Cultural barriers to treatment: Differences between Latino and White Americans
Latino Americans with alcohol use disorder are less likely to attend treatment than White Americans. To inform strategies that address this disparity, this study examined whether beliefs that would interfere with getting specialty care for alcohol use disorder were more common in Latino compared to White individuals.
To date, research on the reasons why Latino Americans are less likely to receive specialty alcohol use disorder treatment has been mixed. Surveys suggest that logistical barriers (e.g., difficulties finding treatment, or obtaining childcare) may be one reason why Latino Americans are less likely to seek out treatment compared to White Americans. However, other research contradicts these findings. The reasons for disparities in treatment utilization are made more unclear by evidence that other issues may contribute to observed treatment disparities. Qualitative research, for example, suggests that low perceived treatment need (e.g., not believing treatment was necessary), low perceived treatment efficacy (e.g., not believing treatment would be helpful), cultural barriers (e.g., perceptions that treatment providers lack familiarity with Latino culture), and incongruent recovery goals (e.g., individual goals of reducing but not abstaining from alcohol) were all reasons cited by Latino participants for not pursuing alcohol treatment. In addition, Latino Americans described how stigma towards substance use treatment (e.g., concerns of peer/family judgment due to pursuing treatment) deterred them from seeking care.
It is important to further investigate sex differences in barriers to alcohol treatment among Latino/as to better understand how to reach these populations. To inform strategies that address potential treatment seeking disparities for Latino Americans with alcohol use disorder, this study investigated differences in beliefs about treatment between Latino and White Americans by gender recruited from a national sample of US adults.
HOW WAS THIS STUDY CONDUCTED?
This study was a quantitative cross-sectional descriptive survey in a nationally representative sample of White and Latino US adults. The primary goal of this research was to determine the unique barriers to specialty alcohol use disorder treatment endorsed by Latino Americans using a validated survey measure. The study also examined how endorsement of barriers varied across participants’ birth sex (i.e., males and females). Descriptive statistics and multivariable models were used to characterize the outcome of endorsed treatment barriers.
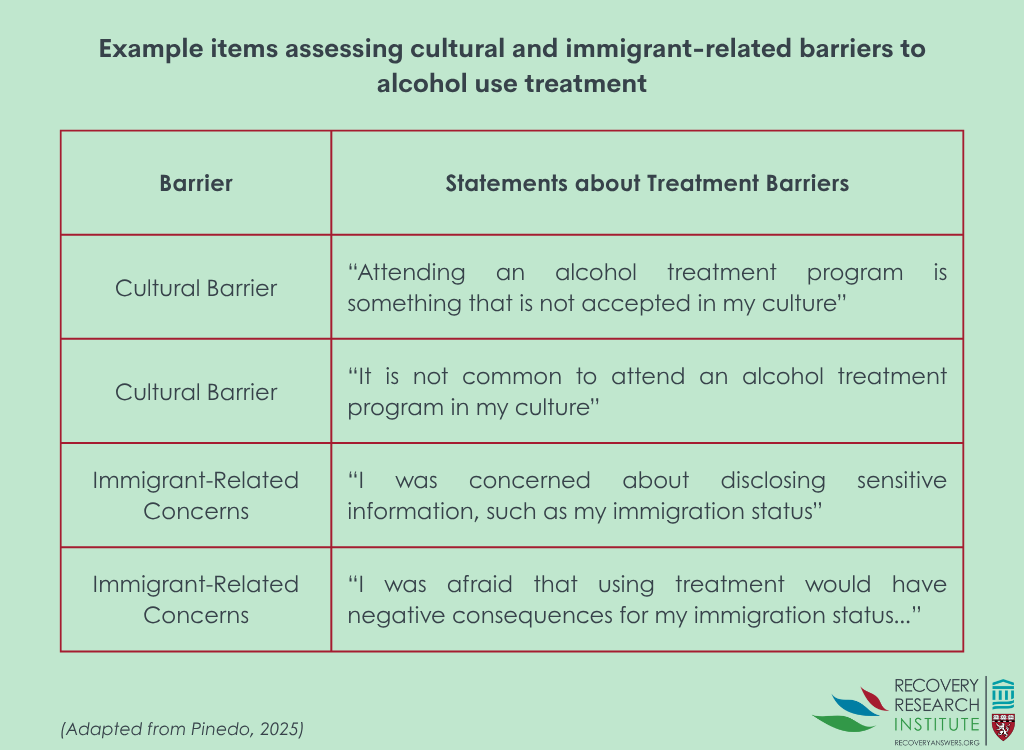
The primary outcomes of the present study were the assessment of perceived barriers to specialty alcohol use disorder treatment in Latino vs. White individuals on the Barriers to Specialty Alcohol Treatment Scale. The Barriers to Specialty Alcohol Treatment Scale is a 36-item survey measure that was designed to capture a wide array of barriers to specialty alcohol treatment not assessed by previous instruments. This measure was informed by previous quantitative and qualitative research to assess barriers especially relevant to Latino Americans. See Graphic below for example items.
