WHAT PROBLEM DOES THIS STUDY ADDRESS?
Despite continued need, substance use disorder treatment utilization remains low: in 2022, less than 5% of people who needed substance use disorder treatment received it. Many factors contribute to underutilization of treatment, including inaccessibility of treatment and lack of long-term follow-up from providers. Recovery Management Checkups are empirically-supported continuing care-style interventions designed to help re-engage people with treatment if necessary, and regularly monitor treatment engagement and effectiveness over 12 months. Although there is evidence that Recovery Management Check-Ups work well in primary care settings, it is unknown how best to implement such interventions into real-world healthcare settings. This study describes the implementation of a Recovery Management Checkup intervention within a federally qualified health center.
HOW WAS THIS STUDY CONDUCTED?
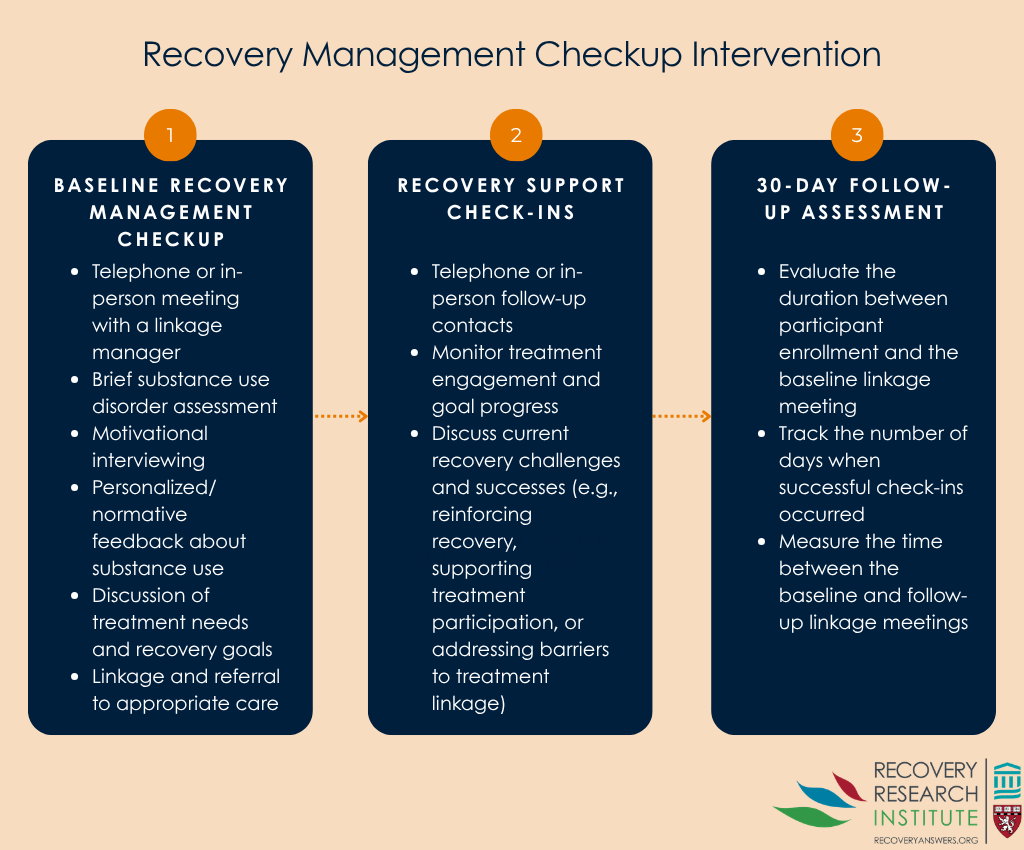
This was a convergent mixed methods study — a research design in which both qualitative and quantitative data are collected, analyzed, and then integrated to draw overall conclusions. Data for this study were collected from a Midwestern federally qualified health center after completion of the authors’ prior clinical trial. Federally Qualified Health Centers, or FQHCs, are community clinics that receive federal funding to provide comprehensive primary care in underserved areas. Prior to implementing the intervention, personnel screened patients attending primary care visits for substance use disorder to estimate the potential need for referral services. Participants were recruited from a pool of patients attending an initial substance use disorder treatment appointment, at which time they were informed about the study and consented by a linkage manager. At the beginning of the study visit, linkage managers completed a brief substance use disorder assessment then moved directly to the intervention. During this time, linkage managers used Recovery Management Checkup procedures, including Motivational Interviewing techniques with personalized feedback, to problem solve potential treatment barriers and help link patients to care. Following this visit, linkage managers regularly checked in with patients over 30 days (e.g., via telephone) to determine treatment engagement. A separate focus group of health center staff was later conducted to determine what impacted the implementation of the intervention. See graphic below describing the study intervention and approach.
