Is everyone benefiting from the expansion of telemedicine?
Substance use disorder treatment is increasingly being delivered via telehealth. While this has led to net improvements in access to treatment, overall, individuals with limited or no access to a cellphone or internet may be disadvantaged, especially when living in rural areas that already have fewer treatment options. This study examined the association between technology access and treatment engagement for individuals who live in rural areas.
For many, the shift from in-person to telehealth-based treatment for substance use disorder has increased access to care. However, for individuals with limited or no access cellphone or internet access, telehealth services may be very difficult to access. With some clinics shifting programming from in-person to online, such individuals may have even less access to treatment than they would have had prior to the proliferation of telehealth. This is especially true for people living in rural areas who may be more likely to rely on telehealth services given the physical distance between residential areas and treatment locations.
At the same time, in the United States (US), people living in rural areas are also more likely than those living in urban areas to not have cellphone or internet access. To identify potential disparities to inform policy and practice, this study examined associations between access to technology and engagement with substance use disorder treatment among individuals living in rural areas in 10 US states.
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional, observational study of 3,048 individuals with prior 30-day injection drug or non-prescribed opioid use living in rural areas of 10 US states. Recruitment occurred as part of the Rural Opioid Initiative from January 2018 to March 2020 in rural regions of 10 US stats spanning 65 counties. While the broader goal of this national initiative was to develop and test interventions for people who use drugs from rural US areas, the current study focused on the first phase to characterize participants and local policies in the areas where research sites were located. Participants were 18 years or older, except in Illinois and Wisconsin, where the minimum age for study participation was 15.
Study outcomes included: 1) Receiving outpatient substance use disorder counseling from a clinician or program in the past 30 days, 2) number of days of outpatient substance use disorder counseling in the past 6 months; (3) receipt of a medication for opioid use disorder in the past 30 days, and 4) number of days of self-reported medication for opioid use disorder in the past 6 months.
Participants were asked if they had a cellphone with an active service plan (without distinction between smartphones and other types of cellphones), and if they’d used the internet in the past 30 days. The researchers inferred that participants not using the internet in the past 30 days did not have internet access. Participants were coded as having: 1) Both cellphone and internet access; 2) no cellphone access; 3) no internet access; and 4) neither cellphone nor internet access.
The researchers controlled statistically for a range of individual characteristics such as age, gender, race/ethnicity, education, marital status, health insurance, receipt of general health care in the prior 6 months, Supplemental Nutrition Assistance Program (SNAP) benefits participation, recent incarceration, any overdose in the prior 30 days, and primary substance used. This way, any differences between the four groups in treatment engagement would rule out these potential alternative explanations for the findings.
The study sample was on average 36 years of age, 57% male, 85% White, 96% non-Hispanic, and 88% unmarried. 54% of participants endorsed experiencing homelessness in the past 6 months and 41% had a history of incarceration.
WHAT DID THIS STUDY FIND?
Access to communication technology was low and most participants were not engaged with treatment
In terms of access to technology, 59% of the sample endorsed having both cellphone and past 30-day internet access, 35% did not own a cellphone, 10% had not accessed the internet in the prior 30 days, while 6% had neither a cellphone nor recent past 30-day internet use.
