Body weight and risk of death in opioid medication treatment
Opioid agonist medications like methadone and buprenorphine can lead to weight gain and even obesity, which can bring with it a host of health challenges including premature death. This study examined the effects of being either underweight or obese on risk of death during buprenorphine and methadone treatment.
Chronic repeated use of illicit opioids like heroin and fentanyl can reduce appetite. Resulting malnutrition can compromise bone health and immune system function. Addressing nutritional health when patients present for opioid use disorder treatment is often an essential component of holistic recovery. In addition to providing medication treatments like methadone and buprenorphine, opioid use disorder treatment programs may offer patients information about healthy lifestyle changes such as nutritional intake to promote improvements in health and well-being.
At the same time, weight gain and increased body mass index (BMI) – a common way of measuring health-limiting levels of body fat – are potential side effects of agonist medication treatments for opioid use disorder. Individuals receiving methadone treatment, for example, are more likely to be overweight and obese relative to the general population, with about 3/4 of patients being overweight.
There are likely many reasons underlying this weight gain. For example, underweight patients may be encouraged by healthcare providers and treatment staff to gain weight during the initial stages of treatment, which could lead to excessive weight gain over time. In addition, dysregulated reward systems may contribute to comfort eating to provide feelings of reward in the absence of a person’s drug of choice. Chronic exposure to illicit opioids and opioid agonist treatments like methadone can also lead to heightened preferences for foods with high sugar content. Indeed, individuals receiving methadone are shown to increase consumption of sugary foods and beverages throughout the course of treatment. Methadone itself can also cause increased appetite and reduced metabolism, further contributing to overeating and weight gain.
Obesity comes with risk of morbidity and mortality, independent of opioid use disorder. Thus, it is essential to better understand this increased risk of weight gain during opioid use disorder medication treatment and its effect on patient outcomes. Though weight gain is common during medication treatment, the relationship between weight gain and mortality risk during medication treatment is not entirely clear and few studies have included patients receiving both methadone and buprenorphine treatment. This study aimed to address this gap by assessing the relationship between weight and risk of death among individuals receiving methadone or buprenorphine treatment for opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a retrospective case–control study of the relationship between body weight and mortality risk for adults receiving opioid agonist medication treatment. The authors examined government data collected at addiction treatment facilities in two regions of England (i.e. Derbyshire & Teesside). The analysis included living patients (n = 1,574) who received opioid agonist treatment (buprenorphine or methadone) between 2022 and 2023, as well as deceased patients (n = 233) who were receiving opioid agonist treatment at the time of their death between 2015 and 2023.
Variables included BMI (for determining whether a person was overweight, underweight, or healthy weight), age, opioid agonist treatment type and dose, smoking status, and residence in a deprived region of England (determined with residential zip codes of patients and assessing factors like income, employment, education, and crime in that region). Causes of death were also assessed for deceased patients. Body weight was evaluated as BMI, determined with measures of height and weight obtained at patients’ most recent treatment service appointments (for deceased patients, this was collected at their last attended appointment prior to death). BMIs of ≤15 are considered underweight and indexes of 16 – 24 are considered healthy weight. BMIs of 25 are considered overweight and those of 30 and greater are considered “obese”. Causes of death were determined from coroner reports, which only included unnatural and unexpected deaths (n = 202/233 deaths included in analyses of mortality cause). Less than 2% of patients were excluded from analyses because they opted out of data sharing for research purposes. Nineteen percent of deceased patients had missing data for smoking status.
The study’s primary focus was on 1) the relationship between weight and mortality among patients receiving buprenorphine or methadone (n=1807) controlling statistically for age, gender, medication type and dose, regional socioeconomic status (i.e., “deprivation” index), and smoking status; and (2) the weight and mortality specifically among patients receiving methadone and for whom methadone dose was available in the dataset (n=1562) adjusting also for these same factors (apart from medication type/dose). They also examined the role of other variables of interest like age and gender (see variables of interest above).
WHAT DID THIS STUDY FIND?
