Attitudes toward Narcan among people who use drugs
Widespread distribution of naloxone (also referred to by the brand name Narcan) can help prevent overdose and save lives. Because quick administration is key, naloxone attitudes among those most likely to administer it, including people who are present and also using drugs, may help explain how likely someone is to administer it. This study examined attitudes toward naloxone in a sample of people who use drugs.
People who use drugs are often witnesses to overdoses. Therefore, distributing naloxone (i.e., overdose reversal) among this group is a priority. However, acceptance remains limited—even when naloxone is free or low-cost—due perhaps to stigma. Stigma refers to socially discrediting attitudes towards a particular characteristic, behavior, or condition. The use of naloxone may be stigmatized by those who believe that it helps people avoid negative consequences thereby “enabling” continued drug use. This is an example of “intervention stigma,” or negative beliefs about evidence-based interventions. These beliefs are common not only among the general public but also among healthcare providers and emergency responders, potentially affecting how people talk about naloxone, how it is disseminated, and whether people use it. This study investigated stigmatizing beliefs among key stakeholders in the use of naloxone: people who use drugs.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed baseline data from 293 individuals who participated in a digital intervention which was designed to provide support for adults receiving treatment for substance use disorder. Baseline measures included stigma towards naloxone, stigma towards medications for opioid use disorder, overdose history, number of recovery attempts, past 30-day substance use, current use of medication for opioid use disorder, and current mental health difficulties including depression and anxiety.
The study characterized naloxone stigma overall and by group across demographic, psychosocial, substance use, and mental health factors. Next, the study examined the association between stigma towards naloxone and stigma towards medications for opioid use disorder while making statistical adjustments for age, gender, race, education, lifetime overdose, and opioid versus nonopioid misuse. Such statistical adjustments help to isolate the effect of interest – i.e., whether naloxone stigma is independently related to medication stigma.
Participants were recruited from treatment programs, recovery housing, criminal legal settings, and emergency rooms. The sample were mostly older than age 31 years (82%), White (75%), currently unemployed (64%), living in unstable housing (67.5%), and reported opioid misuse (58%). Most had an educational level of high school or beyond (78.2%) and more than half identified as cisgender women (53.9%). Note, “cisgender woman” describes people who are assigned female sex at birth and identify their gender as woman.
WHAT DID THIS STUDY FIND?
Some held stigmatizing beliefs toward naloxone
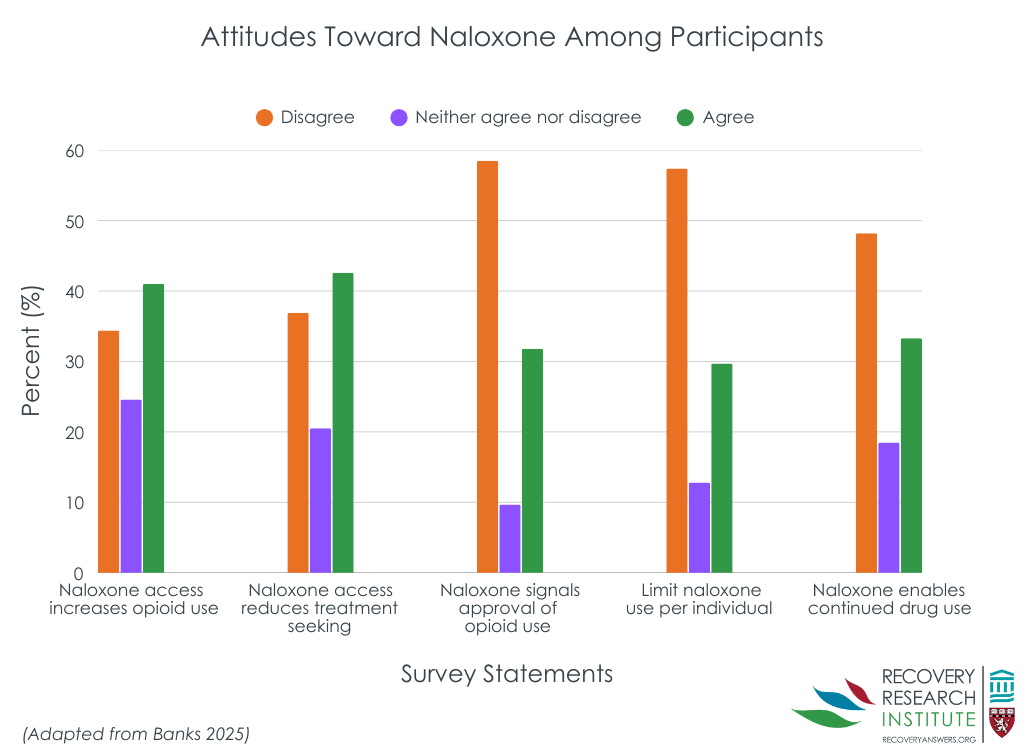
One in 3 participants agreed with beliefs that access to naloxone leads to more opioid use and less treatment seeking and that naloxone “is enabling” people who use drugs. Other responses varied in agreement (see Figure below).