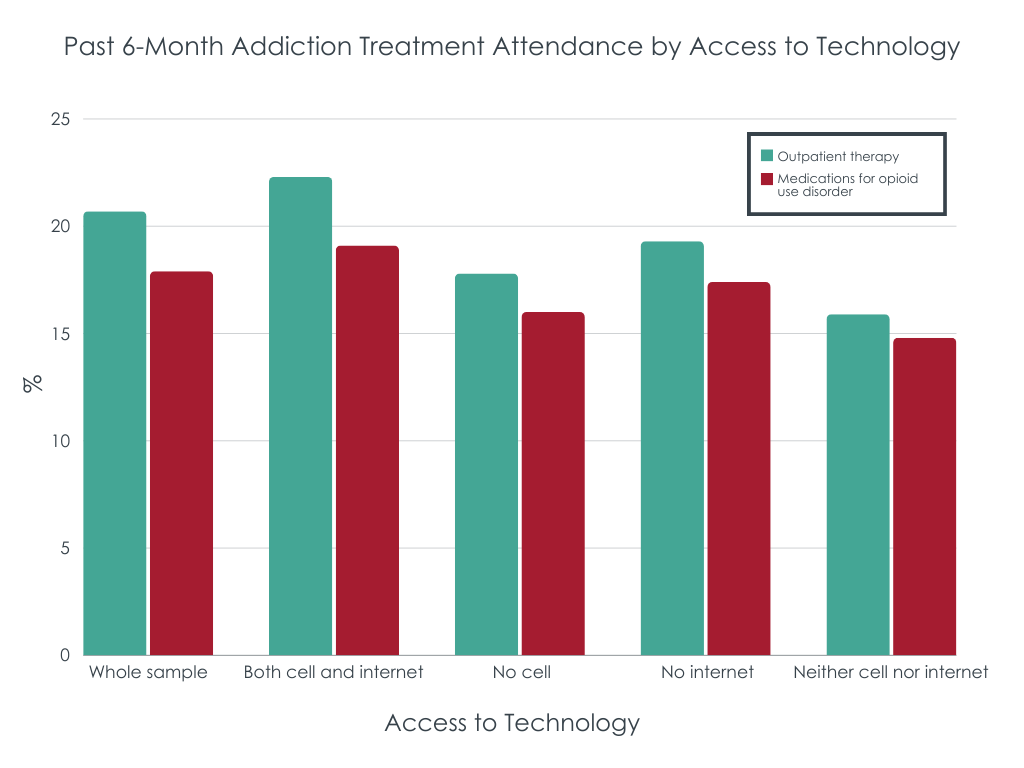
Most participants were not engaged with treatment. In the past 30 days, only 21% of participants reported attending outpatient substance use disorder treatment, and only 18% of participants a medication for opioid use disorder.
Combined cellphone and internet access was associated with better treatment engagement
After controlling for individual characteristics, having both a cellphone and past 30-day internet use, versus neither, was associated with 28% greater odds and 44% more days of recent engagement with outpatient substance use disorder treatment, as well as 29% more days taking opioid use disorder medication over the past 6 months.
Even with internet access, not having a cellphone was associated with worse treatment engagement
Compared to participants with a cellphone, those without a cellphone were 23% less likely to have received outpatient counseling in the past 30 days and 34% less likely to have received outpatient counseling in the past 6 months. And while they were not markedly different in terms of past 30-day receipt of opioid use disorder medication, those without cellphone access were 23% less likely to have received an opioid use disorder medication in the past 6 months.
Having a cellphone appeared to offset not having internet access
Participants with a cellphone were not markedly different in terms of past 30-day, or 6-month counseling or opioid use disorder medication use based on whether they had internet access or not.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The major substance use disorder shift treatment from in-person to telehealth has generally improved access to care, yet many people—often those who are most socially marginalized or geographically isolated—have either not benefited from this shift or may even be worse off because of it. In this study, the researchers found that people who consume opioids and live in rural areas have better engagement with treatment when they have, at a minimum, access to a cellphone, or better yet, access to both a cellphone and the internet. The corollary of this is that those without access to these forms of technology, especially those without cellphone access are far less likely to access care. This is particularly problematic because these are likely also the people in most need of support. At the same time, it is also likely that participants’ access to cell phones and the internet is related to their broader access to resources that could support substance use disorder recovery (e.g., having financial resources, stable housing, employment etc.). In other words, it is likely that for people who do not have digital and online communication technologies, this lack of technology is a marker of lower recovery capital. For example, these individuals may be more impaired for some reason either due to severe addiction or additional other psychiatric problems that may make it more difficult for them to obtain and/or use such technology. While the study controlled for many other factors that would explain the relationship between lack of technology and lower engagement with substance use disorder treatment, there were many variables they could not measure. Future research will ideally measure both remote telehealth substance use disorder care and onsite substance use disorder care. If, in fact, not having technology is a barrier to telehealth engagement, studies needed to measure that and onsite care separately, such that disparities would be present more so for telehealth.
