Can a text-messaging intervention help young adults reduce cannabis use?
Young adults have the highest rates of cannabis use disorder but are the least likely to receive treatment. At the same time, their smartphone use is nearly universal. This study exploited this common use among young adults to test a text message-delivered intervention to reduce their cannabis use.
Young adults report a range of barriers to engaging in cannabis use treatment, including stigma, cost, doubts about treatment effectiveness, not being ready to quit cannabis use entirely, and a preference to self-manage their use. These challenges highlight a need for innovative, scalable interventions that meet the needs and preferences of young adults.
In addition to testing whether a text message-delivered intervention can reduce cannabis use among young adults, understanding how exactly an intervention like this works can help inform and strengthen future interventions. Prior research has identified 3 potential mechanisms of change that explain how cannabis use disorder treatment works: 1) social (peer influences on cannabis use behaviors); 2) cognitive (readiness to change cannabis use behaviors); and 3) behavioral (use of protective behavioral strategies to reduce negative consequences of cannabis use). However, these mechanisms have not been examined within a fully text message-delivered intervention. This study evaluated whether a 4-week, text message-delivered cannabis reduction intervention designed to target peer influence, motivation to change, and harm reduction strategies could reduce cannabis use among young adults, and whether these mechanisms played a significant role in promoting changes in cannabis-related behaviors.
HOW WAS THIS STUDY CONDUCTED?
This study was a 2-arm parallel randomized controlled trial with 1078 young adults (ages 18-25) with likely cannabis use disorder based on a screener, positive toxicology screen for THC, and no recent substance use treatment. Participants were recruited from Colorado (551) and Tennessee (527) through geographically targeted social media ads and flyers posted on college campuses. After enrollment, participants were randomly assigned to either a 4-week text message-delivered intervention or a waitlist control group that only completed assessments, and were followed for 6 months. The sample was a little over half female (57%), mostly White (71%), and just over half (53%) currently enrolled in college.
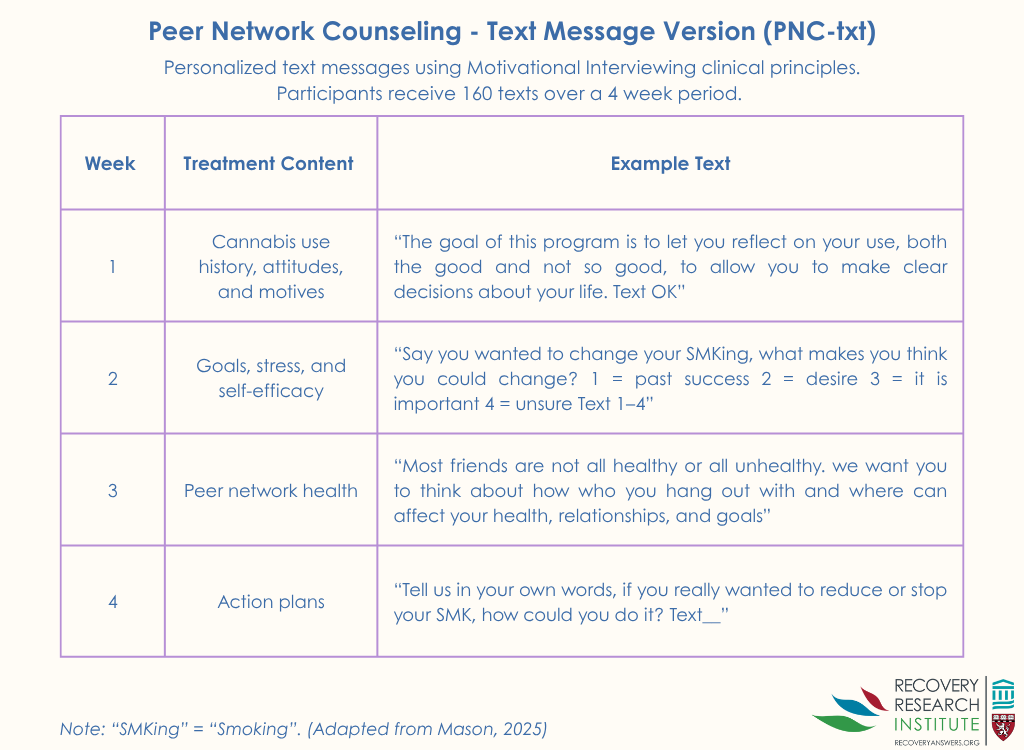
The intervention was adapted from an in-person treatment known as Peer Network Counseling, which employs motivational interviewing principles to explore individuals’ personal goals, bolster motivation to change, and encourage reflection on peer influences (see graphic below). In the text messaged-based version, participants received 160 tailored text messages over 4 weeks, delivered every other day. The messages encouraged participants to consider how their social environment, particularly their closest friends, aligned with or conflicted with their health and life goals. The intervention also delivers content on protective behavioral strategies that can be used to reduce cannabis-related harms, such as only using cannabis on the weekends. Participants completed a baseline survey on their cannabis use, peer relationships, attitudes, goals, and plans for change. The information gathered in the survey was used to personalize the text message conversations, which were delivered through an automated platform. Participants could choose the time of day to receive their texts and had the option to request additional motivational, mental health, or harm reduction messages on demand.