There were group differences on specific stigma items
There were no demographic differences found using the total score for naloxone stigma, however, an item level analysis revealed some key differences. In response to, “There should be a limit on the number of times one person receives naloxone to reverse an overdose,” 2/3 of White people disagreed compared to a little more than half of people of color.
On the item “Opioid users will use more opioids if they know they have access to naloxone,” women were more likely than men to to disagree (39% vs. 29%) or agree (29% vs. 20%), while men were more likely to be unsure or neutral (51% vs. 32%).
Other factors associated with stigma were identified. More naloxone stigma was endorsed by those with nonopioid drug misuse, without prior overdose, and those with fewer recovery attempts compared to their counterparts. Similar trends were observed when predicting stigma towards medication for opioid use disorder: opioid misuse, prior overdose, and use of medication for opioid use disorder were negatively associated with medication stigma.
Stigma toward naloxone and medications were related
The association between stigma towards naloxone and stigma towards medications for opioid use disorder was of medium strength. The only other significant predictor of medication stigma was lifetime overdose, which remained negatively associated with stigma towards medication for opioid use disorder. This means as the number of overdoses increased, stigma towards medications decreased.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The most common stigmatizing beliefs toward naloxone were 1) that the overdose antidote enabled or increased drug use and 2) that it decreased treatment-seeking. Similar to findings from emergency responders, perceptions that supporting naloxone equated to condoning drug use or that naloxone administration should have a limit were less commonly endorsed. Compared with professional groups, people who use drugs reported more naloxone stigma. This highlights the importance of including this group in strategies to increase widespread deployment of naloxone. Because more experience with overdose and recovery was associated with less stigmatizing beliefs toward naloxone, trainings might leverage peers with more experience to deliver the intervention to those with less experience.
Although responses to substance use in the US have been shifting from a criminal justice response to public health centered models, the shift has not applied equally to all groups. Minoritized individuals may themselves hold more stigmatizing attitudes toward substance use disorders, shaped by lived experiences of disproportionate punishment and messaging that frames addiction as a moral failing rather than a health condition.
Women had more polarized views in that they were more likely to both disagree and agree with the idea that naloxone access leads to increased opioid use, with fewer sitting on the fence, while men were more likely to be neutral. This suggests gender differences in how people perceive harm reduction resources like naloxone, possibly shaped by different personal experiences, exposure to harm reduction messaging, or societal roles in caregiving and health advocacy. The unique experiences of women in this regard are noteworthy given previous research has shown they are more likely than men to be blamed for their opioid related impairment.
Finally, this study is one of the first to empirically link stigma toward naloxone and medications for opioid use disorder. This implies that existing stigma interventions for naloxone could also target stigma towards medications for opioid use disorder.
Some of the sample sizes in the comparisons were small; thus, the degree to which these findings replicate to larger samples is unknown.
The race/ethnicity of the non-White group of participants is unknown. Therefore, the degree to which these findings generalize to individuals identified as Asian, Native American, Black/African American, and other is not clear.
