WHAT PROBLEM DOES THIS STUDY ADDRESS?
As time in recovery increases, the likelihood of improvements in health, wellbeing, and life milestones such as career advancement and education also tends to grow. While the likelihood of relapse decreases over time as the brain heals, readapts, and recalibrates and elements of recovery capital increase, risk for relapse and disorder recurrence remains. Understanding the challenges that can put people at risk for relapse even after several years or decades in recovery is an important but understudied area of recovery science. By uncovering and documenting the factors that might precipitate long-term relapse risk, research can inform clinical disease management strategies. This can empower clinicians to inquire about the presence of various warning signs before people have once again become symptomatic, hopefully allowing for risk mitigation strategies to be implemented.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study recruited 50 adults who met DSM-5 criteria for a lifetime history of alcohol use disorder, were abstinent or in remission for the previous 90 days, and had experienced a recurrence of alcohol use disorder within the past 5 years after at least 1 year of full sustained remission. Participants first completed an online survey that collected information on demographics, substance use history, mental health diagnoses, treatment experiences, participation in 12-step or other mutual help organizations, recovery support services, and use of online resources or social networking sites. Each participant then completed a semi-structured interview that inquired about any biological/health, social, psychological, and treatment and recovery support service usage changes that occurred in the year prior to the relapse. Then, for each factor identified as contributing to relapse, participants estimated when exactly during that year prior to the relapse the change began and rated the extent to which they believed it contributed to their relapse (i.e., “did not contribute”, “possibly contributed”, “probably contributed”, or “definitely contributed”). At the end of the interview, participants were also asked to identify what they believed was the single most important reason for their relapse.
WHAT DID THIS STUDY FIND?
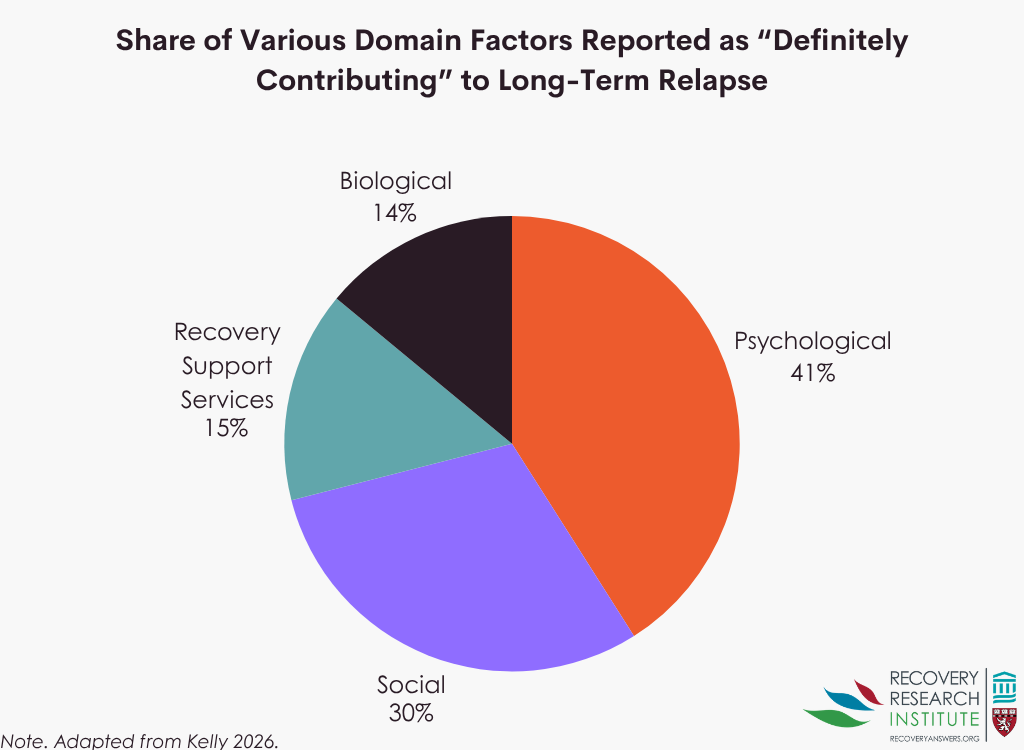
Participants who had experienced sustained remission from anywhere from 1 year to 23 years prior to relapse identified 26 factors that changed in the year prior to relapse across biological, psychological, social, and recovery support service domains. As shown in the graph below, among factors rated as “definitely contributing” to relapse, psychological factors accounted for the largest proportion (41%), followed by social (30%), recovery support services (15%), and biological factors (14%).