If helping potential patients access a cellphone and the internet would increase the number of people engaging in treatment, ensuring people have access to a cellphone may mitigate a significant barrier to telehealth treatment engagement. Helping prospective patients access a cellphone through programs like the Federal Communications Commission’s (FCC) Federal Lifeline could increase treatment engagement.
This study was cross-sectional, meaning the data were collected at a single point in time. By their nature, cross-sectional studies are limited in their capacity to determine whether the independent variable – technology access in this study – was the cause of differences in outcomes – treatment engagement in this study.
Participants were not formally assessed for opioid use disorder, so it can’t be known what percentage of the sample met diagnostic criteria for it or the degree of severity.
Participants without internet use in the past 30 days were presumed to not have access to the internet. It’s possible some of these participants did have internet access but were not using it for some other reason.
Participants weren’t necessarily seeking treatment for substance use problems. This would have affected rates of treatment engagement in the sample in unknown ways.
Participants were not asked if any of their substance use disorder care was via telehealth, so it is not known how many participants were receiving treatment in-person versus online.
The details of participants’ technology access, such as whether their cellphone had smartphone capabilities or where they accessed the internet (e.g., home versus a public place) were not assessed. Given a basic cellphone and smartphone have very different functionality, it will be important to assess this detail in future studies seeking to understand the impact of cellphone access on treatment engagement.
The perceived usefulness of having a cellphone or available internet in interacting with services, were not assessed. Ideally future studies will assess the subjective utility of technology for accessing treatment.
BOTTOM LINE
The rapid expansion of telehealth services has increased access to substance use disorder care, but not everyone is experiencing this increased access equally. The researchers’ findings indicate that many individuals who use opioids and live in rural settings have limited access to cellphones and internet, and that this in turn is associated with lower rates of treatment engagement. While their results indicate having access to both a cellphone and the internet would be most ideal, at a minimum, having at least a cellphone may help buffer against some of these detriments. It is also possible that cellphone and internet access reflect broader access to resources that can support treatment engagement and substance use disorder recovery (e.g., greater financial resources, stable housing, employment) and that these factors are really driving the researchers’ findings.
For individuals and families seeking recovery: In the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, communication technology access is obviously critical. Federal programs are available that can help individuals with limited means get a smartphone.
For treatment professionals and treatment systems: In the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, communication technology access is obviously critical. Finding ways to get prospective patients cellphone access, at a minimum, could increase treatment engagement.
For scientists: Access to communication technology has become increasingly important as the substance use disorder treatment field has shifted to providing more services via telehealth. The researchers’ findings suggest cellphone ownership, at a minimum, may help offset some of detriments on treatment engagement of having limited access to communication technology. Future studies will ideally determine if a cellphone is enough to offset these detriments, and what kinds of treatment engagement cellphone ownership offsets (i.e., telehealth vs. in-person services). The perceived utility of communication technology in treatment engagement among individuals who use drugs could also be explored.
For policy makers: Given the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, it is important individuals seeking substance use disorder treatment have access to communication technology. Making communication technology like cellphones a reimbursable health insurance expense and existing programs like the Federal Lifeline for Low-Income Consumers could help offset any potential disparities.
For many, the shift from in-person to telehealth-based treatment for substance use disorder has increased access to care. However, for individuals with limited or no access cellphone or internet access, telehealth services may be very difficult to access. With some clinics shifting programming from in-person to online, such individuals may have even less access to treatment than they would have had prior to the proliferation of telehealth. This is especially true for people living in rural areas who may be more likely to rely on telehealth services given the physical distance between residential areas and treatment locations.
At the same time, in the United States (US), people living in rural areas are also more likely than those living in urban areas to not have cellphone or internet access. To identify potential disparities to inform policy and practice, this study examined associations between access to technology and engagement with substance use disorder treatment among individuals living in rural areas in 10 US states.