BOTTOM LINE
This study examined barriers to naloxone deployment in people who use drugs, specifically the role of stigmatizing beliefs. One-third of participants endorsed felt naloxone enabled or increased drug use and decreased treatment-seeking – presumably by reducing the impact of negative consequences which can enhance motivation for change. Non-White participants were slightly more likely to feel there should be a limit on the number of times one person receives naloxone to reverse an overdose compared to White participants. The ways criminal justice responses to opioid use disorder have disproportionately impacting minority communities may explain this finding. Women endorsed more split views (i.e., both greater agreement and disagreement) compared to men on whether naloxone access leads to increased opioid use. More research on gender differences among those who use drugs is warranted. Overdose education and naloxone distribution specifically for people who use drugs may help address these stigmatizing beliefs and ultimately increase the use of naloxone during overdose events.
For individuals and families seeking recovery: Individuals who use drugs may have stigmatizing (i.e., discrediting) beliefs toward naloxone and medications for opioid use disorder. Increasing evidence-based knowledge while addressing the lived experiences of people who use drugs may empower people who use drugs as community contributors while increasing the ready availability and use of naloxone during overdose events.
For treatment professionals and treatment systems: This study examined naloxone stigma among people who use drugs. Findings emphasize the potential role of overdose education and naloxone distribution among those earlier in the substance use disorder course and should include those who use opioids as well as those who do not use opioids, as both groups may be bystanders to opioid-related overdose events.
For scientists: This study examined naloxone stigma among people who use drugs and medications for opioid use disorder. Measures that differentiate the nature and magnitude of stigma based on medication types, routes of administration, and personal and professional characteristics are needed to understand the impact of stigma and inform solutions to alleviate them. Research may also help to develop and test naloxone education specifically designed for people who use drugs.
For policy makers: Despite its efficacy and safety, people may have stigmatizing beliefs toward naloxone. This study found that more experience with overdose and recovery are associated with less naloxone stigma among people who use drugs. Trainings specifically designed for people who use drugs may improve attitudes toward naloxone in this important stakeholder group, potentially increasing the likelihood that they will use naloxone as bystanders to overdose events.
People who use drugs are often witnesses to overdoses. Therefore, distributing naloxone (i.e., overdose reversal) among this group is a priority. However, acceptance remains limited—even when naloxone is free or low-cost—due perhaps to stigma. Stigma refers to socially discrediting attitudes towards a particular characteristic, behavior, or condition. The use of naloxone may be stigmatized by those who believe that it helps people avoid negative consequences thereby “enabling” continued drug use. This is an example of “intervention stigma,” or negative beliefs about evidence-based interventions. These beliefs are common not only among the general public but also among healthcare providers and emergency responders, potentially affecting how people talk about naloxone, how it is disseminated, and whether people use it. This study investigated stigmatizing beliefs among key stakeholders in the use of naloxone: people who use drugs.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed baseline data from 293 individuals who participated in a digital intervention which was designed to provide support for adults receiving treatment for substance use disorder. Baseline measures included stigma towards naloxone, stigma towards medications for opioid use disorder, overdose history, number of recovery attempts, past 30-day substance use, current use of medication for opioid use disorder, and current mental health difficulties including depression and anxiety.
The study characterized naloxone stigma overall and by group across demographic, psychosocial, substance use, and mental health factors. Next, the study examined the association between stigma towards naloxone and stigma towards medications for opioid use disorder while making statistical adjustments for age, gender, race, education, lifetime overdose, and opioid versus nonopioid misuse. Such statistical adjustments help to isolate the effect of interest – i.e., whether naloxone stigma is independently related to medication stigma.
Participants were recruited from treatment programs, recovery housing, criminal legal settings, and emergency rooms. The sample were mostly older than age 31 years (82%), White (75%), currently unemployed (64%), living in unstable housing (67.5%), and reported opioid misuse (58%). Most had an educational level of high school or beyond (78.2%) and more than half identified as cisgender women (53.9%). Note, “cisgender woman” describes people who are assigned female sex at birth and identify their gender as woman.
WHAT DID THIS STUDY FIND?
Some held stigmatizing beliefs toward naloxone
One in 3 participants agreed with beliefs that access to naloxone leads to more opioid use and less treatment seeking and that naloxone “is enabling” people who use drugs. Other responses varied in agreement (see Figure below).