Primary outcomes were self-reported cannabis use (past 30-day frequency) and THC metabolite levels measured by drug tests sent through the mail, assessed at 1, 3, and 6 months post-baseline. Secondary outcomes focused on 3 hypothesized mechanisms of change: 1) motivation to change, measured using the Marijuana Ladder; 2) use of protective behavioral strategies, assessed with the Protective Behavioral Strategies for Marijuana Scale; and 3) peer network health, measured by the Young Adult Social Network Assessment, which calculates the balance of participants’ perceptions of their closest peers’ protective (e.g., encouragement for non-cannabis use) versus risky behaviors (e.g., peer cannabis use)
For the analysis, researchers tested whether changes in cannabis use over time differed significantly between the treatment and control groups. They also conducted mediation analysis to examine whether the intervention influenced cannabis use indirectly, by first increasing motivation to change, improving peer-related factors, or promoting usage of protective behavioral strategies, which then led to reductions in cannabis use.
WHAT DID THIS STUDY FIND?
The text message-delivered intervention did not do better than waitlist control
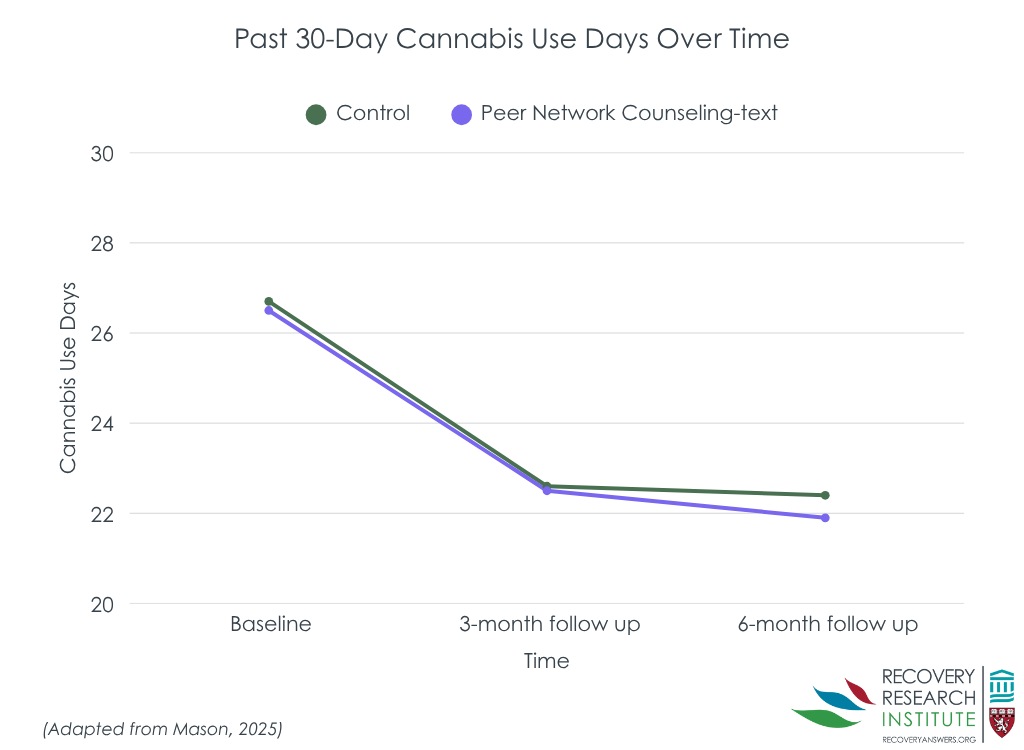
The text-message delivered intervention did not significantly reduce cannabis use compared to the waitlist control group over the 6-month follow-up period (see graph below). However, both groups reported notable reductions of about 4 fewer days of past 30-day cannabis use from baseline to 6 months. At 6 months, participants in the treatment group reported an average of 21.9 days of past 30-day cannabis use, compared to 22.4 days in the control group.