Deceased patients had higher BMI
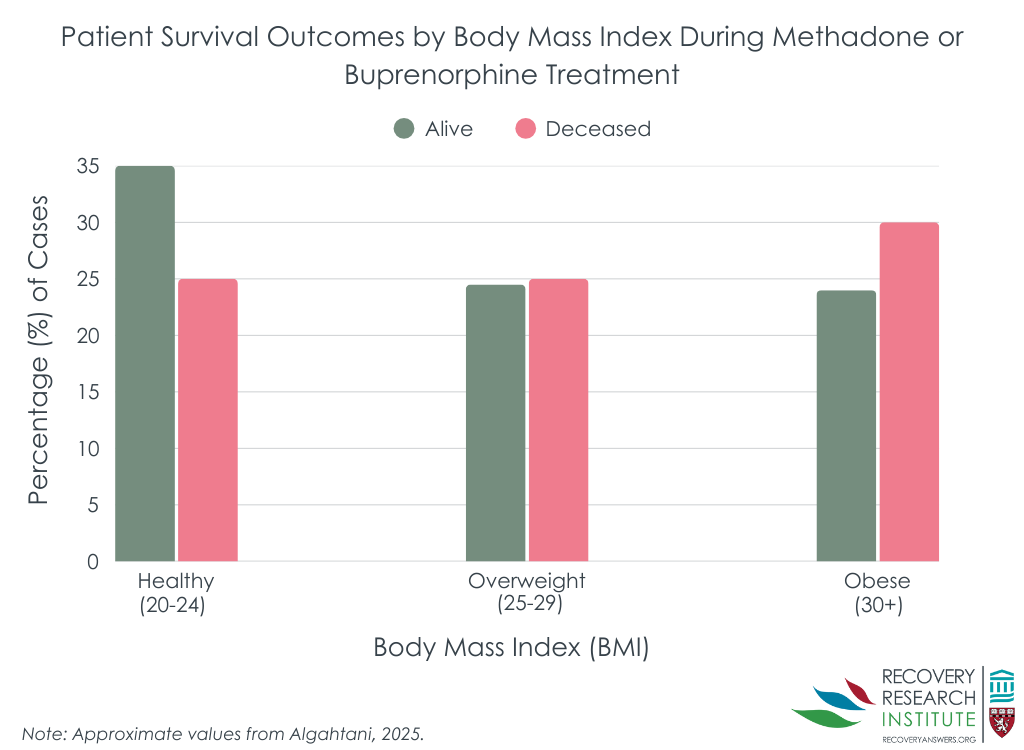
On average, a BMI of 26 was consistent with with an “overweight” patient population based on the threshold of 25. Half were overweight and one-quarter had a BMI consistent with obesity. As might be expected, deceased patients had a higher average BMI than living patients (M = 26.63 vs. 25.61), though this difference was small (standardized effect size of only 0.14).
Being obese or underweight was associated with increased risk of mortality
Compared to BMI of 25, obesity (i.e. BMI of ≥30) was associated with increased risk of mortality (Figure below); a BMI of 30, 35, and 40 increased risk of death by 7.7%, 37.2%, and 107.3%, respectively. Individuals who were underweight (i.e. BMI of ≤15) also had a 44% increased risk of death.
Individuals who were older, smoked tobacco, and lived in more deprived areas had increased odds of mortality relative to those who were younger, nonsmokers, and those living in less deprived regions. Odds of mortality were greatest among those who smoked, with smoking increasing odds of death by about 170%. Individuals taking methadone were also more likely to have died than individuals taking buprenorphine (~89% increased odds). Among those who received methadone treatment, dose of methadone was not associated with mortality risk.
Drug toxicity was the leading cause of death among healthy and overweight patients
Acute drug toxicity accounted for 46% of deaths in both those with a healthy BMI as well as overweight individuals. Drug toxicity accounted for about 25% of deaths among underweight patients, with cancer, infection, and cardiorespiratory complications being somewhat more prominent (~18-20%) causes of death among those who were underweight.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, nearly half of patients receiving opioid agonist treatment with buprenorphine or methadone were overweight, and one-quarter were considered obese. Obesity was associated with greater risk of death regardless of age, gender, medication type and dose, regional socioeconomic status (i.e., “deprivation” index), and smoking status, with risk increasing as BMI increases among obese individuals. Importantly, individuals who were underweight were also more likely to die, suggesting a potential need for healthy weight goals, as opposed to purely weight loss, and ongoing monitoring of patients during medication treatment for opioid use disorder.
Weight has been long known to impact health; increased odds of death with higher BMI are seen in the general population but few studies have examined this relationship among individuals who are seeking treatment for opioid use disorder, as they are often stereotyped as being underweight as a result of illicit opioid use and related malnutrition. However, with treatment, weight fluctuations and their implications have been less well understood to date. As such, treatment guidelines may fail to address weight management in the long term.