Respondents indicate via a 5-point Likert scale ranging from (1) strongly disagree to (5) strongly agree the degree to which each barrier to treatment personally impacted them. The scale consists of items across 7 domains including low problem recognition (e.g., “I didn’t feel I had a drinking problem”), incongruent recovery goals (e.g., “I wanted to reduce my drinking but not stop completely”), low perceived treatment efficacy (e.g., “I didn’t think treatment would be helpful for me because alcohol treatment is not effective”), cultural concerns (e.g., “Attending an alcohol treatment is something that is not accepted in my culture”), immigration-related concerns (e.g., “I was afraid that using treatment would have negative consequences for the immigration status of someone in my family, like my parents or children”), perceived lack of social support (e.g., “I was afraid of being rejected going to treatment”), and logistical barriers to treatment (“My health insurance didn’t cover alcohol treatment”).
The present study utilized a pre-existing nationally representative web panel with ~2 million members. For the current study, randomly selected panel members were invited to complete a brief screener to determine their eligibility to participate. Eligible participants were: (1) adults (i.e., 18+ years of age), who (2) identified as White or of Latino racial/ethnic descent, and (3) met diagnostic criteria for alcohol use disorder via criteria outlined in the DSM-5 within the past 5 years. Recruitment minimums were used to ensure an equal proportion of participants across ethnicity and sex.
The study sample included 1200 participants evenly distributed across sex and ethnicity (i.e., the sample included 300 Latinos, 300 Latinas, 300 White males and 300 White females). The study did not use weights to provide unbiased estimates of US adults as is typical for representative samples; therefore, the current findings should not be considered representative of all US adults, even though participants were randomly selected from a larger representative sample. Participants in the sample were on average 34 years old. Most participants (60%) did not have a college degree, were employed (75%), and had an annual income of ≥$50,000 (55%). Most participants (82%) reported having health insurance. Most of the participants (88%) were born in the US, however, more Latino Americans reported being born outside the US compared to White Americans (80% vs. 97% respectively). On average, participants reported 4 alcohol use disorder symptoms consistent with moderate alcohol use disorder. However, most participants (71%) did not report receiving any specialty alcohol use disorder treatment in the past 5 years.
WHAT DID THIS STUDY FIND?
Latino Americans had higher levels of perceived barriers to treatment than White Americans
Latino Americans were more likely to endorse 22 out of 36 barriers to specialty alcohol treatment. These included logistical, cultural, and social support-related barriers to care. In contrast, White individuals did not have any barriers to treatment with which they agreed more than Latino individuals.
Adjusting for whether someone was foreign or US born, gender, age, household income, health insurance status, and treatment use in the past 5 years to isolate the independent associations between barriers and Latino vs. White ethnicity, 9 barriers had higher levels among Latinos. These included beliefs that treatment was not effective, discomfort communicating in English, concerns that treatment would impact participants’ immigration status, and beliefs that providers were from a different culture (e.g., providers would not understand the participant’s cultural background). For every 1 point in the direction of higher levels of the perceived barrier (e.g., agree vs. neutral or strongly agree vs. agree), participants were 25-50% more likely to identify as Latino than White.
No differences in specialty treatment barriers were found by sex
When the authors compared rates of specialty treatment barrier endorsement, they found that there were no differences between Latinos and Latinas.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings showed that Latino Americans with alcohol use disorders may face unique barriers to specialty alcohol treatment compared to White Americans. As might be expected given their unique cultural experiences, Latino Americans were more likely to report that concerns about cultural differences between themselves and their providers, discomfort communicating in English, and the potential impact treatment may have on themselves or their loved ones’ immigration status than White Americans. In addition, however, they also endorsed higher levels not thinking treatment will work because it is ineffective. Taken together, these results may indicate that Latino Americans with alcohol use disorders face unique challenges to specialty alcohol care.