The intervention improved motivation and use of harm reduction strategies, but not changes in peer networks
Compared to controls, the intervention group had greater increases in readiness to change their cannabis use at 1 and 3 months, and greater use of protective behavioral strategies at 1 month. However, the intervention and control groups had similar improvements in their peer network health (i.e., more protective than risk factors) over time.
Cannabis use was indirectly reduced through increased motivation and use of protective behavioral strategies
Although the intervention did not directly reduce cannabis use more compared to the control group, analyses focused on how the treatment worked (i.e., mediation analyses) revealed indirect effects. As mentioned above, the treatment increased motivation to change and use of protective behavioral strategies more than controls at 1 month, and the study also found that shifts in these variables predicted lower cannabis use at 6 months. Together, this suggests the intervention may work by activating these underlying mechanisms of change. Importantly, however, since the intervention and control had similar outcomes despite the intervention doing better on these potential mechanisms (e.g., readiness and protective behavioral strategies), there are likely many other important theoretical factors explaining how young adults modify their cannabis use over time.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Surprisingly, the text message-delivered intervention based on sound psychological and proven intervention principles did not outperform the waitlist control in directly reducing cannabis use over time. However, it did increase motivation to change and the use of protective behavioral strategies, 2 factors that were shown to predict reduced cannabis use at 6 months. That said, despite the treatment working as intended, the similar outcomes for intervention and control mean that there are many other theoretical factors explaining how young adults modify their cannabis use over time. Also of note, though peer influence is a well-established factor in substance use and recovery, and this intervention was designed to create positive shifts in peer networks, the intervention did not produce changes in peer network health, which may require more time or more intensive approaches to be impactful.
Regarding mechanisms of change, findings were mixed when compared to prior research. Earlier studies have supported 3 targeted mechanisms – positive shifts in one’s peer network, readiness to change, and protective behavioral strategies. This text message-delivered adaptation led to increases in motivation to change and use of protective behavioral strategies, but did not produce changes in peer network health. One important caveat is that the study was conducted during the COVID-19 pandemic, a period when limited social interaction may have reduced the influence of peers; though this would be expected to impact groups equally given the randomized design. Notably, the intervention increased readiness to change at 1 month compared to control, which was then associated with reduced cannabis use at 6 months. This finding is consistent with the motivational interviewing framework, which has strong empirical support for reducing substance use. Similarly, increased use of protective behavioral strategies was also linked to reduced cannabis use at 6 months. This aligns with prior research and may reflect a broader pattern among young adults who may be open to reducing cannabis-related harms without pursuing abstinence or in-person treatment. In this context, flexible and accessible digital intervention formats may be particularly well-suited to meet the needs of this population.
The timing of the study during the COVID-19 pandemic may have affected participants’ cannabis use, peer relationships, and engagement with the intervention. Social distancing restrictions may have especially impacted the role of peer dynamics which was one of the three hypothesized clinical mechanisms for the intervention.
The study sample consisted of predominantly White, college-enrolled young adults and findings may not be generalizable to diverse or non-college-attending young adult populations.
This study used an inactive control condition (waitlist control) rather than an active comparison group (e.g., another digital or in-person intervention).
BOTTOM LINE
A brief, text message-delivered intervention did not reduce cannabis use more than a waitlist control, and was found to promote reductions indirectly by increasing motivation to change and encouraging the use of protective behavioral strategies. Given the widespread, daily use of smartphones among young adults, scalable and low-cost digital interventions may offer meaningful public health benefits, particularly for individuals who prefer to self-manage their cannabis use or are unwilling or unable to engage in traditional, in-person treatment. However, for young adults who are already motivated to change their cannabis use, simply tracking cannabis use over time may be just as effective as receiving a structured peer network counseling text message program. Future research is needed to explore how digital tools can be optimized or combined with other supports to enhance their effectiveness.