This study suggests that weight management may be important in reducing mortality risk among patients receiving medication treatment. Additional research is needed to determine the best ways to integrate weight monitoring and management (diet, exercise, etc.) into treatment plans that promote patient education and compliance with suggested programs. Given that individuals receiving medication treatment are required to regularly visit with their doctor, nutrition could be easily incorporated into healthcare discussions and monitoring with little cost.
As expected, certain patient characteristics were also associated with increased mortality, including older age, living in a region considered more deprived, and smoking tobacco. The link between these factors and mortality risk is well established in the general population. In this study tobacco smoking had the greatest impact on mortality, increasing odds of death by about 170% in methadone and buprenorphine patients. This emphasizes the importance of addressing tobacco and nicotine use during addiction treatment, to help patients improve their overall health and reduce risk factors for morbidity and mortality.
Individuals prescribed methadone were also more likely to have died than individuals who received buprenorphine. Though the most common cause of death was acute drug toxicity (e.g., overdose death), methadone dose was not associated with mortality risk, suggesting that factors other than the medication type may contribute to differences in mortality risk among these patient samples. For example, disorder severity may differ among patients receiving methadone versus buprenorphine. Indeed, methadone is typically reserved for individuals with more severe opioid use disorder cases, and individuals with greater severity may be more likely to also present with ongoing illicit opioid use, as well as other comorbid conditions and medications that increase risk of death. Thus, differences in disorder severity, comorbidities, and ongoing drug use may have contributed to observed differences in mortality risk by medication type. Additional research, including randomized controlled trials that can better account for severity and comorbidities, will help clarify the influence of medication type on BMI and mortality risk.
This study was conducted in two communities in England that are known to have poorer health outcomes and findings may not apply to communities with greater resources and access to healthy living.
Deceased and living patients were examined at different time periods to gather a larger sample of deceased patients and time-related factors may play a role in mortality risks and patterns – though it is unclear whether this would over or underestimate the relationship between BMI and mortality. Nineteen percent of patients who were deceased had missing data on smoking.
These data were also examined retrospectively, limited information was available for covariates, and disorder severity and ongoing illicit drug use was not assessed as a factor that may have influenced mortality risk, warranting additional research.
BOTTOM LINE
Nearly half of patients receiving opioid agonist treatment with buprenorphine or methadone were overweight, with one-quarter being obese. Being obese and being underweight were associated with increased risk of death. This study highlights a potentially important role for weight monitoring during medication treatment for opioid use disorder to reduce patient risk of mortality. Additional research will help clarify the relationship between medication treatment, body mass index (BMI), and mortality risk, which can ultimately help inform comprehensive treatment approaches that promote addiction recovery alongside the recovery of other physical and mental health conditions that arise over the course of treatment.
For individuals and families seeking recovery: Methadone and buprenorphine are lifesaving medications for many that can help initiate and sustain recovery. All medications come with side effects and, when known, these side effects can be mitigated or avoided. Individuals receiving methadone or buprenorphine treatment may be at risk of gaining weight to the point where they are considered overweight or obese, which can increase risk of death. Thus, it is important to manage all aspects of health while undergoing treatment, including nutritional health. Individuals and families are encouraged to speak to their healthcare providers about their diet and steps they can take to improve their eating habits to support a healthy weight and reduce the risks associated with being overweight and underweight.
For treatment professionals and treatment systems: This study suggests that weight management is essential to reducing mortality risk among patients receiving opioid use disorder medication treatment, as being underweight and overweight increases risk of death. Regular doctor visits, as necessitated for medication treatment, may be an ideal time to address nutrition and weight management to better support patient health with limited additional cost to the provider, as BMI assessment only requires a scale for measuring weight and height.
For scientists: Randomized controlled trials are needed to examine the relationship between weight/BMI and mortality risk among methadone and buprenorphine patients. Studies examining differences according to medication type, controlling for potential confounders like opioid use disorder severity, ongoing illicit drug use, other prescribed medications and comorbid disorders are warranted to determine if this effect is methadone specific and to determine the degree to which nutritional intake, medication pharmacokinetics and metabolism contribute to the relationship between BMI and mortality risk during medication treatment.