Quantitative outcomes of this study were rates of positive substance use disorder screening among patients and comparisons between clinical and research linkage managers, including differences in rate of successful meeting completion and days between baseline and follow-up linkage meetings. Qualitative outcomes included an assessment of linkage manager’s Motivational Interviewing performance. In addition, the study analyzed transcript data from a focus group with the health center’s director of behavioral health, quality nurse manager, a substance use screener, and the health center linkage manager to assess factors related to intervention implementation.
The goal of these analyses was to identify barriers and facilitators to implementing the Recovery Management Checkup intervention within a health center setting and assess differences between clinical and research linkage manager intervention delivery. However, given that the intervention, check-in, and follow-up procedures were condensed from the originally designed 12-month timeframe to 30 days, it seems likely that the study could not assess all the relevant factors impacting intervention implementation. As such, results should be considered preliminary; further research is needed to better determine how to implement Recovery Management Checkup interventions in primary care settings.
WHAT DID THIS STUDY FIND?
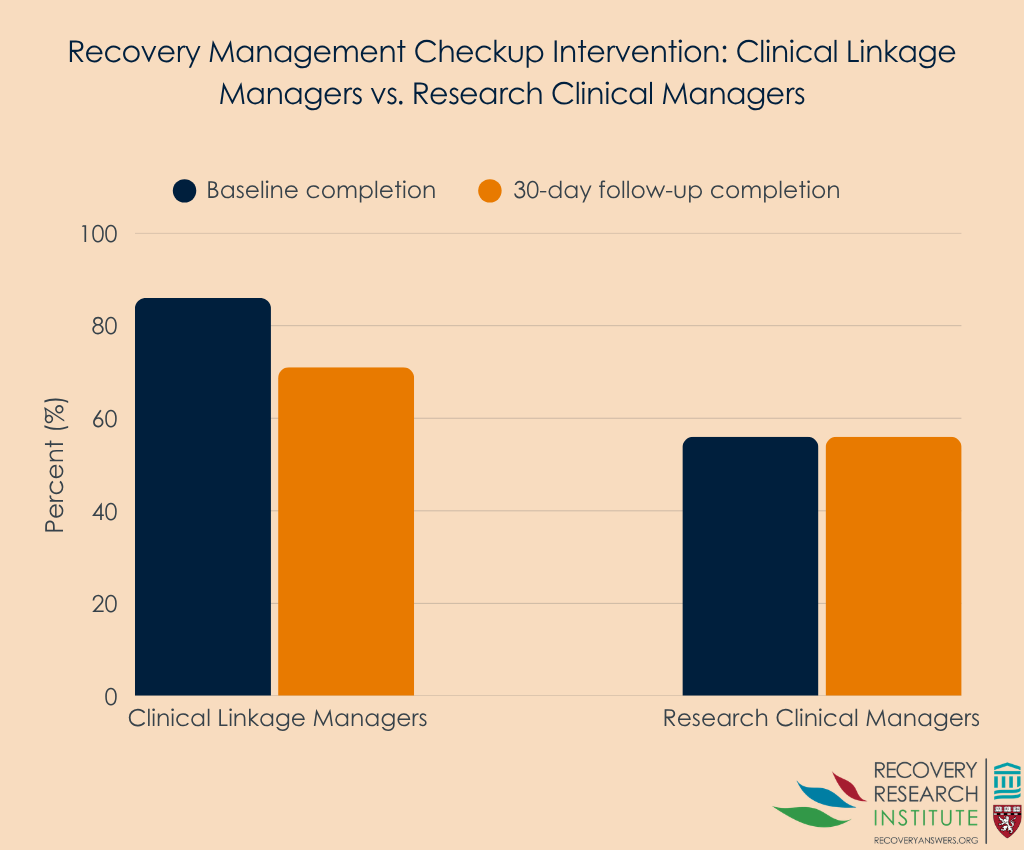
Half of primary care patients screened positive for moderate to high risk for substance use disorder, suggesting that referral services were warranted. As shown in the graph below, clinical linkage managers had a higher baseline completion rate (86%) and 30-day follow-up completion rate (71%) than the research clinical manager (56% and 56% respectively). Analysis of baseline assessment discussions further showed differences between linkage managers: the research linkage manager consistently asked follow-up questions after patient responses to specific measures, while the clinical linkage manager displayed better adherence to motivational interviewing principles (such as compassion and acceptance) during meetings.