The present results suggest that tailoring specialty alcohol treatment programs to better reflect the needs/experiences of Latino Americans may increase Latino Americans’ treatment seeking. Given that Latino American participants unilaterally cited a perceived cultural mismatch between themselves and providers as a barrier to care this would likely be a strong intervention point by which to facilitate treatment seeking among those in need. This is supported by research demonstrating that incorporating important aspects of Latino American culture can be effective at engaging and retaining Latino adults in treatment. Alternatively, efforts to merely acknowledge the lived experiences of Latino patients (e.g., immigration challenges) could be enough to improve treatment engagement. Research shows that such acknowledgment may produce better treatment outcomes than relying on a “one size fits all” approach that is agnostic to the lived reality of being a Latino American who also has a substance use disorder. That said, it is unknown why Latino Americans perceived specialty alcohol treatment as being less effective than White Americans. It could be that Latinos are more skeptical of medical explanations and treatments for mental health more generally, of which alcohol use disorder treatment is only one type. It is also possible that Latino American participants may have had negative interactions with providers previously who lacked cultural competence/humility which negatively impacted their treatment. This is somewhat supported by research suggesting that a lack of cultural competence/humility among providers results in worse behavioral outcomes among patients. Future research is needed to replicate and explicate this interesting and potentially important finding.
Although the survey recruited individuals from a large web-based sample representative of US adults, they did not use weights needed to provide a true representative set of findings. Therefore, it is possible that the results lack generalizability to the general population of those with an alcohol use disorder. That said, there is evidence that utilizing non-probability samples can yield valid results when working with difficult to recruit populations. Caution should be made interpreting these findings beyond the current study.
In a similar vein, it is unclear how generalizable these results are to Latino Americans who are less acculturated to US culture. Although proportionally more Latino Americans reported being born outside the US (20%) compared to White Americans (3%) the majority were nevertheless native-born Americans. Additionally, although the authors do not explicitly state as such, it is assumed that all participants completed the study survey in English. Therefore, it is unclear how applicable the identified barriers to specialty alcohol treatment may be for those who were less ingrained in American culture (e.g., those who could not read English). It is plausible that barriers related to cultural differences between patients and providers described may be even more pronounced among such Latino Americans, but it is beyond the scope of these data to indicate this. Future research on the unique barriers to treatment experienced by less acculturated Latino Americans is needed.
The current study only captured participants’ self-reported sex (male or female). Therefore, it is unclear how reported barriers may vary across more granular measures of sex/gender. This is relevant as the social forces acting upon people’s intersecting racial/ethnic and gender identities can result in unique constellation of barriers to care. Future studies should consider how gender identity among Latino Americans with alcohol use disorders may also influence specialty treatment seeking.
BOTTOM LINE
Latino Americans with alcohol use disorders face unique challenges to specialty alcohol care. They endorsed beliefs that treatment was not effective, discomfort communicating in English, concerns that treatment would impact their own or their loved ones’ immigration status, and beliefs that providers were not culturally competent. Although the present study did not explore why such differences were found, it is possible that Latino individuals had a general skepticism regarding medical explanations and treatments for mental health or previous negative experiences with providers. It is critical for more research to be conducted to investigate possible reasons why such treatment barriers exist and how they can be overcome.
For individuals and families seeking recovery: Latino Americans with alcohol use disorders face unique barriers to specialty alcohol care relative to White Americans. Individuals and families seeking recovery from alcohol use disorder should be aware of such potential barriers to accessing treatment. It is important for those seeking recovery for themselves or others to be aware of potential options which may facilitate treatment. For example, searching for providers who are bilingual and/or who are nested within Latino cultural enclaves. The Substance Abuse and Mental Health Services Administration national helpline is available in Spanish which can help those who unable/uncomfortable communicating in English find the help they need.
For treatment professionals and treatment systems: Latino Americans may perceive specialty alcohol treatment as ineffective and have misgivings about providers’ potential misunderstanding of their worldviews. Therefore, it may be beneficial for treatment professionals and those working with Latino American populations with alcohol use disorders to modify their practices to be more accommodating/welcoming to Latino Americans. For example, this could be done by incorporating bilingual services (e.g., having Spanish versions of patient intake forms, employing bilingual staff, etc.) and hiring Latino American providers. Additionally, given concerns about the impact of treatment on immigration status, treatment systems should provide clear information about confidentiality (e.g., protected health information).
For scientists: Scientists would do well to prioritize research that centers the lived experiences and structural challenges faced by Latino Americans. Future studies should explore how cultural, linguistic, and immigration-related factors influence perceptions of and access to alcohol treatment. Given that many Latino Americans in the current study cited a cultural mismatch with providers as a barrier to care there is also a need to research the effectiveness of culturally tailored interventions for reasons of both engagement and efficacy. Scientists should also consider mixed methods approaches to better capture the nuanced reasons behind low treatment utilization (e.g., due to stigma and fear of legal consequences). It is vital for researchers to identify actionable strategies for improving equity in treatment access and outcomes.