For policy makers: Understanding the relationship between BMI and mortality among individuals with opioid use disorder is important because obesity and opioid use disorder are established, independent risk factors for death, and unhealthy weight gain is relatively common during opioid use disorder medication treatment. The relationship between weight gain and mortality risk during medication treatment requires additional research to determine differences in risk according to medication type, disorder severity, and other comorbid conditions. Studies like this can ultimately help reduce mortality to better support the overall goal of opioid use disorder medication treatment programs (improved health reduced risk for drug use-related death).
Chronic repeated use of illicit opioids like heroin and fentanyl can reduce appetite. Resulting malnutrition can compromise bone health and immune system function. Addressing nutritional health when patients present for opioid use disorder treatment is often an essential component of holistic recovery. In addition to providing medication treatments like methadone and buprenorphine, opioid use disorder treatment programs may offer patients information about healthy lifestyle changes such as nutritional intake to promote improvements in health and well-being.
At the same time, weight gain and increased body mass index (BMI) – a common way of measuring health-limiting levels of body fat – are potential side effects of agonist medication treatments for opioid use disorder. Individuals receiving methadone treatment, for example, are more likely to be overweight and obese relative to the general population, with about 3/4 of patients being overweight.
There are likely many reasons underlying this weight gain. For example, underweight patients may be encouraged by healthcare providers and treatment staff to gain weight during the initial stages of treatment, which could lead to excessive weight gain over time. In addition, dysregulated reward systems may contribute to comfort eating to provide feelings of reward in the absence of a person’s drug of choice. Chronic exposure to illicit opioids and opioid agonist treatments like methadone can also lead to heightened preferences for foods with high sugar content. Indeed, individuals receiving methadone are shown to increase consumption of sugary foods and beverages throughout the course of treatment. Methadone itself can also cause increased appetite and reduced metabolism, further contributing to overeating and weight gain.
Obesity comes with risk of morbidity and mortality, independent of opioid use disorder. Thus, it is essential to better understand this increased risk of weight gain during opioid use disorder medication treatment and its effect on patient outcomes. Though weight gain is common during medication treatment, the relationship between weight gain and mortality risk during medication treatment is not entirely clear and few studies have included patients receiving both methadone and buprenorphine treatment. This study aimed to address this gap by assessing the relationship between weight and risk of death among individuals receiving methadone or buprenorphine treatment for opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a retrospective case–control study of the relationship between body weight and mortality risk for adults receiving opioid agonist medication treatment. The authors examined government data collected at addiction treatment facilities in two regions of England (i.e. Derbyshire & Teesside). The analysis included living patients (n = 1,574) who received opioid agonist treatment (buprenorphine or methadone) between 2022 and 2023, as well as deceased patients (n = 233) who were receiving opioid agonist treatment at the time of their death between 2015 and 2023.
Variables included BMI (for determining whether a person was overweight, underweight, or healthy weight), age, opioid agonist treatment type and dose, smoking status, and residence in a deprived region of England (determined with residential zip codes of patients and assessing factors like income, employment, education, and crime in that region). Causes of death were also assessed for deceased patients. Body weight was evaluated as BMI, determined with measures of height and weight obtained at patients’ most recent treatment service appointments (for deceased patients, this was collected at their last attended appointment prior to death). BMIs of ≤15 are considered underweight and indexes of 16 – 24 are considered healthy weight. BMIs of 25 are considered overweight and those of 30 and greater are considered “obese”. Causes of death were determined from coroner reports, which only included unnatural and unexpected deaths (n = 202/233 deaths included in analyses of mortality cause). Less than 2% of patients were excluded from analyses because they opted out of data sharing for research purposes. Nineteen percent of deceased patients had missing data for smoking status.
The study’s primary focus was on 1) the relationship between weight and mortality among patients receiving buprenorphine or methadone (n=1807) controlling statistically for age, gender, medication type and dose, regional socioeconomic status (i.e., “deprivation” index), and smoking status; and (2) the weight and mortality specifically among patients receiving methadone and for whom methadone dose was available in the dataset (n=1562) adjusting also for these same factors (apart from medication type/dose). They also examined the role of other variables of interest like age and gender (see variables of interest above).
WHAT DID THIS STUDY FIND?
Deceased patients had higher BMI
On average, a BMI of 26 was consistent with with an “overweight” patient population based on the threshold of 25. Half were overweight and one-quarter had a BMI consistent with obesity. As might be expected, deceased patients had a higher average BMI than living patients (M = 26.63 vs. 25.61), though this difference was small (standardized effect size of only 0.14).
