to reoffend at 1 year and 2 years post-referral respectively compared to those who were not referred to the program. In addition, the odds that defendants in the diversion program received a prison sentence at the end of criminal proceedings were 27% lower compared to defendants who had not been referred to the program.
Hospital care usage was higher among those referred to the diversion program
Participants who were referred to the diversion program were 9% more likely to have been the subject of ambulance callouts and 16% more likely to be hospitalized compared to those not referred to the program. In addition, they were 10% more likely to have visited the emergency room specifically for substance use related reasons compared to those not referred to the program.
Mortality rates were lower among defendants in the diversion program
Participants who were referred to the diversion program were 33% less likely to have died for any reason 2 years post-index data than those who were not referred to the program.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study showed that a diversion program could be an effective strategy for reducing future crime. Defendants who were referred to the Magistrates Early Referral into Treatment program were less likely to have reoffended up to 2 years post-referral compared to defendants who were not referred. In addition, those referred to the diversion program had lower odds of being sentenced to prison compared to those who had not been referred to the program. However, the impact of this program on defendants’ health was mixed. Compared to participants who were not referred to the program, those who were referred were more likely to be the subject of an ambulance callout, visit the emergency room, and be admitted to hospitals for treatment. Conversely, mortality among defendants who were referred to the program was lower 2 years after initial court appearance compared to those who had not been referred to the program. It is unknown why these seemingly opposed sets of results were found but may suggest that the experience of substance use treatment increased the likelihood of seeking healthcare. This is somewhat supported by the structure of the Magistrates Early Referral into Treatment program: at the beginning of the program, clients are screened for various health conditions (e.g., viruses and mental health conditions) with healthcare for such conditions becoming part of their care planning. Treatment regimens and needs were then transferred to care providers at exit from the program. In this case, more treatment utilization would be a positive outcome for the diversion program.
It is also possible that despite the matching of treatment and comparison groups, participants still differed meaningfully across conditions in some way. For example, since the control condition was comprised of those who lived in areas where the program was not offered there may be some important differences between the populations. For example, areas where the program was offered may have also had limited access to outpatient treatment for example, making them more dependent on emergency services. This could explain why those in the program were more likely to receive healthcare in acute medical settings. While speculative, it is possible that endemic environmental differences between the groups accounted for this unexpected pattern of results.
Finally, the study did not differentiate between those who completed the program and those who did not. It is likely that those who were referred to the program but did not complete (or start) it had different outcomes than those who successfully completed the program which may partially explain the mixed health results.
Overall, these results suggest that diversion programs like the one tested here may help reduce crime and mortality. The study did not explicitly examine substance use but, given the lower levels of reoffending and likelihood of receiving a prison sentence, it is likely that the program also helped reduce substance use.
There is no way for the researchers to differentiate between those who completed the program and those who did not. The present study only differentiates between those who were referred to the Magistrates Early Referral into Treatment program and those who were not. It seems likely that those who were referred to the program but did not complete (or start) it had different outcomes than those who successfully completed the program which may partially explain the mixed health results. This is somewhat supported by evidence that those who complete similar programs had a positive experience and presumably experience more treatment success.
Administrative data limits the authors’ ability to observe specific health outcomes. For example, the authors could not directly measure rates of substance use related healthcare access (e.g., outpatient treatment). Rather they had to rely on hospitalization records which measured emergency healthcare access. Similarly, the use of such data precluded the authors’ ability to compare rates of substance use between the conditions. Had the authors been able to prospectively track defendants, they may have been able to more accurately measure substance use and treatment access/usage.
The present study sample was derived from defendants in Australia, which may limit the applicability of findings to those in the US. Australia, like most wealthy nations, has universal health coverage, obviating a significant care barrier experienced by those in the US: lack of health coverage. In the US, receiving substance use disorder treatment can be challenging, and it is likely even more difficult for those concurrently navigating the criminal justice system.
BOTTOM LINE
This matched-control study suggests that a diversion program may be effective at reducing crime and recidivism among those with substance use issues in the criminal justice system. Defendants who were referred to the program had lower odds of being sentenced to prison and were less likely to have reoffended up to 2 years post-referral compared to those who were not. The diversion program group’s greater use of emergency medical services may be related to more healthcare utilization, a positive outcome given that they also had lower mortality relative to those who were not referred.
For individuals and families seeking recovery: The present study suggests that treatment-oriented alternatives to incarceration can be helpful in reducing future legal involvement and lowering the risk of early death. Although people referred to the diversion programs used emergency health services more often than others, this may reflect increased healthcare seeking/utilization rather than worsening health. Families can view these programs as opportunities for their loved ones to enter treatment and connect with supportive services. Overall, diversion programs such as the Magistrates Early Referral into Treatment program underscore that treatment-focused approaches can support recovery more effectively than punishment.
For treatment professionals and treatment systems: The present study suggests that diversion programs can reduce recidivism and improve survival among clients. The increased use of emergency and hospital services among referred individuals may signal unmet health needs coming to light, highlighting the importance of coordinated, continuous care during and after program participation. These results suggest that early screening, linkage to care, and structured discharge planning are critical components of effective diversion-based treatment. Strengthening collaboration between courts, community providers, and healthcare systems may further enhance outcomes for justice-involved defendants with substance use disorders.
For scientists: The present study had its limitations, but points to the utility of the studied diversion program, suggesting that there is a need for more rigorous evaluation of diversion programs, including prospective designs that can directly measure substance use patterns, treatment engagement, and longer-term health outcomes. The mixed healthcare findings highlight knowledge gaps about whether increased service use reflects greater need, better access, or changes in health. Future studies should prioritize examining program completion, implementation fidelity, and contextual factors (e.g., endemic resource availability) that may shape outcomes.
For policy makers: The present study suggests that diversion programs can be a promising alternative to punitive approaches to substance use. Referral to the diversion program was associated with reduced recidivism and lower mortality among defendants. The mixed healthcare results, however, may point to the importance of ensuring adequate local resources (e.g., accessible recovery support services) so that diversion programs can function as intended. Investing in robust implementation, monitoring, and evaluation systems could help ensure programs are equitable and effective across regions.