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional, observational study of 3,048 individuals with prior 30-day injection drug or non-prescribed opioid use living in rural areas of 10 US states. Recruitment occurred as part of the Rural Opioid Initiative from January 2018 to March 2020 in rural regions of 10 US stats spanning 65 counties. While the broader goal of this national initiative was to develop and test interventions for people who use drugs from rural US areas, the current study focused on the first phase to characterize participants and local policies in the areas where research sites were located. Participants were 18 years or older, except in Illinois and Wisconsin, where the minimum age for study participation was 15.
Study outcomes included: 1) Receiving outpatient substance use disorder counseling from a clinician or program in the past 30 days, 2) number of days of outpatient substance use disorder counseling in the past 6 months; (3) receipt of a medication for opioid use disorder in the past 30 days, and 4) number of days of self-reported medication for opioid use disorder in the past 6 months.
Participants were asked if they had a cellphone with an active service plan (without distinction between smartphones and other types of cellphones), and if they’d used the internet in the past 30 days. The researchers inferred that participants not using the internet in the past 30 days did not have internet access. Participants were coded as having: 1) Both cellphone and internet access; 2) no cellphone access; 3) no internet access; and 4) neither cellphone nor internet access.
The researchers controlled statistically for a range of individual characteristics such as age, gender, race/ethnicity, education, marital status, health insurance, receipt of general health care in the prior 6 months, Supplemental Nutrition Assistance Program (SNAP) benefits participation, recent incarceration, any overdose in the prior 30 days, and primary substance used. This way, any differences between the four groups in treatment engagement would rule out these potential alternative explanations for the findings.
The study sample was on average 36 years of age, 57% male, 85% White, 96% non-Hispanic, and 88% unmarried. 54% of participants endorsed experiencing homelessness in the past 6 months and 41% had a history of incarceration.
WHAT DID THIS STUDY FIND?
Access to communication technology was low and most participants were not engaged with treatment
In terms of access to technology, 59% of the sample endorsed having both cellphone and past 30-day internet access, 35% did not own a cellphone, 10% had not accessed the internet in the prior 30 days, while 6% had neither a cellphone nor recent past 30-day internet use.
Most participants were not engaged with treatment. In the past 30 days, only 21% of participants reported attending outpatient substance use disorder treatment, and only 18% of participants a medication for opioid use disorder.
Combined cellphone and internet access was associated with better treatment engagement
After controlling for individual characteristics, having both a cellphone and past 30-day internet use, versus neither, was associated with 28% greater odds and 44% more days of recent engagement with outpatient substance use disorder treatment, as well as 29% more days taking opioid use disorder medication over the past 6 months.
Even with internet access, not having a cellphone was associated with worse treatment engagement
Compared to participants with a cellphone, those without a cellphone were 23% less likely to have received outpatient counseling in the past 30 days and 34% less likely to have received outpatient counseling in the past 6 months. And while they were not markedly different in terms of past 30-day receipt of opioid use disorder medication, those without cellphone access were 23% less likely to have received an opioid use disorder medication in the past 6 months.
Having a cellphone appeared to offset not having internet access
Participants with a cellphone were not markedly different in terms of past 30-day, or 6-month counseling or opioid use disorder medication use based on whether they had internet access or not.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The major substance use disorder shift treatment from in-person to telehealth has generally improved access to care, yet many people—often those who are most socially marginalized or geographically isolated—have either not benefited from this shift or may even be worse off because of it. In this study, the researchers found that people who consume opioids and live in rural areas have better engagement with treatment when they have, at a minimum, access to a cellphone, or better yet, access to both a cellphone and the internet. The corollary of this is that those without access to these forms of technology, especially those without cellphone access are far less likely to access care. This is particularly problematic because these are likely also the people in most need of support. At the same time, it is also likely that participants’ access to cell phones and the internet is related to their broader access to resources that could support substance use disorder recovery (e.g., having financial resources, stable housing, employment etc.). In other words, it is likely that for people who do not have digital and online communication technologies, this lack of technology is a marker of lower recovery capital. For example, these individuals may be more impaired for some reason either due to severe addiction or additional other psychiatric problems that may make it more difficult for them to obtain and/or use such technology. While the study controlled for many other factors that would explain the relationship between lack of technology and lower engagement with substance use disorder treatment, there were many variables they could not measure. Future research will ideally measure both remote telehealth substance use disorder care and onsite substance use disorder care. If, in fact, not having technology is a barrier to telehealth engagement, studies needed to measure that and onsite care separately, such that disparities would be present more so for telehealth.