There were group differences on specific stigma items
There were no demographic differences found using the total score for naloxone stigma, however, an item level analysis revealed some key differences. In response to, “There should be a limit on the number of times one person receives naloxone to reverse an overdose,” 2/3 of White people disagreed compared to a little more than half of people of color.
On the item “Opioid users will use more opioids if they know they have access to naloxone,” women were more likely than men to to disagree (39% vs. 29%) or agree (29% vs. 20%), while men were more likely to be unsure or neutral (51% vs. 32%).
Other factors associated with stigma were identified. More naloxone stigma was endorsed by those with nonopioid drug misuse, without prior overdose, and those with fewer recovery attempts compared to their counterparts. Similar trends were observed when predicting stigma towards medication for opioid use disorder: opioid misuse, prior overdose, and use of medication for opioid use disorder were negatively associated with medication stigma.
Stigma toward naloxone and medications were related
The association between stigma towards naloxone and stigma towards medications for opioid use disorder was of medium strength. The only other significant predictor of medication stigma was lifetime overdose, which remained negatively associated with stigma towards medication for opioid use disorder. This means as the number of overdoses increased, stigma towards medications decreased.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The most common stigmatizing beliefs toward naloxone were 1) that the overdose antidote enabled or increased drug use and 2) that it decreased treatment-seeking. Similar to findings from emergency responders, perceptions that supporting naloxone equated to condoning drug use or that naloxone administration should have a limit were less commonly endorsed. Compared with professional groups, people who use drugs reported more naloxone stigma. This highlights the importance of including this group in strategies to increase widespread deployment of naloxone. Because more experience with overdose and recovery was associated with less stigmatizing beliefs toward naloxone, trainings might leverage peers with more experience to deliver the intervention to those with less experience.
Although responses to substance use in the US have been shifting from a criminal justice response to public health centered models, the shift has not applied equally to all groups. Minoritized individuals may themselves hold more stigmatizing attitudes toward substance use disorders, shaped by lived experiences of disproportionate punishment and messaging that frames addiction as a moral failing rather than a health condition.
Women had more polarized views in that they were more likely to both disagree and agree with the idea that naloxone access leads to increased opioid use, with fewer sitting on the fence, while men were more likely to be neutral. This suggests gender differences in how people perceive harm reduction resources like naloxone, possibly shaped by different personal experiences, exposure to harm reduction messaging, or societal roles in caregiving and health advocacy. The unique experiences of women in this regard are noteworthy given previous research has shown they are more likely than men to be blamed for their opioid related impairment.
Finally, this study is one of the first to empirically link stigma toward naloxone and medications for opioid use disorder. This implies that existing stigma interventions for naloxone could also target stigma towards medications for opioid use disorder.
Some of the sample sizes in the comparisons were small; thus, the degree to which these findings replicate to larger samples is unknown.
The race/ethnicity of the non-White group of participants is unknown. Therefore, the degree to which these findings generalize to individuals identified as Asian, Native American, Black/African American, and other is not clear.
BOTTOM LINE
This study examined barriers to naloxone deployment in people who use drugs, specifically the role of stigmatizing beliefs. One-third of participants endorsed felt naloxone enabled or increased drug use and decreased treatment-seeking – presumably by reducing the impact of negative consequences which can enhance motivation for change. Non-White participants were slightly more likely to feel there should be a limit on the number of times one person receives naloxone to reverse an overdose compared to White participants. The ways criminal justice responses to opioid use disorder have disproportionately impacting minority communities may explain this finding. Women endorsed more split views (i.e., both greater agreement and disagreement) compared to men on whether naloxone access leads to increased opioid use. More research on gender differences among those who use drugs is warranted. Overdose education and naloxone distribution specifically for people who use drugs may help address these stigmatizing beliefs and ultimately increase the use of naloxone during overdose events.
For individuals and families seeking recovery: Individuals who use drugs may have stigmatizing (i.e., discrediting) beliefs toward naloxone and medications for opioid use disorder. Increasing evidence-based knowledge while addressing the lived experiences of people who use drugs may empower people who use drugs as community contributors while increasing the ready availability and use of naloxone during overdose events.