Being obese or underweight was associated with increased risk of mortality
Compared to BMI of 25, obesity (i.e. BMI of ≥30) was associated with increased risk of mortality (Figure below); a BMI of 30, 35, and 40 increased risk of death by 7.7%, 37.2%, and 107.3%, respectively. Individuals who were underweight (i.e. BMI of ≤15) also had a 44% increased risk of death.
Individuals who were older, smoked tobacco, and lived in more deprived areas had increased odds of mortality relative to those who were younger, nonsmokers, and those living in less deprived regions. Odds of mortality were greatest among those who smoked, with smoking increasing odds of death by about 170%. Individuals taking methadone were also more likely to have died than individuals taking buprenorphine (~89% increased odds). Among those who received methadone treatment, dose of methadone was not associated with mortality risk.
Drug toxicity was the leading cause of death among healthy and overweight patients
Acute drug toxicity accounted for 46% of deaths in both those with a healthy BMI as well as overweight individuals. Drug toxicity accounted for about 25% of deaths among underweight patients, with cancer, infection, and cardiorespiratory complications being somewhat more prominent (~18-20%) causes of death among those who were underweight.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, nearly half of patients receiving opioid agonist treatment with buprenorphine or methadone were overweight, and one-quarter were considered obese. Obesity was associated with greater risk of death regardless of age, gender, medication type and dose, regional socioeconomic status (i.e., “deprivation” index), and smoking status, with risk increasing as BMI increases among obese individuals. Importantly, individuals who were underweight were also more likely to die, suggesting a potential need for healthy weight goals, as opposed to purely weight loss, and ongoing monitoring of patients during medication treatment for opioid use disorder.
Weight has been long known to impact health; increased odds of death with higher BMI are seen in the general population but few studies have examined this relationship among individuals who are seeking treatment for opioid use disorder, as they are often stereotyped as being underweight as a result of illicit opioid use and related malnutrition. However, with treatment, weight fluctuations and their implications have been less well understood to date. As such, treatment guidelines may fail to address weight management in the long term.
This study suggests that weight management may be important in reducing mortality risk among patients receiving medication treatment. Additional research is needed to determine the best ways to integrate weight monitoring and management (diet, exercise, etc.) into treatment plans that promote patient education and compliance with suggested programs. Given that individuals receiving medication treatment are required to regularly visit with their doctor, nutrition could be easily incorporated into healthcare discussions and monitoring with little cost.
As expected, certain patient characteristics were also associated with increased mortality, including older age, living in a region considered more deprived, and smoking tobacco. The link between these factors and mortality risk is well established in the general population. In this study tobacco smoking had the greatest impact on mortality, increasing odds of death by about 170% in methadone and buprenorphine patients. This emphasizes the importance of addressing tobacco and nicotine use during addiction treatment, to help patients improve their overall health and reduce risk factors for morbidity and mortality.
Individuals prescribed methadone were also more likely to have died than individuals who received buprenorphine. Though the most common cause of death was acute drug toxicity (e.g., overdose death), methadone dose was not associated with mortality risk, suggesting that factors other than the medication type may contribute to differences in mortality risk among these patient samples. For example, disorder severity may differ among patients receiving methadone versus buprenorphine. Indeed, methadone is typically reserved for individuals with more severe opioid use disorder cases, and individuals with greater severity may be more likely to also present with ongoing illicit opioid use, as well as other comorbid conditions and medications that increase risk of death. Thus, differences in disorder severity, comorbidities, and ongoing drug use may have contributed to observed differences in mortality risk by medication type. Additional research, including randomized controlled trials that can better account for severity and comorbidities, will help clarify the influence of medication type on BMI and mortality risk.
This study was conducted in two communities in England that are known to have poorer health outcomes and findings may not apply to communities with greater resources and access to healthy living.
Deceased and living patients were examined at different time periods to gather a larger sample of deceased patients and time-related factors may play a role in mortality risks and patterns – though it is unclear whether this would over or underestimate the relationship between BMI and mortality. Nineteen percent of patients who were deceased had missing data on smoking.
These data were also examined retrospectively, limited information was available for covariates, and disorder severity and ongoing illicit drug use was not assessed as a factor that may have influenced mortality risk, warranting additional research.