If helping potential patients access a cellphone and the internet would increase the number of people engaging in treatment, ensuring people have access to a cellphone may mitigate a significant barrier to telehealth treatment engagement. Helping prospective patients access a cellphone through programs like the Federal Communications Commission’s (FCC) Federal Lifeline could increase treatment engagement.
This study was cross-sectional, meaning the data were collected at a single point in time. By their nature, cross-sectional studies are limited in their capacity to determine whether the independent variable – technology access in this study – was the cause of differences in outcomes – treatment engagement in this study.
Participants were not formally assessed for opioid use disorder, so it can’t be known what percentage of the sample met diagnostic criteria for it or the degree of severity.
Participants without internet use in the past 30 days were presumed to not have access to the internet. It’s possible some of these participants did have internet access but were not using it for some other reason.
Participants weren’t necessarily seeking treatment for substance use problems. This would have affected rates of treatment engagement in the sample in unknown ways.
Participants were not asked if any of their substance use disorder care was via telehealth, so it is not known how many participants were receiving treatment in-person versus online.
The details of participants’ technology access, such as whether their cellphone had smartphone capabilities or where they accessed the internet (e.g., home versus a public place) were not assessed. Given a basic cellphone and smartphone have very different functionality, it will be important to assess this detail in future studies seeking to understand the impact of cellphone access on treatment engagement.
The perceived usefulness of having a cellphone or available internet in interacting with services, were not assessed. Ideally future studies will assess the subjective utility of technology for accessing treatment.
BOTTOM LINE
The rapid expansion of telehealth services has increased access to substance use disorder care, but not everyone is experiencing this increased access equally. The researchers’ findings indicate that many individuals who use opioids and live in rural settings have limited access to cellphones and internet, and that this in turn is associated with lower rates of treatment engagement. While their results indicate having access to both a cellphone and the internet would be most ideal, at a minimum, having at least a cellphone may help buffer against some of these detriments. It is also possible that cellphone and internet access reflect broader access to resources that can support treatment engagement and substance use disorder recovery (e.g., greater financial resources, stable housing, employment) and that these factors are really driving the researchers’ findings.
For individuals and families seeking recovery: In the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, communication technology access is obviously critical. Federal programs are available that can help individuals with limited means get a smartphone.
For treatment professionals and treatment systems: In the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, communication technology access is obviously critical. Finding ways to get prospective patients cellphone access, at a minimum, could increase treatment engagement.
For scientists: Access to communication technology has become increasingly important as the substance use disorder treatment field has shifted to providing more services via telehealth. The researchers’ findings suggest cellphone ownership, at a minimum, may help offset some of detriments on treatment engagement of having limited access to communication technology. Future studies will ideally determine if a cellphone is enough to offset these detriments, and what kinds of treatment engagement cellphone ownership offsets (i.e., telehealth vs. in-person services). The perceived utility of communication technology in treatment engagement among individuals who use drugs could also be explored.
For policy makers: Given the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, it is important individuals seeking substance use disorder treatment have access to communication technology. Making communication technology like cellphones a reimbursable health insurance expense and existing programs like the Federal Lifeline for Low-Income Consumers could help offset any potential disparities.
For many, the shift from in-person to telehealth-based treatment for substance use disorder has increased access to care. However, for individuals with limited or no access cellphone or internet access, telehealth services may be very difficult to access. With some clinics shifting programming from in-person to online, such individuals may have even less access to treatment than they would have had prior to the proliferation of telehealth. This is especially true for people living in rural areas who may be more likely to rely on telehealth services given the physical distance between residential areas and treatment locations.