For individuals and families seeking recovery: For young adults with mild to moderate cannabis use problems who are contemplating changing their cannabis use but may not want to quit entirely, text messaging and other digital support tools might help to enhance motivation to change and encourage the use of harm reduction strategies intended to mitigate harms associated with heavy cannabis use. These self-guided approaches may be appealing for those who prefer to self-manage their cannabis use privately and who do not wish to engage in formal or in-person treatment. However, this study found that adapting an existing in-person intervention like Peer Network Counseling into a text message format may not offer more benefit than simply tracking cannabis use over time, especially for individuals already motivated to make changes. For those with more severe cannabis use or who need additional support, combining digital tools with other services and supports may be necessary to produce meaningful improvements.
For treatment professionals and treatment systems: Substance use treatment providers and systems may consider incorporating smartphone-based interventions, such as text message-delivered programs, as an accessible and scalable option to support young adults looking to reduce or quit their cannabis use. Similarly, treatment providers may consider allocating resources to support the training of staff and integration of digital interventions into their existing services, either as a standalone treatment or adjunct to in-person options. While the benefits of text message interventions for cannabis reductions may be modest, they may help to engage those who prefer self-managed approaches or who do not wish to engage with in-person or more formal services.
For scientists: Findings from this study support readiness to change and protective behavioral strategies as modifiable mechanisms in digital interventions for reducing cannabis use among young adults. However, despite improving on hypothesized mechanisms of behavior change, the text message-based intervention did not outperform a waitlist control in reducing cannabis use. This highlights the need for research than can help refine the theories (e.g., qualitative work) explaining how text message-based approaches for young adult cannabis use are designed to work.
For policy makers: Investing in digital technologies to address young adult cannabis use may offer a cost-effective and scalable way to support to individuals who are unwilling or unable to engage in traditional, in-person treatment. Even modest improvements when multiplied across the larger population to which it could be applied could yield substantial public health benefits.
Young adults report a range of barriers to engaging in cannabis use treatment, including stigma, cost, doubts about treatment effectiveness, not being ready to quit cannabis use entirely, and a preference to self-manage their use. These challenges highlight a need for innovative, scalable interventions that meet the needs and preferences of young adults.
In addition to testing whether a text message-delivered intervention can reduce cannabis use among young adults, understanding how exactly an intervention like this works can help inform and strengthen future interventions. Prior research has identified 3 potential mechanisms of change that explain how cannabis use disorder treatment works: 1) social (peer influences on cannabis use behaviors); 2) cognitive (readiness to change cannabis use behaviors); and 3) behavioral (use of protective behavioral strategies to reduce negative consequences of cannabis use). However, these mechanisms have not been examined within a fully text message-delivered intervention. This study evaluated whether a 4-week, text message-delivered cannabis reduction intervention designed to target peer influence, motivation to change, and harm reduction strategies could reduce cannabis use among young adults, and whether these mechanisms played a significant role in promoting changes in cannabis-related behaviors.
HOW WAS THIS STUDY CONDUCTED?
This study was a 2-arm parallel randomized controlled trial with 1078 young adults (ages 18-25) with likely cannabis use disorder based on a screener, positive toxicology screen for THC, and no recent substance use treatment. Participants were recruited from Colorado (551) and Tennessee (527) through geographically targeted social media ads and flyers posted on college campuses. After enrollment, participants were randomly assigned to either a 4-week text message-delivered intervention or a waitlist control group that only completed assessments, and were followed for 6 months. The sample was a little over half female (57%), mostly White (71%), and just over half (53%) currently enrolled in college.
The intervention was adapted from an in-person treatment known as Peer Network Counseling, which employs motivational interviewing principles to explore individuals’ personal goals, bolster motivation to change, and encourage reflection on peer influences (see graphic below). In the text messaged-based version, participants received 160 tailored text messages over 4 weeks, delivered every other day. The messages encouraged participants to consider how their social environment, particularly their closest friends, aligned with or conflicted with their health and life goals. The intervention also delivers content on protective behavioral strategies that can be used to reduce cannabis-related harms, such as only using cannabis on the weekends. Participants completed a baseline survey on their cannabis use, peer relationships, attitudes, goals, and plans for change. The information gathered in the survey was used to personalize the text message conversations, which were delivered through an automated platform. Participants could choose the time of day to receive their texts and had the option to request additional motivational, mental health, or harm reduction messages on demand.