BOTTOM LINE
Nearly half of patients receiving opioid agonist treatment with buprenorphine or methadone were overweight, with one-quarter being obese. Being obese and being underweight were associated with increased risk of death. This study highlights a potentially important role for weight monitoring during medication treatment for opioid use disorder to reduce patient risk of mortality. Additional research will help clarify the relationship between medication treatment, body mass index (BMI), and mortality risk, which can ultimately help inform comprehensive treatment approaches that promote addiction recovery alongside the recovery of other physical and mental health conditions that arise over the course of treatment.
For individuals and families seeking recovery: Methadone and buprenorphine are lifesaving medications for many that can help initiate and sustain recovery. All medications come with side effects and, when known, these side effects can be mitigated or avoided. Individuals receiving methadone or buprenorphine treatment may be at risk of gaining weight to the point where they are considered overweight or obese, which can increase risk of death. Thus, it is important to manage all aspects of health while undergoing treatment, including nutritional health. Individuals and families are encouraged to speak to their healthcare providers about their diet and steps they can take to improve their eating habits to support a healthy weight and reduce the risks associated with being overweight and underweight.
For treatment professionals and treatment systems: This study suggests that weight management is essential to reducing mortality risk among patients receiving opioid use disorder medication treatment, as being underweight and overweight increases risk of death. Regular doctor visits, as necessitated for medication treatment, may be an ideal time to address nutrition and weight management to better support patient health with limited additional cost to the provider, as BMI assessment only requires a scale for measuring weight and height.
For scientists: Randomized controlled trials are needed to examine the relationship between weight/BMI and mortality risk among methadone and buprenorphine patients. Studies examining differences according to medication type, controlling for potential confounders like opioid use disorder severity, ongoing illicit drug use, other prescribed medications and comorbid disorders are warranted to determine if this effect is methadone specific and to determine the degree to which nutritional intake, medication pharmacokinetics and metabolism contribute to the relationship between BMI and mortality risk during medication treatment.
For policy makers: Understanding the relationship between BMI and mortality among individuals with opioid use disorder is important because obesity and opioid use disorder are established, independent risk factors for death, and unhealthy weight gain is relatively common during opioid use disorder medication treatment. The relationship between weight gain and mortality risk during medication treatment requires additional research to determine differences in risk according to medication type, disorder severity, and other comorbid conditions. Studies like this can ultimately help reduce mortality to better support the overall goal of opioid use disorder medication treatment programs (improved health reduced risk for drug use-related death).
Chronic repeated use of illicit opioids like heroin and fentanyl can reduce appetite. Resulting malnutrition can compromise bone health and immune system function. Addressing nutritional health when patients present for opioid use disorder treatment is often an essential component of holistic recovery. In addition to providing medication treatments like methadone and buprenorphine, opioid use disorder treatment programs may offer patients information about healthy lifestyle changes such as nutritional intake to promote improvements in health and well-being.
At the same time, weight gain and increased body mass index (BMI) – a common way of measuring health-limiting levels of body fat – are potential side effects of agonist medication treatments for opioid use disorder. Individuals receiving methadone treatment, for example, are more likely to be overweight and obese relative to the general population, with about 3/4 of patients being overweight.
There are likely many reasons underlying this weight gain. For example, underweight patients may be encouraged by healthcare providers and treatment staff to gain weight during the initial stages of treatment, which could lead to excessive weight gain over time. In addition, dysregulated reward systems may contribute to comfort eating to provide feelings of reward in the absence of a person’s drug of choice. Chronic exposure to illicit opioids and opioid agonist treatments like methadone can also lead to heightened preferences for foods with high sugar content. Indeed, individuals receiving methadone are shown to increase consumption of sugary foods and beverages throughout the course of treatment. Methadone itself can also cause increased appetite and reduced metabolism, further contributing to overeating and weight gain.
Obesity comes with risk of morbidity and mortality, independent of opioid use disorder. Thus, it is essential to better understand this increased risk of weight gain during opioid use disorder medication treatment and its effect on patient outcomes. Though weight gain is common during medication treatment, the relationship between weight gain and mortality risk during medication treatment is not entirely clear and few studies have included patients receiving both methadone and buprenorphine treatment. This study aimed to address this gap by assessing the relationship between weight and risk of death among individuals receiving methadone or buprenorphine treatment for opioid use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a retrospective case–control study of the relationship between body weight and mortality risk for adults receiving opioid agonist medication treatment. The authors examined government data collected at addiction treatment facilities in two regions of England (i.e. Derbyshire & Teesside). The analysis included living patients (n = 1,574) who received opioid agonist treatment (buprenorphine or methadone) between 2022 and 2023, as well as deceased patients (n = 233) who were receiving opioid agonist treatment at the time of their death between 2015 and 2023.