At the same time, in the United States (US), people living in rural areas are also more likely than those living in urban areas to not have cellphone or internet access. To identify potential disparities to inform policy and practice, this study examined associations between access to technology and engagement with substance use disorder treatment among individuals living in rural areas in 10 US states.
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional, observational study of 3,048 individuals with prior 30-day injection drug or non-prescribed opioid use living in rural areas of 10 US states. Recruitment occurred as part of the Rural Opioid Initiative from January 2018 to March 2020 in rural regions of 10 US stats spanning 65 counties. While the broader goal of this national initiative was to develop and test interventions for people who use drugs from rural US areas, the current study focused on the first phase to characterize participants and local policies in the areas where research sites were located. Participants were 18 years or older, except in Illinois and Wisconsin, where the minimum age for study participation was 15.
Study outcomes included: 1) Receiving outpatient substance use disorder counseling from a clinician or program in the past 30 days, 2) number of days of outpatient substance use disorder counseling in the past 6 months; (3) receipt of a medication for opioid use disorder in the past 30 days, and 4) number of days of self-reported medication for opioid use disorder in the past 6 months.
Participants were asked if they had a cellphone with an active service plan (without distinction between smartphones and other types of cellphones), and if they’d used the internet in the past 30 days. The researchers inferred that participants not using the internet in the past 30 days did not have internet access. Participants were coded as having: 1) Both cellphone and internet access; 2) no cellphone access; 3) no internet access; and 4) neither cellphone nor internet access.
The researchers controlled statistically for a range of individual characteristics such as age, gender, race/ethnicity, education, marital status, health insurance, receipt of general health care in the prior 6 months, Supplemental Nutrition Assistance Program (SNAP) benefits participation, recent incarceration, any overdose in the prior 30 days, and primary substance used. This way, any differences between the four groups in treatment engagement would rule out these potential alternative explanations for the findings.
The study sample was on average 36 years of age, 57% male, 85% White, 96% non-Hispanic, and 88% unmarried. 54% of participants endorsed experiencing homelessness in the past 6 months and 41% had a history of incarceration.
WHAT DID THIS STUDY FIND?
Access to communication technology was low and most participants were not engaged with treatment
In terms of access to technology, 59% of the sample endorsed having both cellphone and past 30-day internet access, 35% did not own a cellphone, 10% had not accessed the internet in the prior 30 days, while 6% had neither a cellphone nor recent past 30-day internet use.
Most participants were not engaged with treatment. In the past 30 days, only 21% of participants reported attending outpatient substance use disorder treatment, and only 18% of participants a medication for opioid use disorder.
Combined cellphone and internet access was associated with better treatment engagement
After controlling for individual characteristics, having both a cellphone and past 30-day internet use, versus neither, was associated with 28% greater odds and 44% more days of recent engagement with outpatient substance use disorder treatment, as well as 29% more days taking opioid use disorder medication over the past 6 months.
Even with internet access, not having a cellphone was associated with worse treatment engagement
Compared to participants with a cellphone, those without a cellphone were 23% less likely to have received outpatient counseling in the past 30 days and 34% less likely to have received outpatient counseling in the past 6 months. And while they were not markedly different in terms of past 30-day receipt of opioid use disorder medication, those without cellphone access were 23% less likely to have received an opioid use disorder medication in the past 6 months.