Primary outcomes were self-reported cannabis use (past 30-day frequency) and THC metabolite levels measured by drug tests sent through the mail, assessed at 1, 3, and 6 months post-baseline. Secondary outcomes focused on 3 hypothesized mechanisms of change: 1) motivation to change, measured using the Marijuana Ladder; 2) use of protective behavioral strategies, assessed with the Protective Behavioral Strategies for Marijuana Scale; and 3) peer network health, measured by the Young Adult Social Network Assessment, which calculates the balance of participants’ perceptions of their closest peers’ protective (e.g., encouragement for non-cannabis use) versus risky behaviors (e.g., peer cannabis use)
For the analysis, researchers tested whether changes in cannabis use over time differed significantly between the treatment and control groups. They also conducted mediation analysis to examine whether the intervention influenced cannabis use indirectly, by first increasing motivation to change, improving peer-related factors, or promoting usage of protective behavioral strategies, which then led to reductions in cannabis use.
WHAT DID THIS STUDY FIND?
The text message-delivered intervention did not do better than waitlist control
The text-message delivered intervention did not significantly reduce cannabis use compared to the waitlist control group over the 6-month follow-up period (see graph below). However, both groups reported notable reductions of about 4 fewer days of past 30-day cannabis use from baseline to 6 months. At 6 months, participants in the treatment group reported an average of 21.9 days of past 30-day cannabis use, compared to 22.4 days in the control group.
The intervention improved motivation and use of harm reduction strategies, but not changes in peer networks
Compared to controls, the intervention group had greater increases in readiness to change their cannabis use at 1 and 3 months, and greater use of protective behavioral strategies at 1 month. However, the intervention and control groups had similar improvements in their peer network health (i.e., more protective than risk factors) over time.
Cannabis use was indirectly reduced through increased motivation and use of protective behavioral strategies
Although the intervention did not directly reduce cannabis use more compared to the control group, analyses focused on how the treatment worked (i.e., mediation analyses) revealed indirect effects. As mentioned above, the treatment increased motivation to change and use of protective behavioral strategies more than controls at 1 month, and the study also found that shifts in these variables predicted lower cannabis use at 6 months. Together, this suggests the intervention may work by activating these underlying mechanisms of change. Importantly, however, since the intervention and control had similar outcomes despite the intervention doing better on these potential mechanisms (e.g., readiness and protective behavioral strategies), there are likely many other important theoretical factors explaining how young adults modify their cannabis use over time.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Surprisingly, the text message-delivered intervention based on sound psychological and proven intervention principles did not outperform the waitlist control in directly reducing cannabis use over time. However, it did increase motivation to change and the use of protective behavioral strategies, 2 factors that were shown to predict reduced cannabis use at 6 months. That said, despite the treatment working as intended, the similar outcomes for intervention and control mean that there are many other theoretical factors explaining how young adults modify their cannabis use over time. Also of note, though peer influence is a well-established factor in substance use and recovery, and this intervention was designed to create positive shifts in peer networks, the intervention did not produce changes in peer network health, which may require more time or more intensive approaches to be impactful.
Regarding mechanisms of change, findings were mixed when compared to prior research. Earlier studies have supported 3 targeted mechanisms – positive shifts in one’s peer network, readiness to change, and protective behavioral strategies. This text message-delivered adaptation led to increases in motivation to change and use of protective behavioral strategies, but did not produce changes in peer network health. One important caveat is that the study was conducted during the COVID-19 pandemic, a period when limited social interaction may have reduced the influence of peers; though this would be expected to impact groups equally given the randomized design. Notably, the intervention increased readiness to change at 1 month compared to control, which was then associated with reduced cannabis use at 6 months. This finding is consistent with the motivational interviewing framework, which has strong empirical support for reducing substance use. Similarly, increased use of protective behavioral strategies was also linked to reduced cannabis use at 6 months. This aligns with prior research and may reflect a broader pattern among young adults who may be open to reducing cannabis-related harms without pursuing abstinence or in-person treatment. In this context, flexible and accessible digital intervention formats may be particularly well-suited to meet the needs of this population.