Variables included BMI (for determining whether a person was overweight, underweight, or healthy weight), age, opioid agonist treatment type and dose, smoking status, and residence in a deprived region of England (determined with residential zip codes of patients and assessing factors like income, employment, education, and crime in that region). Causes of death were also assessed for deceased patients. Body weight was evaluated as BMI, determined with measures of height and weight obtained at patients’ most recent treatment service appointments (for deceased patients, this was collected at their last attended appointment prior to death). BMIs of ≤15 are considered underweight and indexes of 16 – 24 are considered healthy weight. BMIs of 25 are considered overweight and those of 30 and greater are considered “obese”. Causes of death were determined from coroner reports, which only included unnatural and unexpected deaths (n = 202/233 deaths included in analyses of mortality cause). Less than 2% of patients were excluded from analyses because they opted out of data sharing for research purposes. Nineteen percent of deceased patients had missing data for smoking status.
The study’s primary focus was on 1) the relationship between weight and mortality among patients receiving buprenorphine or methadone (n=1807) controlling statistically for age, gender, medication type and dose, regional socioeconomic status (i.e., “deprivation” index), and smoking status; and (2) the weight and mortality specifically among patients receiving methadone and for whom methadone dose was available in the dataset (n=1562) adjusting also for these same factors (apart from medication type/dose). They also examined the role of other variables of interest like age and gender (see variables of interest above).
WHAT DID THIS STUDY FIND?
Deceased patients had higher BMI
On average, a BMI of 26 was consistent with with an “overweight” patient population based on the threshold of 25. Half were overweight and one-quarter had a BMI consistent with obesity. As might be expected, deceased patients had a higher average BMI than living patients (M = 26.63 vs. 25.61), though this difference was small (standardized effect size of only 0.14).
Being obese or underweight was associated with increased risk of mortality
Compared to BMI of 25, obesity (i.e. BMI of ≥30) was associated with increased risk of mortality (Figure below); a BMI of 30, 35, and 40 increased risk of death by 7.7%, 37.2%, and 107.3%, respectively. Individuals who were underweight (i.e. BMI of ≤15) also had a 44% increased risk of death.
Individuals who were older, smoked tobacco, and lived in more deprived areas had increased odds of mortality relative to those who were younger, nonsmokers, and those living in less deprived regions. Odds of mortality were greatest among those who smoked, with smoking increasing odds of death by about 170%. Individuals taking methadone were also more likely to have died than individuals taking buprenorphine (~89% increased odds). Among those who received methadone treatment, dose of methadone was not associated with mortality risk.
Drug toxicity was the leading cause of death among healthy and overweight patients
Acute drug toxicity accounted for 46% of deaths in both those with a healthy BMI as well as overweight individuals. Drug toxicity accounted for about 25% of deaths among underweight patients, with cancer, infection, and cardiorespiratory complications being somewhat more prominent (~18-20%) causes of death among those who were underweight.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, nearly half of patients receiving opioid agonist treatment with buprenorphine or methadone were overweight, and one-quarter were considered obese. Obesity was associated with greater risk of death regardless of age, gender, medication type and dose, regional socioeconomic status (i.e., “deprivation” index), and smoking status, with risk increasing as BMI increases among obese individuals. Importantly, individuals who were underweight were also more likely to die, suggesting a potential need for healthy weight goals, as opposed to purely weight loss, and ongoing monitoring of patients during medication treatment for opioid use disorder.
Weight has been long known to impact health; increased odds of death with higher BMI are seen in the general population but few studies have examined this relationship among individuals who are seeking treatment for opioid use disorder, as they are often stereotyped as being underweight as a result of illicit opioid use and related malnutrition. However, with treatment, weight fluctuations and their implications have been less well understood to date. As such, treatment guidelines may fail to address weight management in the long term.
This study suggests that weight management may be important in reducing mortality risk among patients receiving medication treatment. Additional research is needed to determine the best ways to integrate weight monitoring and management (diet, exercise, etc.) into treatment plans that promote patient education and compliance with suggested programs. Given that individuals receiving medication treatment are required to regularly visit with their doctor, nutrition could be easily incorporated into healthcare discussions and monitoring with little cost.