Having a cellphone appeared to offset not having internet access
Participants with a cellphone were not markedly different in terms of past 30-day, or 6-month counseling or opioid use disorder medication use based on whether they had internet access or not.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The major substance use disorder shift treatment from in-person to telehealth has generally improved access to care, yet many people—often those who are most socially marginalized or geographically isolated—have either not benefited from this shift or may even be worse off because of it. In this study, the researchers found that people who consume opioids and live in rural areas have better engagement with treatment when they have, at a minimum, access to a cellphone, or better yet, access to both a cellphone and the internet. The corollary of this is that those without access to these forms of technology, especially those without cellphone access are far less likely to access care. This is particularly problematic because these are likely also the people in most need of support. At the same time, it is also likely that participants’ access to cell phones and the internet is related to their broader access to resources that could support substance use disorder recovery (e.g., having financial resources, stable housing, employment etc.). In other words, it is likely that for people who do not have digital and online communication technologies, this lack of technology is a marker of lower recovery capital. For example, these individuals may be more impaired for some reason either due to severe addiction or additional other psychiatric problems that may make it more difficult for them to obtain and/or use such technology. While the study controlled for many other factors that would explain the relationship between lack of technology and lower engagement with substance use disorder treatment, there were many variables they could not measure. Future research will ideally measure both remote telehealth substance use disorder care and onsite substance use disorder care. If, in fact, not having technology is a barrier to telehealth engagement, studies needed to measure that and onsite care separately, such that disparities would be present more so for telehealth.
If helping potential patients access a cellphone and the internet would increase the number of people engaging in treatment, ensuring people have access to a cellphone may mitigate a significant barrier to telehealth treatment engagement. Helping prospective patients access a cellphone through programs like the Federal Communications Commission’s (FCC) Federal Lifeline could increase treatment engagement.
This study was cross-sectional, meaning the data were collected at a single point in time. By their nature, cross-sectional studies are limited in their capacity to determine whether the independent variable – technology access in this study – was the cause of differences in outcomes – treatment engagement in this study.
Participants were not formally assessed for opioid use disorder, so it can’t be known what percentage of the sample met diagnostic criteria for it or the degree of severity.
Participants without internet use in the past 30 days were presumed to not have access to the internet. It’s possible some of these participants did have internet access but were not using it for some other reason.
Participants weren’t necessarily seeking treatment for substance use problems. This would have affected rates of treatment engagement in the sample in unknown ways.
Participants were not asked if any of their substance use disorder care was via telehealth, so it is not known how many participants were receiving treatment in-person versus online.
The details of participants’ technology access, such as whether their cellphone had smartphone capabilities or where they accessed the internet (e.g., home versus a public place) were not assessed. Given a basic cellphone and smartphone have very different functionality, it will be important to assess this detail in future studies seeking to understand the impact of cellphone access on treatment engagement.
The perceived usefulness of having a cellphone or available internet in interacting with services, were not assessed. Ideally future studies will assess the subjective utility of technology for accessing treatment.
BOTTOM LINE
The rapid expansion of telehealth services has increased access to substance use disorder care, but not everyone is experiencing this increased access equally. The researchers’ findings indicate that many individuals who use opioids and live in rural settings have limited access to cellphones and internet, and that this in turn is associated with lower rates of treatment engagement. While their results indicate having access to both a cellphone and the internet would be most ideal, at a minimum, having at least a cellphone may help buffer against some of these detriments. It is also possible that cellphone and internet access reflect broader access to resources that can support treatment engagement and substance use disorder recovery (e.g., greater financial resources, stable housing, employment) and that these factors are really driving the researchers’ findings.
For individuals and families seeking recovery: In the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, communication technology access is obviously critical. Federal programs are available that can help individuals with limited means get a smartphone.
For treatment professionals and treatment systems: In the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, communication technology access is obviously critical. Finding ways to get prospective patients cellphone access, at a minimum, could increase treatment engagement.
For scientists: Access to communication technology has become increasingly important as the substance use disorder treatment field has shifted to providing more services via telehealth. The researchers’ findings suggest cellphone ownership, at a minimum, may help offset some of detriments on treatment engagement of having limited access to communication technology. Future studies will ideally determine if a cellphone is enough to offset these detriments, and what kinds of treatment engagement cellphone ownership offsets (i.e., telehealth vs. in-person services). The perceived utility of communication technology in treatment engagement among individuals who use drugs could also be explored.
For policy makers: Given the shifting substance use disorder treatment landscape that is increasingly emphasizing telehealth services, it is important individuals seeking substance use disorder treatment have access to communication technology. Making communication technology like cellphones a reimbursable health insurance expense and existing programs like the Federal Lifeline for Low-Income Consumers could help offset any potential disparities.