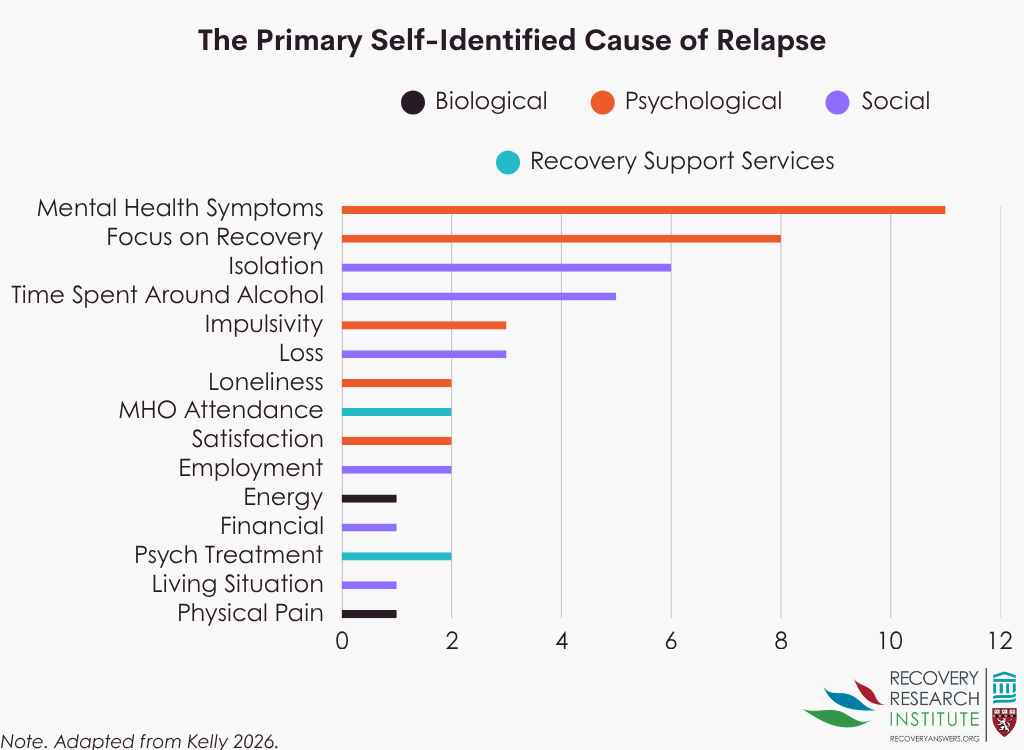
Across all factors and levels of contribution to relapse, reduced focus on recovery and low energy were the most commonly reported contributors, followed by mental health symptoms, sleep problems, loneliness, and isolation. Reduced focus on recovery also had the highest proportion of participants identifying it as definitely contributing to relapse, followed by physical pain, mental health symptoms, and impulsivity. Although the timing of specific factors and domain trajectories varied across participants, there was a general pattern of factors gradually emerging in the months leading up to relapse. When asked to identify the single most important reason for their relapse, as shown in the graph below, participants most often reported mental health symptoms (n = 11), followed by reduced focus on recovery (n = 8).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Most treatment and recovery research and theory have focused primarily on the early stages of recovery. These early stages of stabilization typically are associated with conditioned cue reactivity (i.e., the triggers of “people, places, and things”) and neurophysiological dysregulation which settles down over the first year as deconditioning occurs and the central nervous system becomes reaccustomed to the absence of the drug. Little has been documented in theory or research about contributors to long-term relapse following years of remission. Such precursors may have more to do with stress, coping, and self-regulation capabilities than the more commonly noted neurobiological challenges. Hence, individuals in long-term remission from alcohol use disorder may benefit from different supports than those in early recovery. This study found that a wide range of factors across multiple life domains were perceived to contribute to long-term relapse, and the frequency, potency, and timing of these factors varied across individuals. A consistent theme was a reduced focus on recovery as an important precursor to relapse as well as management of mental health symptoms such as anxiety and mood. Although many individuals experience improvements in health, wellbeing, and life circumstances over time, the competing demands of even positive life events can shift attention away from recovery and introduce new stressors (e.g., getting promoted in a job and having to move to new city). These findings provide the first empirical checklist of remission-based warning signs and symptoms that may be important to identify in order to help reduce long-term relapse risk. Such a list can help sensitize and empower clinicians working in long-term disease management to take action in collaboration with patients to mitigate such risks and help prevent recurrence of alcohol use disorder.