For policy makers: The present study may indicate that systemic barriers (e.g., a lack of culturally competent providers) are a deterrent for Latino Americans seeking specialty alcohol use treatment. Therefore, it is imperative for policymakers to consider potential solutions to improve access to such care for Latino Americans. For example, policies which support workforce development initiatives that train providers in how to practice cultural competency/humility in care and incentivize the hiring of bilingual professionals. Such efforts could improve treatment utilization and engagement among Latino Americans. Additionally, policymakers could strengthen confidentiality protections to ensure the safety of undocumented patients.
To date, research on the reasons why Latino Americans are less likely to receive specialty alcohol use disorder treatment has been mixed. Surveys suggest that logistical barriers (e.g., difficulties finding treatment, or obtaining childcare) may be one reason why Latino Americans are less likely to seek out treatment compared to White Americans. However, other research contradicts these findings. The reasons for disparities in treatment utilization are made more unclear by evidence that other issues may contribute to observed treatment disparities. Qualitative research, for example, suggests that low perceived treatment need (e.g., not believing treatment was necessary), low perceived treatment efficacy (e.g., not believing treatment would be helpful), cultural barriers (e.g., perceptions that treatment providers lack familiarity with Latino culture), and incongruent recovery goals (e.g., individual goals of reducing but not abstaining from alcohol) were all reasons cited by Latino participants for not pursuing alcohol treatment. In addition, Latino Americans described how stigma towards substance use treatment (e.g., concerns of peer/family judgment due to pursuing treatment) deterred them from seeking care.
It is important to further investigate sex differences in barriers to alcohol treatment among Latino/as to better understand how to reach these populations. To inform strategies that address potential treatment seeking disparities for Latino Americans with alcohol use disorder, this study investigated differences in beliefs about treatment between Latino and White Americans by gender recruited from a national sample of US adults.
HOW WAS THIS STUDY CONDUCTED?
This study was a quantitative cross-sectional descriptive survey in a nationally representative sample of White and Latino US adults. The primary goal of this research was to determine the unique barriers to specialty alcohol use disorder treatment endorsed by Latino Americans using a validated survey measure. The study also examined how endorsement of barriers varied across participants’ birth sex (i.e., males and females). Descriptive statistics and multivariable models were used to characterize the outcome of endorsed treatment barriers.
The primary outcomes of the present study were the assessment of perceived barriers to specialty alcohol use disorder treatment in Latino vs. White individuals on the Barriers to Specialty Alcohol Treatment Scale. The Barriers to Specialty Alcohol Treatment Scale is a 36-item survey measure that was designed to capture a wide array of barriers to specialty alcohol treatment not assessed by previous instruments. This measure was informed by previous quantitative and qualitative research to assess barriers especially relevant to Latino Americans. See Graphic below for example items.
Respondents indicate via a 5-point Likert scale ranging from (1) strongly disagree to (5) strongly agree the degree to which each barrier to treatment personally impacted them. The scale consists of items across 7 domains including low problem recognition (e.g., “I didn’t feel I had a drinking problem”), incongruent recovery goals (e.g., “I wanted to reduce my drinking but not stop completely”), low perceived treatment efficacy (e.g., “I didn’t think treatment would be helpful for me because alcohol treatment is not effective”), cultural concerns (e.g., “Attending an alcohol treatment is something that is not accepted in my culture”), immigration-related concerns (e.g., “I was afraid that using treatment would have negative consequences for the immigration status of someone in my family, like my parents or children”), perceived lack of social support (e.g., “I was afraid of being rejected going to treatment”), and logistical barriers to treatment (“My health insurance didn’t cover alcohol treatment”).
The present study utilized a pre-existing nationally representative web panel with ~2 million members. For the current study, randomly selected panel members were invited to complete a brief screener to determine their eligibility to participate. Eligible participants were: (1) adults (i.e., 18+ years of age), who (2) identified as White or of Latino racial/ethnic descent, and (3) met diagnostic criteria for alcohol use disorder via criteria outlined in the DSM-5 within the past 5 years. Recruitment minimums were used to ensure an equal proportion of participants across ethnicity and sex.
The study sample included 1200 participants evenly distributed across sex and ethnicity (i.e., the sample included 300 Latinos, 300 Latinas, 300 White males and 300 White females). The study did not use weights to provide unbiased estimates of US adults as is typical for representative samples; therefore, the current findings should not be considered representative of all US adults, even though participants were randomly selected from a larger representative sample. Participants in the sample were on average 34 years old. Most participants (60%) did not have a college degree, were employed (75%), and had an annual income of ≥$50,000 (55%). Most participants (82%) reported having health insurance. Most of the participants (88%) were born in the US, however, more Latino Americans reported being born outside the US compared to White Americans (80% vs. 97% respectively). On average, participants reported 4 alcohol use disorder symptoms consistent with moderate alcohol use disorder. However, most participants (71%) did not report receiving any specialty alcohol use disorder treatment in the past 5 years.