As expected, certain patient characteristics were also associated with increased mortality, including older age, living in a region considered more deprived, and smoking tobacco. The link between these factors and mortality risk is well established in the general population. In this study tobacco smoking had the greatest impact on mortality, increasing odds of death by about 170% in methadone and buprenorphine patients. This emphasizes the importance of addressing tobacco and nicotine use during addiction treatment, to help patients improve their overall health and reduce risk factors for morbidity and mortality.
Individuals prescribed methadone were also more likely to have died than individuals who received buprenorphine. Though the most common cause of death was acute drug toxicity (e.g., overdose death), methadone dose was not associated with mortality risk, suggesting that factors other than the medication type may contribute to differences in mortality risk among these patient samples. For example, disorder severity may differ among patients receiving methadone versus buprenorphine. Indeed, methadone is typically reserved for individuals with more severe opioid use disorder cases, and individuals with greater severity may be more likely to also present with ongoing illicit opioid use, as well as other comorbid conditions and medications that increase risk of death. Thus, differences in disorder severity, comorbidities, and ongoing drug use may have contributed to observed differences in mortality risk by medication type. Additional research, including randomized controlled trials that can better account for severity and comorbidities, will help clarify the influence of medication type on BMI and mortality risk.
This study was conducted in two communities in England that are known to have poorer health outcomes and findings may not apply to communities with greater resources and access to healthy living.
Deceased and living patients were examined at different time periods to gather a larger sample of deceased patients and time-related factors may play a role in mortality risks and patterns – though it is unclear whether this would over or underestimate the relationship between BMI and mortality. Nineteen percent of patients who were deceased had missing data on smoking.
These data were also examined retrospectively, limited information was available for covariates, and disorder severity and ongoing illicit drug use was not assessed as a factor that may have influenced mortality risk, warranting additional research.
BOTTOM LINE
Nearly half of patients receiving opioid agonist treatment with buprenorphine or methadone were overweight, with one-quarter being obese. Being obese and being underweight were associated with increased risk of death. This study highlights a potentially important role for weight monitoring during medication treatment for opioid use disorder to reduce patient risk of mortality. Additional research will help clarify the relationship between medication treatment, body mass index (BMI), and mortality risk, which can ultimately help inform comprehensive treatment approaches that promote addiction recovery alongside the recovery of other physical and mental health conditions that arise over the course of treatment.
For individuals and families seeking recovery: Methadone and buprenorphine are lifesaving medications for many that can help initiate and sustain recovery. All medications come with side effects and, when known, these side effects can be mitigated or avoided. Individuals receiving methadone or buprenorphine treatment may be at risk of gaining weight to the point where they are considered overweight or obese, which can increase risk of death. Thus, it is important to manage all aspects of health while undergoing treatment, including nutritional health. Individuals and families are encouraged to speak to their healthcare providers about their diet and steps they can take to improve their eating habits to support a healthy weight and reduce the risks associated with being overweight and underweight.
For treatment professionals and treatment systems: This study suggests that weight management is essential to reducing mortality risk among patients receiving opioid use disorder medication treatment, as being underweight and overweight increases risk of death. Regular doctor visits, as necessitated for medication treatment, may be an ideal time to address nutrition and weight management to better support patient health with limited additional cost to the provider, as BMI assessment only requires a scale for measuring weight and height.
For scientists: Randomized controlled trials are needed to examine the relationship between weight/BMI and mortality risk among methadone and buprenorphine patients. Studies examining differences according to medication type, controlling for potential confounders like opioid use disorder severity, ongoing illicit drug use, other prescribed medications and comorbid disorders are warranted to determine if this effect is methadone specific and to determine the degree to which nutritional intake, medication pharmacokinetics and metabolism contribute to the relationship between BMI and mortality risk during medication treatment.
For policy makers: Understanding the relationship between BMI and mortality among individuals with opioid use disorder is important because obesity and opioid use disorder are established, independent risk factors for death, and unhealthy weight gain is relatively common during opioid use disorder medication treatment. The relationship between weight gain and mortality risk during medication treatment requires additional research to determine differences in risk according to medication type, disorder severity, and other comorbid conditions. Studies like this can ultimately help reduce mortality to better support the overall goal of opioid use disorder medication treatment programs (improved health reduced risk for drug use-related death).