
Retrain the Brain: Effects on Neural Alcohol Cue Reactivity
Addiction is a disorder, with both environmental and neurological attributes, changing complex neurobiological pathways in the brain.
When people suffering from alcohol addiction see alcohol-related stimuli and images, physiological reactions occur in the brain, a phenomenon known as cue reactivity. This is because of the process of associative learning or “classical conditioning”, whereby certain cues (e.g., seeing the drug or a picture of the drug itself or seeing people, places, or other things associated with the drug) become strongly associated with the drug taking experience.
Of particular importance is reactivity in areas of the brain that are associated with craving and reward processing:
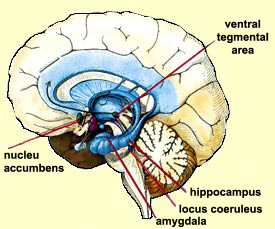
Current research suggests that after a few weeks of therapy, activation in these areas due to alcohol-related cues may decrease, signifying the potential for interventions that reduce neural cue reactivity.
One such intervention is cognitive bias modification which addresses a bias in the tendency to approach alcohol, and has been shown in a previous study to reduce alcohol craving and relapse. To better understand the mechanism underlying cognitive bias modification training, Wiers and colleagues used a double-blind randomized experiment to evaluate the effects of this training on neural reactivity induced by alcohol-related cues.
- READ MORE ON STUDY METHODS
-
32 male participants in inpatient treatment for alcohol use disorder in Germany were randomized to cognitive bias modification training (n = 15) or the control condition, sham training (n = 17). Participants performed an approach-avoidance task in response to an irrelevant stimulus, cue image format (i.e., portrait or landscape).
Depending on the format of the cue, participants pushed or pulled images of alcohol and soft drinks on a computer using a joystick (e.g., pushed the joystick if the image was landscape format and pulled if it was portrait).
Pulling the joystick caused the image size to increase while pushing the joystick caused the size to decrease. This zooming feature created a visual impression that the picture was pulled closer (approach) or pushed away (avoidance). Without the zooming effect, pushing the joystick in response to an alcohol image could be interpreted as avoidance in respect to the patient’s body but also as approach with respect to the alcohol (see here for more detail). The task, which used an equal number of alcohol and soft drink images, was performed before and after the training period to measure approach bias for alcohol cues (i.e. the propensity of a participant to pull alcohol cues faster than they push them).
During the three week training period, participants completed six sessions of the approach-avoidance task. The ratio of alcohol to soft drink images was changed for the bias modification training group but remained at 50/50 for the control group. The goal of cognitive bias modification was to decrease approach bias and the impulsivity towards alcohol-related cues by training participants to learn to push away and avoid these cues. The same images from the approach-avoidance task were also used in a functional MRI (fMRI) cue reactivity task, the purpose of which was to measure neural cue reactivity before and after the training period.
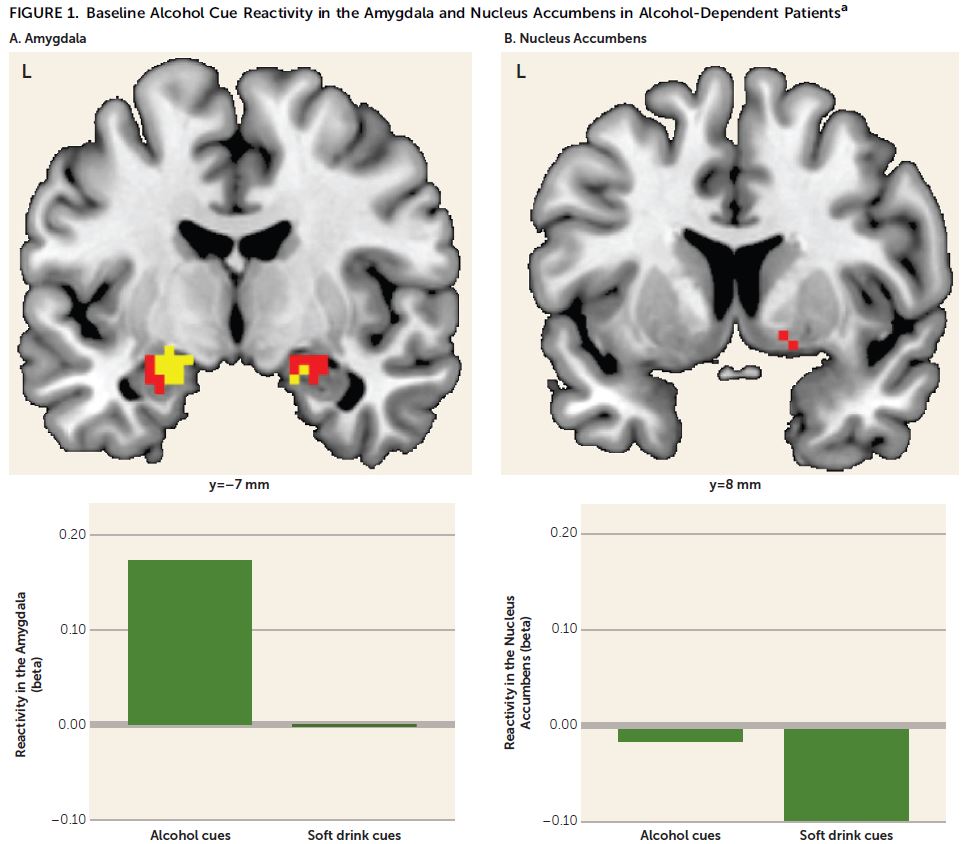
Participants also rated pictures for arousal (on a 5-point Likert scale) and alcohol craving (using the Desire for Alcohol Questionnaire). The authors hypothesized that before the training period, all participants would show activation in the amygdala and nucleus accumbens in response to alcohol cues, and the cognitive bias modification group would show a decrease in cue reactivity after training. On average, participants were 44 years old, had 10 years of education, and had used alcohol heavily for 15 years. There were no significant differences in baseline demographic or clinical characteristics between groups.