WHAT DID THIS STUDY FIND?
Latino Americans had higher levels of perceived barriers to treatment than White Americans
Latino Americans were more likely to endorse 22 out of 36 barriers to specialty alcohol treatment. These included logistical, cultural, and social support-related barriers to care. In contrast, White individuals did not have any barriers to treatment with which they agreed more than Latino individuals.
Adjusting for whether someone was foreign or US born, gender, age, household income, health insurance status, and treatment use in the past 5 years to isolate the independent associations between barriers and Latino vs. White ethnicity, 9 barriers had higher levels among Latinos. These included beliefs that treatment was not effective, discomfort communicating in English, concerns that treatment would impact participants’ immigration status, and beliefs that providers were from a different culture (e.g., providers would not understand the participant’s cultural background). For every 1 point in the direction of higher levels of the perceived barrier (e.g., agree vs. neutral or strongly agree vs. agree), participants were 25-50% more likely to identify as Latino than White.
No differences in specialty treatment barriers were found by sex
When the authors compared rates of specialty treatment barrier endorsement, they found that there were no differences between Latinos and Latinas.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings showed that Latino Americans with alcohol use disorders may face unique barriers to specialty alcohol treatment compared to White Americans. As might be expected given their unique cultural experiences, Latino Americans were more likely to report that concerns about cultural differences between themselves and their providers, discomfort communicating in English, and the potential impact treatment may have on themselves or their loved ones’ immigration status than White Americans. In addition, however, they also endorsed higher levels not thinking treatment will work because it is ineffective. Taken together, these results may indicate that Latino Americans with alcohol use disorders face unique challenges to specialty alcohol care.
The present results suggest that tailoring specialty alcohol treatment programs to better reflect the needs/experiences of Latino Americans may increase Latino Americans’ treatment seeking. Given that Latino American participants unilaterally cited a perceived cultural mismatch between themselves and providers as a barrier to care this would likely be a strong intervention point by which to facilitate treatment seeking among those in need. This is supported by research demonstrating that incorporating important aspects of Latino American culture can be effective at engaging and retaining Latino adults in treatment. Alternatively, efforts to merely acknowledge the lived experiences of Latino patients (e.g., immigration challenges) could be enough to improve treatment engagement. Research shows that such acknowledgment may produce better treatment outcomes than relying on a “one size fits all” approach that is agnostic to the lived reality of being a Latino American who also has a substance use disorder. That said, it is unknown why Latino Americans perceived specialty alcohol treatment as being less effective than White Americans. It could be that Latinos are more skeptical of medical explanations and treatments for mental health more generally, of which alcohol use disorder treatment is only one type. It is also possible that Latino American participants may have had negative interactions with providers previously who lacked cultural competence/humility which negatively impacted their treatment. This is somewhat supported by research suggesting that a lack of cultural competence/humility among providers results in worse behavioral outcomes among patients. Future research is needed to replicate and explicate this interesting and potentially important finding.
Although the survey recruited individuals from a large web-based sample representative of US adults, they did not use weights needed to provide a true representative set of findings. Therefore, it is possible that the results lack generalizability to the general population of those with an alcohol use disorder. That said, there is evidence that utilizing non-probability samples can yield valid results when working with difficult to recruit populations. Caution should be made interpreting these findings beyond the current study.
In a similar vein, it is unclear how generalizable these results are to Latino Americans who are less acculturated to US culture. Although proportionally more Latino Americans reported being born outside the US (20%) compared to White Americans (3%) the majority were nevertheless native-born Americans. Additionally, although the authors do not explicitly state as such, it is assumed that all participants completed the study survey in English. Therefore, it is unclear how applicable the identified barriers to specialty alcohol treatment may be for those who were less ingrained in American culture (e.g., those who could not read English). It is plausible that barriers related to cultural differences between patients and providers described may be even more pronounced among such Latino Americans, but it is beyond the scope of these data to indicate this. Future research on the unique barriers to treatment experienced by less acculturated Latino Americans is needed.
The current study only captured participants’ self-reported sex (male or female). Therefore, it is unclear how reported barriers may vary across more granular measures of sex/gender. This is relevant as the social forces acting upon people’s intersecting racial/ethnic and gender identities can result in unique constellation of barriers to care. Future studies should consider how gender identity among Latino Americans with alcohol use disorders may also influence specialty treatment seeking.
BOTTOM LINE
Latino Americans with alcohol use disorders face unique challenges to specialty alcohol care. They endorsed beliefs that treatment was not effective, discomfort communicating in English, concerns that treatment would impact their own or their loved ones’ immigration status, and beliefs that providers were not culturally competent. Although the present study did not explore why such differences were found, it is possible that Latino individuals had a general skepticism regarding medical explanations and treatments for mental health or previous negative experiences with providers. It is critical for more research to be conducted to investigate possible reasons why such treatment barriers exist and how they can be overcome.