For treatment professionals and treatment systems: This study examined naloxone stigma among people who use drugs. Findings emphasize the potential role of overdose education and naloxone distribution among those earlier in the substance use disorder course and should include those who use opioids as well as those who do not use opioids, as both groups may be bystanders to opioid-related overdose events.
For scientists: This study examined naloxone stigma among people who use drugs and medications for opioid use disorder. Measures that differentiate the nature and magnitude of stigma based on medication types, routes of administration, and personal and professional characteristics are needed to understand the impact of stigma and inform solutions to alleviate them. Research may also help to develop and test naloxone education specifically designed for people who use drugs.
For policy makers: Despite its efficacy and safety, people may have stigmatizing beliefs toward naloxone. This study found that more experience with overdose and recovery are associated with less naloxone stigma among people who use drugs. Trainings specifically designed for people who use drugs may improve attitudes toward naloxone in this important stakeholder group, potentially increasing the likelihood that they will use naloxone as bystanders to overdose events.
People who use drugs are often witnesses to overdoses. Therefore, distributing naloxone (i.e., overdose reversal) among this group is a priority. However, acceptance remains limited—even when naloxone is free or low-cost—due perhaps to stigma. Stigma refers to socially discrediting attitudes towards a particular characteristic, behavior, or condition. The use of naloxone may be stigmatized by those who believe that it helps people avoid negative consequences thereby “enabling” continued drug use. This is an example of “intervention stigma,” or negative beliefs about evidence-based interventions. These beliefs are common not only among the general public but also among healthcare providers and emergency responders, potentially affecting how people talk about naloxone, how it is disseminated, and whether people use it. This study investigated stigmatizing beliefs among key stakeholders in the use of naloxone: people who use drugs.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed baseline data from 293 individuals who participated in a digital intervention which was designed to provide support for adults receiving treatment for substance use disorder. Baseline measures included stigma towards naloxone, stigma towards medications for opioid use disorder, overdose history, number of recovery attempts, past 30-day substance use, current use of medication for opioid use disorder, and current mental health difficulties including depression and anxiety.
The study characterized naloxone stigma overall and by group across demographic, psychosocial, substance use, and mental health factors. Next, the study examined the association between stigma towards naloxone and stigma towards medications for opioid use disorder while making statistical adjustments for age, gender, race, education, lifetime overdose, and opioid versus nonopioid misuse. Such statistical adjustments help to isolate the effect of interest – i.e., whether naloxone stigma is independently related to medication stigma.
Participants were recruited from treatment programs, recovery housing, criminal legal settings, and emergency rooms. The sample were mostly older than age 31 years (82%), White (75%), currently unemployed (64%), living in unstable housing (67.5%), and reported opioid misuse (58%). Most had an educational level of high school or beyond (78.2%) and more than half identified as cisgender women (53.9%). Note, “cisgender woman” describes people who are assigned female sex at birth and identify their gender as woman.
WHAT DID THIS STUDY FIND?
Some held stigmatizing beliefs toward naloxone
One in 3 participants agreed with beliefs that access to naloxone leads to more opioid use and less treatment seeking and that naloxone “is enabling” people who use drugs. Other responses varied in agreement (see Figure below).
There were group differences on specific stigma items
There were no demographic differences found using the total score for naloxone stigma, however, an item level analysis revealed some key differences. In response to, “There should be a limit on the number of times one person receives naloxone to reverse an overdose,” 2/3 of White people disagreed compared to a little more than half of people of color.
On the item “Opioid users will use more opioids if they know they have access to naloxone,” women were more likely than men to to disagree (39% vs. 29%) or agree (29% vs. 20%), while men were more likely to be unsure or neutral (51% vs. 32%).
Other factors associated with stigma were identified. More naloxone stigma was endorsed by those with nonopioid drug misuse, without prior overdose, and those with fewer recovery attempts compared to their counterparts. Similar trends were observed when predicting stigma towards medication for opioid use disorder: opioid misuse, prior overdose, and use of medication for opioid use disorder were negatively associated with medication stigma.