Alcohol approach bias scores did not differ before or after training for the two groups. A decrease in mean reaction time just missed significance for the bias modification training group but not for the control group. In both groups, craving scores were higher before training, with a significant decrease observed in the bias modification training group. There was a significant group-by-time interaction for arousal ratings but decrease in ratings was not significant for each group.
IN CONTEXT
Cue reactivity studies offer a different perspective on recovery research as reductions in cue reactivity is thought to be a mechanism of recovery and remission.
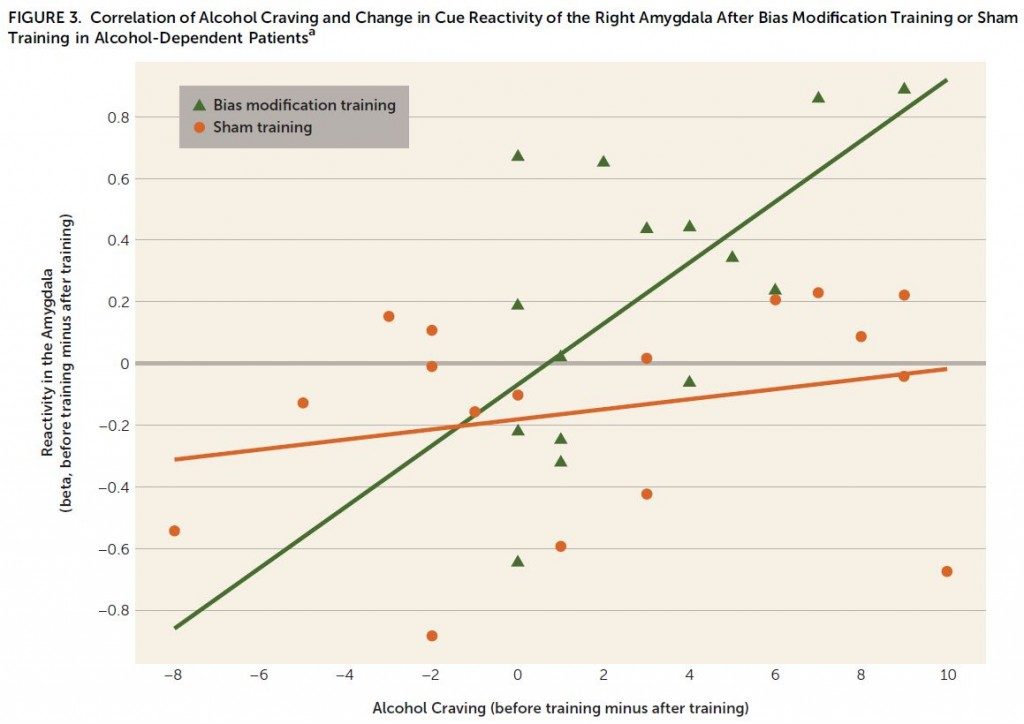
The results of this novel study provide support for the ability of cognitive bias modification training to affect alcohol cue-evoked activity in the amygdala, an area of the brain associated with alcohol craving and relapse.
The correlation between the decrease in amygdala activity and decrease in craving scores after the training period for the bias modification training group is important for two reasons:
- it provides evidence of a mechanism behind the clinical benefit of cognitive bias modification training
- it points toward reduced activity in the amygdala in response to alcohol cues as a potential biomarker for reductions in alcohol craving.
This study also shows the potential of using fMRI measurements to predict effectiveness of this training type for individual patients.
- LIMITATIONS
-
- It is unclear why the training resulted in reduced amygdala activity in response to alcohol cues (which was correlated with reduced craving) but did not result in reduced craving relative to sham training.
- While the authors attempted to assess the relationship between cue reactivity and relapse one year later, the study was not powered to detect these effects, providing an avenue for future research into amygdala reactivity as a predictor of relapse.
BOTTOM LINE
- For individuals & families seeking recovery: Cognitive bias modification training is a new area of research. More research is needed to know if this approach improves outcomes over other methods.
- For scientists: Neuroimaging studies provide another dimension to recovery research. Identifying biomarkers and predictors of substance use outcomes may eventually help inform clinical practice interventions.
- For policy makers: As technology improves, neuroimaging may become more commonplace in the clinical setting. Support for such advancements is necessary for the production of clinically valuable results.
- For treatment professionals and treatment systems: While these results are preliminary and not yet ready for dissemination and implementation, such techniques may be employed in the future. Currently there is some support for the benefit of cognitive bias modification training which may benefit patients with alcohol use disorder.
CITATIONS
Wiers, C. E., Stelzel, C., Gladwin, T. E., Park, S. Q., Pawelczack, S., Gawron, C. K., … & Bermpohl, F. (2014). Effects of Cognitive Bias Modification Training on Neural Alcohol Cue Reactivity in Alcohol Dependence. American Journal of Psychiatry.