For individuals and families seeking recovery: Latino Americans with alcohol use disorders face unique barriers to specialty alcohol care relative to White Americans. Individuals and families seeking recovery from alcohol use disorder should be aware of such potential barriers to accessing treatment. It is important for those seeking recovery for themselves or others to be aware of potential options which may facilitate treatment. For example, searching for providers who are bilingual and/or who are nested within Latino cultural enclaves. The Substance Abuse and Mental Health Services Administration national helpline is available in Spanish which can help those who unable/uncomfortable communicating in English find the help they need.
For treatment professionals and treatment systems: Latino Americans may perceive specialty alcohol treatment as ineffective and have misgivings about providers’ potential misunderstanding of their worldviews. Therefore, it may be beneficial for treatment professionals and those working with Latino American populations with alcohol use disorders to modify their practices to be more accommodating/welcoming to Latino Americans. For example, this could be done by incorporating bilingual services (e.g., having Spanish versions of patient intake forms, employing bilingual staff, etc.) and hiring Latino American providers. Additionally, given concerns about the impact of treatment on immigration status, treatment systems should provide clear information about confidentiality (e.g., protected health information).
For scientists: Scientists would do well to prioritize research that centers the lived experiences and structural challenges faced by Latino Americans. Future studies should explore how cultural, linguistic, and immigration-related factors influence perceptions of and access to alcohol treatment. Given that many Latino Americans in the current study cited a cultural mismatch with providers as a barrier to care there is also a need to research the effectiveness of culturally tailored interventions for reasons of both engagement and efficacy. Scientists should also consider mixed methods approaches to better capture the nuanced reasons behind low treatment utilization (e.g., due to stigma and fear of legal consequences). It is vital for researchers to identify actionable strategies for improving equity in treatment access and outcomes.
For policy makers: The present study may indicate that systemic barriers (e.g., a lack of culturally competent providers) are a deterrent for Latino Americans seeking specialty alcohol use treatment. Therefore, it is imperative for policymakers to consider potential solutions to improve access to such care for Latino Americans. For example, policies which support workforce development initiatives that train providers in how to practice cultural competency/humility in care and incentivize the hiring of bilingual professionals. Such efforts could improve treatment utilization and engagement among Latino Americans. Additionally, policymakers could strengthen confidentiality protections to ensure the safety of undocumented patients.
To date, research on the reasons why Latino Americans are less likely to receive specialty alcohol use disorder treatment has been mixed. Surveys suggest that logistical barriers (e.g., difficulties finding treatment, or obtaining childcare) may be one reason why Latino Americans are less likely to seek out treatment compared to White Americans. However, other research contradicts these findings. The reasons for disparities in treatment utilization are made more unclear by evidence that other issues may contribute to observed treatment disparities. Qualitative research, for example, suggests that low perceived treatment need (e.g., not believing treatment was necessary), low perceived treatment efficacy (e.g., not believing treatment would be helpful), cultural barriers (e.g., perceptions that treatment providers lack familiarity with Latino culture), and incongruent recovery goals (e.g., individual goals of reducing but not abstaining from alcohol) were all reasons cited by Latino participants for not pursuing alcohol treatment. In addition, Latino Americans described how stigma towards substance use treatment (e.g., concerns of peer/family judgment due to pursuing treatment) deterred them from seeking care.
It is important to further investigate sex differences in barriers to alcohol treatment among Latino/as to better understand how to reach these populations. To inform strategies that address potential treatment seeking disparities for Latino Americans with alcohol use disorder, this study investigated differences in beliefs about treatment between Latino and White Americans by gender recruited from a national sample of US adults.
HOW WAS THIS STUDY CONDUCTED?
This study was a quantitative cross-sectional descriptive survey in a nationally representative sample of White and Latino US adults. The primary goal of this research was to determine the unique barriers to specialty alcohol use disorder treatment endorsed by Latino Americans using a validated survey measure. The study also examined how endorsement of barriers varied across participants’ birth sex (i.e., males and females). Descriptive statistics and multivariable models were used to characterize the outcome of endorsed treatment barriers.
The primary outcomes of the present study were the assessment of perceived barriers to specialty alcohol use disorder treatment in Latino vs. White individuals on the Barriers to Specialty Alcohol Treatment Scale. The Barriers to Specialty Alcohol Treatment Scale is a 36-item survey measure that was designed to capture a wide array of barriers to specialty alcohol treatment not assessed by previous instruments. This measure was informed by previous quantitative and qualitative research to assess barriers especially relevant to Latino Americans. See Graphic below for example items.