Stigma toward naloxone and medications were related
The association between stigma towards naloxone and stigma towards medications for opioid use disorder was of medium strength. The only other significant predictor of medication stigma was lifetime overdose, which remained negatively associated with stigma towards medication for opioid use disorder. This means as the number of overdoses increased, stigma towards medications decreased.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The most common stigmatizing beliefs toward naloxone were 1) that the overdose antidote enabled or increased drug use and 2) that it decreased treatment-seeking. Similar to findings from emergency responders, perceptions that supporting naloxone equated to condoning drug use or that naloxone administration should have a limit were less commonly endorsed. Compared with professional groups, people who use drugs reported more naloxone stigma. This highlights the importance of including this group in strategies to increase widespread deployment of naloxone. Because more experience with overdose and recovery was associated with less stigmatizing beliefs toward naloxone, trainings might leverage peers with more experience to deliver the intervention to those with less experience.
Although responses to substance use in the US have been shifting from a criminal justice response to public health centered models, the shift has not applied equally to all groups. Minoritized individuals may themselves hold more stigmatizing attitudes toward substance use disorders, shaped by lived experiences of disproportionate punishment and messaging that frames addiction as a moral failing rather than a health condition.
Women had more polarized views in that they were more likely to both disagree and agree with the idea that naloxone access leads to increased opioid use, with fewer sitting on the fence, while men were more likely to be neutral. This suggests gender differences in how people perceive harm reduction resources like naloxone, possibly shaped by different personal experiences, exposure to harm reduction messaging, or societal roles in caregiving and health advocacy. The unique experiences of women in this regard are noteworthy given previous research has shown they are more likely than men to be blamed for their opioid related impairment.
Finally, this study is one of the first to empirically link stigma toward naloxone and medications for opioid use disorder. This implies that existing stigma interventions for naloxone could also target stigma towards medications for opioid use disorder.
Some of the sample sizes in the comparisons were small; thus, the degree to which these findings replicate to larger samples is unknown.
The race/ethnicity of the non-White group of participants is unknown. Therefore, the degree to which these findings generalize to individuals identified as Asian, Native American, Black/African American, and other is not clear.
BOTTOM LINE
This study examined barriers to naloxone deployment in people who use drugs, specifically the role of stigmatizing beliefs. One-third of participants endorsed felt naloxone enabled or increased drug use and decreased treatment-seeking – presumably by reducing the impact of negative consequences which can enhance motivation for change. Non-White participants were slightly more likely to feel there should be a limit on the number of times one person receives naloxone to reverse an overdose compared to White participants. The ways criminal justice responses to opioid use disorder have disproportionately impacting minority communities may explain this finding. Women endorsed more split views (i.e., both greater agreement and disagreement) compared to men on whether naloxone access leads to increased opioid use. More research on gender differences among those who use drugs is warranted. Overdose education and naloxone distribution specifically for people who use drugs may help address these stigmatizing beliefs and ultimately increase the use of naloxone during overdose events.
For individuals and families seeking recovery: Individuals who use drugs may have stigmatizing (i.e., discrediting) beliefs toward naloxone and medications for opioid use disorder. Increasing evidence-based knowledge while addressing the lived experiences of people who use drugs may empower people who use drugs as community contributors while increasing the ready availability and use of naloxone during overdose events.
For treatment professionals and treatment systems: This study examined naloxone stigma among people who use drugs. Findings emphasize the potential role of overdose education and naloxone distribution among those earlier in the substance use disorder course and should include those who use opioids as well as those who do not use opioids, as both groups may be bystanders to opioid-related overdose events.
For scientists: This study examined naloxone stigma among people who use drugs and medications for opioid use disorder. Measures that differentiate the nature and magnitude of stigma based on medication types, routes of administration, and personal and professional characteristics are needed to understand the impact of stigma and inform solutions to alleviate them. Research may also help to develop and test naloxone education specifically designed for people who use drugs.
For policy makers: Despite its efficacy and safety, people may have stigmatizing beliefs toward naloxone. This study found that more experience with overdose and recovery are associated with less naloxone stigma among people who use drugs. Trainings specifically designed for people who use drugs may improve attitudes toward naloxone in this important stakeholder group, potentially increasing the likelihood that they will use naloxone as bystanders to overdose events.