The timing of the study during the COVID-19 pandemic may have affected participants’ cannabis use, peer relationships, and engagement with the intervention. Social distancing restrictions may have especially impacted the role of peer dynamics which was one of the three hypothesized clinical mechanisms for the intervention.
The study sample consisted of predominantly White, college-enrolled young adults and findings may not be generalizable to diverse or non-college-attending young adult populations.
This study used an inactive control condition (waitlist control) rather than an active comparison group (e.g., another digital or in-person intervention).
BOTTOM LINE
A brief, text message-delivered intervention did not reduce cannabis use more than a waitlist control, and was found to promote reductions indirectly by increasing motivation to change and encouraging the use of protective behavioral strategies. Given the widespread, daily use of smartphones among young adults, scalable and low-cost digital interventions may offer meaningful public health benefits, particularly for individuals who prefer to self-manage their cannabis use or are unwilling or unable to engage in traditional, in-person treatment. However, for young adults who are already motivated to change their cannabis use, simply tracking cannabis use over time may be just as effective as receiving a structured peer network counseling text message program. Future research is needed to explore how digital tools can be optimized or combined with other supports to enhance their effectiveness.
For individuals and families seeking recovery: For young adults with mild to moderate cannabis use problems who are contemplating changing their cannabis use but may not want to quit entirely, text messaging and other digital support tools might help to enhance motivation to change and encourage the use of harm reduction strategies intended to mitigate harms associated with heavy cannabis use. These self-guided approaches may be appealing for those who prefer to self-manage their cannabis use privately and who do not wish to engage in formal or in-person treatment. However, this study found that adapting an existing in-person intervention like Peer Network Counseling into a text message format may not offer more benefit than simply tracking cannabis use over time, especially for individuals already motivated to make changes. For those with more severe cannabis use or who need additional support, combining digital tools with other services and supports may be necessary to produce meaningful improvements.
For treatment professionals and treatment systems: Substance use treatment providers and systems may consider incorporating smartphone-based interventions, such as text message-delivered programs, as an accessible and scalable option to support young adults looking to reduce or quit their cannabis use. Similarly, treatment providers may consider allocating resources to support the training of staff and integration of digital interventions into their existing services, either as a standalone treatment or adjunct to in-person options. While the benefits of text message interventions for cannabis reductions may be modest, they may help to engage those who prefer self-managed approaches or who do not wish to engage with in-person or more formal services.
For scientists: Findings from this study support readiness to change and protective behavioral strategies as modifiable mechanisms in digital interventions for reducing cannabis use among young adults. However, despite improving on hypothesized mechanisms of behavior change, the text message-based intervention did not outperform a waitlist control in reducing cannabis use. This highlights the need for research than can help refine the theories (e.g., qualitative work) explaining how text message-based approaches for young adult cannabis use are designed to work.
For policy makers: Investing in digital technologies to address young adult cannabis use may offer a cost-effective and scalable way to support to individuals who are unwilling or unable to engage in traditional, in-person treatment. Even modest improvements when multiplied across the larger population to which it could be applied could yield substantial public health benefits.
Young adults report a range of barriers to engaging in cannabis use treatment, including stigma, cost, doubts about treatment effectiveness, not being ready to quit cannabis use entirely, and a preference to self-manage their use. These challenges highlight a need for innovative, scalable interventions that meet the needs and preferences of young adults.
In addition to testing whether a text message-delivered intervention can reduce cannabis use among young adults, understanding how exactly an intervention like this works can help inform and strengthen future interventions. Prior research has identified 3 potential mechanisms of change that explain how cannabis use disorder treatment works: 1) social (peer influences on cannabis use behaviors); 2) cognitive (readiness to change cannabis use behaviors); and 3) behavioral (use of protective behavioral strategies to reduce negative consequences of cannabis use). However, these mechanisms have not been examined within a fully text message-delivered intervention. This study evaluated whether a 4-week, text message-delivered cannabis reduction intervention designed to target peer influence, motivation to change, and harm reduction strategies could reduce cannabis use among young adults, and whether these mechanisms played a significant role in promoting changes in cannabis-related behaviors.
HOW WAS THIS STUDY CONDUCTED?