BOTTOM LINE
The factors contributing to relapse after long-term remission may differ from those in early recovery and vary across individuals. Sustaining recovery may require continued recovery prioritization and identification of bio-psycho-social and recovery support services changes so that effective risk mitigation strategies can be undertaken.
- For individuals and families seeking recovery: Even after many years of recovery, continuing to prioritize recovery-supportive behaviors and staying aware of the risks noted in this study may help support ongoing recovery.
- For treatment professionals and treatment systems: Identifying risk factors for relapse is important across early, sustained, and stable stages of recovery. However, the nature of the specific risks and their relative impact may vary across these stages and between individuals. The findings from this study suggest that regularly reviewing these documented bio-psycho-social and treatment and recovery support service use changes, with patients in remission may help alert patients to emerging risks and help support ongoing recovery. Highlighting both the prevalence and perceived impact of these factors among others in recovery may also encourage continued awareness and vigilance. The researchers also developed a checklist (https://www.frontiersin.org/articles/10.3389/fpubh.2025.1706192/full#supplementary-material) that could be used within recovery support services to help identify and monitor for these potential relapse risks.
- For scientists: Recovery is increasingly conceptualized as a dynamic process, which requires a better understanding of recovery trajectories over time. This study contributes to the literature by identifying relapse risks and the perceived potency of those risks among individuals who relapsed after at least 1 year of alcohol use disorder remission. The identified factors varied in frequency, perceived impact, and timing prior to relapse. Future research could examine these factors prospectively rather than relying on retrospective recall, although a methodological challenge in such designs will be the influence of “assessment reactivity”, where asking about relapse risks over time is likely to alert patients to those very risks and lead to aversive action to mitigate those risks. Additional work could also explore whether similar patterns emerge across other substance use disorders, such as cannabis, opioid, or stimulant use disorder.
- For policy makers: Increased funding for recovery support services that assist individuals across different stages of recovery may help improve outcomes for adults recovering from alcohol use disorder. The findings from this study highlight specific factors, such as mental health symptoms and reduced focus on recovery, that were associated with long-term relapse among adults. Expanding payment for long-term disease management services using checklists such as the one developed in this study, could help empower clinicians to identify sobriety-based warning signs and prevent long-term relapse and disorder recurrence. In turn, this is likely to substantially decrease the disease and economic burden attributable to substance use disorders across different societies.
CITATIONS
Kelly, J. F., Klein, M., Zeng, K., Manske, S., & Abry, A. (2026). Long-term relapse: Markers, mechanisms, and implications for disease management in alcohol use disorder. Frontiers in Public Health, 13. doi: 10.3389/fpubh.2025.1706192.
Note. The study’s author, John F. Kelly, serves as the director of the Recovery Research Institute.