Respondents indicate via a 5-point Likert scale ranging from (1) strongly disagree to (5) strongly agree the degree to which each barrier to treatment personally impacted them. The scale consists of items across 7 domains including low problem recognition (e.g., “I didn’t feel I had a drinking problem”), incongruent recovery goals (e.g., “I wanted to reduce my drinking but not stop completely”), low perceived treatment efficacy (e.g., “I didn’t think treatment would be helpful for me because alcohol treatment is not effective”), cultural concerns (e.g., “Attending an alcohol treatment is something that is not accepted in my culture”), immigration-related concerns (e.g., “I was afraid that using treatment would have negative consequences for the immigration status of someone in my family, like my parents or children”), perceived lack of social support (e.g., “I was afraid of being rejected going to treatment”), and logistical barriers to treatment (“My health insurance didn’t cover alcohol treatment”).
The present study utilized a pre-existing nationally representative web panel with ~2 million members. For the current study, randomly selected panel members were invited to complete a brief screener to determine their eligibility to participate. Eligible participants were: (1) adults (i.e., 18+ years of age), who (2) identified as White or of Latino racial/ethnic descent, and (3) met diagnostic criteria for alcohol use disorder via criteria outlined in the DSM-5 within the past 5 years. Recruitment minimums were used to ensure an equal proportion of participants across ethnicity and sex.
The study sample included 1200 participants evenly distributed across sex and ethnicity (i.e., the sample included 300 Latinos, 300 Latinas, 300 White males and 300 White females). The study did not use weights to provide unbiased estimates of US adults as is typical for representative samples; therefore, the current findings should not be considered representative of all US adults, even though participants were randomly selected from a larger representative sample. Participants in the sample were on average 34 years old. Most participants (60%) did not have a college degree, were employed (75%), and had an annual income of ≥$50,000 (55%). Most participants (82%) reported having health insurance. Most of the participants (88%) were born in the US, however, more Latino Americans reported being born outside the US compared to White Americans (80% vs. 97% respectively). On average, participants reported 4 alcohol use disorder symptoms consistent with moderate alcohol use disorder. However, most participants (71%) did not report receiving any specialty alcohol use disorder treatment in the past 5 years.
WHAT DID THIS STUDY FIND?
Latino Americans had higher levels of perceived barriers to treatment than White Americans
Latino Americans were more likely to endorse 22 out of 36 barriers to specialty alcohol treatment. These included logistical, cultural, and social support-related barriers to care. In contrast, White individuals did not have any barriers to treatment with which they agreed more than Latino individuals.
Adjusting for whether someone was foreign or US born, gender, age, household income, health insurance status, and treatment use in the past 5 years to isolate the independent associations between barriers and Latino vs. White ethnicity, 9 barriers had higher levels among Latinos. These included beliefs that treatment was not effective, discomfort communicating in English, concerns that treatment would impact participants’ immigration status, and beliefs that providers were from a different culture (e.g., providers would not understand the participant’s cultural background). For every 1 point in the direction of higher levels of the perceived barrier (e.g., agree vs. neutral or strongly agree vs. agree), participants were 25-50% more likely to identify as Latino than White.
No differences in specialty treatment barriers were found by sex
When the authors compared rates of specialty treatment barrier endorsement, they found that there were no differences between Latinos and Latinas.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Findings showed that Latino Americans with alcohol use disorders may face unique barriers to specialty alcohol treatment compared to White Americans. As might be expected given their unique cultural experiences, Latino Americans were more likely to report that concerns about cultural differences between themselves and their providers, discomfort communicating in English, and the potential impact treatment may have on themselves or their loved ones’ immigration status than White Americans. In addition, however, they also endorsed higher levels not thinking treatment will work because it is ineffective. Taken together, these results may indicate that Latino Americans with alcohol use disorders face unique challenges to specialty alcohol care.
The present results suggest that tailoring specialty alcohol treatment programs to better reflect the needs/experiences of Latino Americans may increase Latino Americans’ treatment seeking. Given that Latino American participants unilaterally cited a perceived cultural mismatch between themselves and providers as a barrier to care this would likely be a strong intervention point by which to facilitate treatment seeking among those in need. This is supported by research demonstrating that incorporating important aspects of Latino American culture can be effective at engaging and retaining Latino adults in treatment. Alternatively, efforts to merely acknowledge the lived experiences of Latino patients (e.g., immigration challenges) could be enough to improve treatment engagement. Research shows that such acknowledgment may produce better treatment outcomes than relying on a “one size fits all” approach that is agnostic to the lived reality of being a Latino American who also has a substance use disorder. That said, it is unknown why Latino Americans perceived specialty alcohol treatment as being less effective than White Americans. It could be that Latinos are more skeptical of medical explanations and treatments for mental health more generally, of which alcohol use disorder treatment is only one type. It is also possible that Latino American participants may have had negative interactions with providers previously who lacked cultural competence/humility which negatively impacted their treatment. This is somewhat supported by research suggesting that a lack of cultural competence/humility among providers results in worse behavioral outcomes among patients. Future research is needed to replicate and explicate this interesting and potentially important finding.