This study was a 2-arm parallel randomized controlled trial with 1078 young adults (ages 18-25) with likely cannabis use disorder based on a screener, positive toxicology screen for THC, and no recent substance use treatment. Participants were recruited from Colorado (551) and Tennessee (527) through geographically targeted social media ads and flyers posted on college campuses. After enrollment, participants were randomly assigned to either a 4-week text message-delivered intervention or a waitlist control group that only completed assessments, and were followed for 6 months. The sample was a little over half female (57%), mostly White (71%), and just over half (53%) currently enrolled in college.
The intervention was adapted from an in-person treatment known as Peer Network Counseling, which employs motivational interviewing principles to explore individuals’ personal goals, bolster motivation to change, and encourage reflection on peer influences (see graphic below). In the text messaged-based version, participants received 160 tailored text messages over 4 weeks, delivered every other day. The messages encouraged participants to consider how their social environment, particularly their closest friends, aligned with or conflicted with their health and life goals. The intervention also delivers content on protective behavioral strategies that can be used to reduce cannabis-related harms, such as only using cannabis on the weekends. Participants completed a baseline survey on their cannabis use, peer relationships, attitudes, goals, and plans for change. The information gathered in the survey was used to personalize the text message conversations, which were delivered through an automated platform. Participants could choose the time of day to receive their texts and had the option to request additional motivational, mental health, or harm reduction messages on demand.
Primary outcomes were self-reported cannabis use (past 30-day frequency) and THC metabolite levels measured by drug tests sent through the mail, assessed at 1, 3, and 6 months post-baseline. Secondary outcomes focused on 3 hypothesized mechanisms of change: 1) motivation to change, measured using the Marijuana Ladder; 2) use of protective behavioral strategies, assessed with the Protective Behavioral Strategies for Marijuana Scale; and 3) peer network health, measured by the Young Adult Social Network Assessment, which calculates the balance of participants’ perceptions of their closest peers’ protective (e.g., encouragement for non-cannabis use) versus risky behaviors (e.g., peer cannabis use)
For the analysis, researchers tested whether changes in cannabis use over time differed significantly between the treatment and control groups. They also conducted mediation analysis to examine whether the intervention influenced cannabis use indirectly, by first increasing motivation to change, improving peer-related factors, or promoting usage of protective behavioral strategies, which then led to reductions in cannabis use.
WHAT DID THIS STUDY FIND?
The text message-delivered intervention did not do better than waitlist control
The text-message delivered intervention did not significantly reduce cannabis use compared to the waitlist control group over the 6-month follow-up period (see graph below). However, both groups reported notable reductions of about 4 fewer days of past 30-day cannabis use from baseline to 6 months. At 6 months, participants in the treatment group reported an average of 21.9 days of past 30-day cannabis use, compared to 22.4 days in the control group.
The intervention improved motivation and use of harm reduction strategies, but not changes in peer networks
Compared to controls, the intervention group had greater increases in readiness to change their cannabis use at 1 and 3 months, and greater use of protective behavioral strategies at 1 month. However, the intervention and control groups had similar improvements in their peer network health (i.e., more protective than risk factors) over time.
Cannabis use was indirectly reduced through increased motivation and use of protective behavioral strategies
Although the intervention did not directly reduce cannabis use more compared to the control group, analyses focused on how the treatment worked (i.e., mediation analyses) revealed indirect effects. As mentioned above, the treatment increased motivation to change and use of protective behavioral strategies more than controls at 1 month, and the study also found that shifts in these variables predicted lower cannabis use at 6 months. Together, this suggests the intervention may work by activating these underlying mechanisms of change. Importantly, however, since the intervention and control had similar outcomes despite the intervention doing better on these potential mechanisms (e.g., readiness and protective behavioral strategies), there are likely many other important theoretical factors explaining how young adults modify their cannabis use over time.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Surprisingly, the text message-delivered intervention based on sound psychological and proven intervention principles did not outperform the waitlist control in directly reducing cannabis use over time. However, it did increase motivation to change and the use of protective behavioral strategies, 2 factors that were shown to predict reduced cannabis use at 6 months. That said, despite the treatment working as intended, the similar outcomes for intervention and control mean that there are many other theoretical factors explaining how young adults modify their cannabis use over time. Also of note, though peer influence is a well-established factor in substance use and recovery, and this intervention was designed to create positive shifts in peer networks, the intervention did not produce changes in peer network health, which may require more time or more intensive approaches to be impactful.