Analysis of focus group data showed that the intervention was in line with the mission of the health center and patients expressed a desire for linkage services. However numerous systemic and financial barriers made the intervention difficult to implement. Some notable challenges included a lack of technological infrastructure to implement screening into electronic medical records, intervention procedures being incompatible with clinical workflow, and intervention services not being billable, making reimbursement impossible.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study shows how challenging it can be to integrate behavioral health interventions into federally qualified health centers. Although the study suggests both a need for linkage services (half of sampled patients screened positive for moderate/high risk for substance use disorder) and patient buy-in for such services, the realities of providing care make treatment implementation difficult. Such barriers can reduce the effectiveness of an intervention. For instance, study procedures were designed to be administered over 12 months but were condensed to 30 days, limiting patient exposure to the intervention and limiting the study’s ability to assess the full intervention. Additionally, due to issues integrating screening measures into electronic systems, the study was only able to recruit patients who were already attending an initial substance use disorder treatment visit. This sampling approach does not reflect the intended intervention context (primary care visits), making findings less directly generalizable to the target population. Such issues underscore historical gaps between substance use intervention research and practice, which make intervention implementation challenging: highly controlled research contexts do not necessarily reflect the priorities of providers or the environments in which they work. Critically, the current work outlines such challenges and suggests that providing support (for example, financial and technical) to health centers may help ease clinical burden and improve intervention implementation. Further implementation work is needed to determine optimal support strategies for federally qualified health centers.
BOTTOM LINE
Patients receiving care at federally qualified health centers may benefit from integrating Recovery Management Checkup interventions into routine care. Effectively implementing such programs, however, requires substantial financial, technical, and workflow support.
- For individuals and families seeking recovery: Screening and referral to treatment for people with substance use disorders is critical for recovery. The program described here can potentially help support those in need of care access it and receive continued support while in recovery.
- For treatment professionals and treatment systems: This study suggests that there is a need to link patients at federally qualified health centers to substance use disorder treatment. Integrating screening, brief intervention, and referral to treatment practices into routine care, while also following these patients over time as is done in Recovery Management Checkups, could help ensure patients receive the help they need.
- For scientists: The Recovery Management Checkup intervention shows clinical promise but may be difficult to integrate into primary care settings. It is critical for scientists to research appropriate implementation strategies and work with providers to better understand how interventions may need to be tailored to accommodate the realities of providing care.
- For policy makers: This study underscores the need for funding mechanisms that support substance use screening, linkage, and ongoing care coordination in federally qualified health centers. Supporting operational costs and intervention integration may facilitate integration of evidence-based interventions into routine practice.
CITATIONS
Watson, D. P., Singh, R., Taylor, L., Dennis, M. L., Grella, C. E., Johnstone, C., Browne, K., & Saldana, L. (2024). Exploring the feasibility of recovery management checkups for primary care in a federally qualified health center. Frontiers in Public Health, 12. doi: 10.3389/fpubh.2024.1443409.