Although the survey recruited individuals from a large web-based sample representative of US adults, they did not use weights needed to provide a true representative set of findings. Therefore, it is possible that the results lack generalizability to the general population of those with an alcohol use disorder. That said, there is evidence that utilizing non-probability samples can yield valid results when working with difficult to recruit populations. Caution should be made interpreting these findings beyond the current study.
In a similar vein, it is unclear how generalizable these results are to Latino Americans who are less acculturated to US culture. Although proportionally more Latino Americans reported being born outside the US (20%) compared to White Americans (3%) the majority were nevertheless native-born Americans. Additionally, although the authors do not explicitly state as such, it is assumed that all participants completed the study survey in English. Therefore, it is unclear how applicable the identified barriers to specialty alcohol treatment may be for those who were less ingrained in American culture (e.g., those who could not read English). It is plausible that barriers related to cultural differences between patients and providers described may be even more pronounced among such Latino Americans, but it is beyond the scope of these data to indicate this. Future research on the unique barriers to treatment experienced by less acculturated Latino Americans is needed.
The current study only captured participants’ self-reported sex (male or female). Therefore, it is unclear how reported barriers may vary across more granular measures of sex/gender. This is relevant as the social forces acting upon people’s intersecting racial/ethnic and gender identities can result in unique constellation of barriers to care. Future studies should consider how gender identity among Latino Americans with alcohol use disorders may also influence specialty treatment seeking.
BOTTOM LINE
Latino Americans with alcohol use disorders face unique challenges to specialty alcohol care. They endorsed beliefs that treatment was not effective, discomfort communicating in English, concerns that treatment would impact their own or their loved ones’ immigration status, and beliefs that providers were not culturally competent. Although the present study did not explore why such differences were found, it is possible that Latino individuals had a general skepticism regarding medical explanations and treatments for mental health or previous negative experiences with providers. It is critical for more research to be conducted to investigate possible reasons why such treatment barriers exist and how they can be overcome.
For individuals and families seeking recovery: Latino Americans with alcohol use disorders face unique barriers to specialty alcohol care relative to White Americans. Individuals and families seeking recovery from alcohol use disorder should be aware of such potential barriers to accessing treatment. It is important for those seeking recovery for themselves or others to be aware of potential options which may facilitate treatment. For example, searching for providers who are bilingual and/or who are nested within Latino cultural enclaves. The Substance Abuse and Mental Health Services Administration national helpline is available in Spanish which can help those who unable/uncomfortable communicating in English find the help they need.
For treatment professionals and treatment systems: Latino Americans may perceive specialty alcohol treatment as ineffective and have misgivings about providers’ potential misunderstanding of their worldviews. Therefore, it may be beneficial for treatment professionals and those working with Latino American populations with alcohol use disorders to modify their practices to be more accommodating/welcoming to Latino Americans. For example, this could be done by incorporating bilingual services (e.g., having Spanish versions of patient intake forms, employing bilingual staff, etc.) and hiring Latino American providers. Additionally, given concerns about the impact of treatment on immigration status, treatment systems should provide clear information about confidentiality (e.g., protected health information).
For scientists: Scientists would do well to prioritize research that centers the lived experiences and structural challenges faced by Latino Americans. Future studies should explore how cultural, linguistic, and immigration-related factors influence perceptions of and access to alcohol treatment. Given that many Latino Americans in the current study cited a cultural mismatch with providers as a barrier to care there is also a need to research the effectiveness of culturally tailored interventions for reasons of both engagement and efficacy. Scientists should also consider mixed methods approaches to better capture the nuanced reasons behind low treatment utilization (e.g., due to stigma and fear of legal consequences). It is vital for researchers to identify actionable strategies for improving equity in treatment access and outcomes.
For policy makers: The present study may indicate that systemic barriers (e.g., a lack of culturally competent providers) are a deterrent for Latino Americans seeking specialty alcohol use treatment. Therefore, it is imperative for policymakers to consider potential solutions to improve access to such care for Latino Americans. For example, policies which support workforce development initiatives that train providers in how to practice cultural competency/humility in care and incentivize the hiring of bilingual professionals. Such efforts could improve treatment utilization and engagement among Latino Americans. Additionally, policymakers could strengthen confidentiality protections to ensure the safety of undocumented patients.