Regarding mechanisms of change, findings were mixed when compared to prior research. Earlier studies have supported 3 targeted mechanisms – positive shifts in one’s peer network, readiness to change, and protective behavioral strategies. This text message-delivered adaptation led to increases in motivation to change and use of protective behavioral strategies, but did not produce changes in peer network health. One important caveat is that the study was conducted during the COVID-19 pandemic, a period when limited social interaction may have reduced the influence of peers; though this would be expected to impact groups equally given the randomized design. Notably, the intervention increased readiness to change at 1 month compared to control, which was then associated with reduced cannabis use at 6 months. This finding is consistent with the motivational interviewing framework, which has strong empirical support for reducing substance use. Similarly, increased use of protective behavioral strategies was also linked to reduced cannabis use at 6 months. This aligns with prior research and may reflect a broader pattern among young adults who may be open to reducing cannabis-related harms without pursuing abstinence or in-person treatment. In this context, flexible and accessible digital intervention formats may be particularly well-suited to meet the needs of this population.
The timing of the study during the COVID-19 pandemic may have affected participants’ cannabis use, peer relationships, and engagement with the intervention. Social distancing restrictions may have especially impacted the role of peer dynamics which was one of the three hypothesized clinical mechanisms for the intervention.
The study sample consisted of predominantly White, college-enrolled young adults and findings may not be generalizable to diverse or non-college-attending young adult populations.
This study used an inactive control condition (waitlist control) rather than an active comparison group (e.g., another digital or in-person intervention).
BOTTOM LINE
A brief, text message-delivered intervention did not reduce cannabis use more than a waitlist control, and was found to promote reductions indirectly by increasing motivation to change and encouraging the use of protective behavioral strategies. Given the widespread, daily use of smartphones among young adults, scalable and low-cost digital interventions may offer meaningful public health benefits, particularly for individuals who prefer to self-manage their cannabis use or are unwilling or unable to engage in traditional, in-person treatment. However, for young adults who are already motivated to change their cannabis use, simply tracking cannabis use over time may be just as effective as receiving a structured peer network counseling text message program. Future research is needed to explore how digital tools can be optimized or combined with other supports to enhance their effectiveness.
For individuals and families seeking recovery: For young adults with mild to moderate cannabis use problems who are contemplating changing their cannabis use but may not want to quit entirely, text messaging and other digital support tools might help to enhance motivation to change and encourage the use of harm reduction strategies intended to mitigate harms associated with heavy cannabis use. These self-guided approaches may be appealing for those who prefer to self-manage their cannabis use privately and who do not wish to engage in formal or in-person treatment. However, this study found that adapting an existing in-person intervention like Peer Network Counseling into a text message format may not offer more benefit than simply tracking cannabis use over time, especially for individuals already motivated to make changes. For those with more severe cannabis use or who need additional support, combining digital tools with other services and supports may be necessary to produce meaningful improvements.
For treatment professionals and treatment systems: Substance use treatment providers and systems may consider incorporating smartphone-based interventions, such as text message-delivered programs, as an accessible and scalable option to support young adults looking to reduce or quit their cannabis use. Similarly, treatment providers may consider allocating resources to support the training of staff and integration of digital interventions into their existing services, either as a standalone treatment or adjunct to in-person options. While the benefits of text message interventions for cannabis reductions may be modest, they may help to engage those who prefer self-managed approaches or who do not wish to engage with in-person or more formal services.
For scientists: Findings from this study support readiness to change and protective behavioral strategies as modifiable mechanisms in digital interventions for reducing cannabis use among young adults. However, despite improving on hypothesized mechanisms of behavior change, the text message-based intervention did not outperform a waitlist control in reducing cannabis use. This highlights the need for research than can help refine the theories (e.g., qualitative work) explaining how text message-based approaches for young adult cannabis use are designed to work.
For policy makers: Investing in digital technologies to address young adult cannabis use may offer a cost-effective and scalable way to support to individuals who are unwilling or unable to engage in traditional, in-person treatment. Even modest improvements when multiplied across the larger population to which it could be applied could yield substantial public health benefits.