Medication typically prescribed for ADHD may offer some benefit for methamphetamine use disorder
Methamphetamine use disorder is rising in the United States while its treatment is limited by lack of FDA-approved medications. This study tested whether the ADHD medication lisdexamfetamine – best known by the brand name Vyvanse – might offer help to individuals with more severe methamphetamine use profiles.
Methamphetamine is classified as a Schedule II drug indicating some acceptable medical utility. However, methamphetamine also has significant addictive potential and can lead to substantial toxicity in the brain and body, facilitating the breakdown of skeletal muscle, and inducing seizures and bleeding in the brain at high doses and with chronic use. The past decade has seen a rise in prevalence of methamphetamine use and overdoses involving methamphetamine, particularly in conjunction with opioids.
Psychosocial treatments such as contingency management, a collection of approaches that systematically use incentives to positively reinforce stimulant abstinence (e.g., by providing monetary vouchers to patients for testing negative for stimulant use via urinalysis), are empirically supported for those with methamphetamine use disorder. Additionally, cognitive behavioral therapy (CBT) strategies appear to improve treatment retention.
However, studies have shown that psychosocial treatments are less effective among people with higher levels of methamphetamine use – those using more than half the days in a month, for example. There is a pressing need to identify additional treatment alternatives to enhance treatment efficacy for people who use methamphetamine. Despite decades of medication trials and the public health impact of methamphetamine use, there are no medications approved by the Food and Drug Administration for treating methamphetamine use disorder.
Lisdexamfetamine, an agonist-like stimulant medication also known and marketed by the brand name Vyvanse, is currently FDA-approved to treat attention-deficit hyperactivity disorder (ADHD) and binge-eating disorder. Agonist medications have become increasingly investigated as medications for substance use disorders, in part due to their success in treatment of opioid use disorder over the past few decades. Like other agonist medications, lisdexamfetamine operates similarly to methamphetamine pharmacologically but has a slower onset, longer duration of action, and must be metabolized in the stomach to produce its effects (i.e., it is a ”prodrug” of the medication’s active ingredient) which is thought to reduce the medication’s potential for addiction and other non-medical use. This randomized controlled trial tested the initial efficacy and safety of lisdexamfetamine in reducing methamphetamine use for people with more severe methamphetamine use profiles.
HOW WAS THIS STUDY CONDUCTED?
This study used a randomized double-blind trial to test oral lisdexamfetamine (250 mg daily) in 75 individuals or an identical matched placebo for 80 individuals, all of whom were using methamphetamine at least 14 out of the last 28 days. Participants, who were recruited from 6 Australian treatment clinics specializing in the treatment of stimulant use disorder, underwent a 1-week induction of medication followed by 12 weeks of the medication trial and a 2-week taper. They completed follow-ups at weeks 5, 9, 13, and 19 the latter of which occurred 4 weeks after discontinuing the medication or placebo. In addition to medications, all participants were offered 4 sessions of CBT for methamphetamine use by trained and supervised therapists as consistent with standard care. The primary outcome was the number of days of self-reported methamphetamine use in the past 28 days at the end of the 12-week active medication period (week 13). Secondary outcomes included number of days of self-reported methamphetamine use across the entire 12-week treatment period (possible range = 0–84 days), maximum consecutive abstinence days during treatment period, percentage 21+ consecutive abstinence days at any point during the medication period, percentage of methamphetamine-negative urine tests over 12 weeks and in the last 4 weeks (one a week, with missing tests considered positive), craving, withdrawal, methamphetamine use severity, insomnia, depression, anxiety, stress, quality of life, treatment retention, criminal behavior, and treatment satisfaction.
Participants were eligible for the study: 1) If they met criteria for methamphetamine dependence based on the ICD-10 (consistent with DSM-5 moderate or severe) as determined by an addiction medicine specialist; 2) if they used methamphetamine during more than half of the past 28 days; and 3) if they were not ruled out by any exclusion criteria including, but not limited to, currently taking opioid agonist medication, concurrent severe psychiatric or other medical disorder, other substance use disorder which might interfere with participation in the study, or use of another prescribed stimulant (such as methylphenidate). Although 164 were initially recruited for the study, the study excluded 9 individuals (4 in the placebo group, and 5 in the lisdexamfetamine group) who did not start study medication following randomization.
Participants were, on average, 39.4 years of age. And 61% identified as male. Of the full sample, 46% did not complete high school equivalent, whereas 40% had at least trade or vocational school education or higher, with 19% having obtained a university degree. Participants reported an average of 24 days of methamphetamine use in the past 28 days.
WHAT DID THIS STUDY FIND?
The medication reduced methamphetamine use, but only slightly
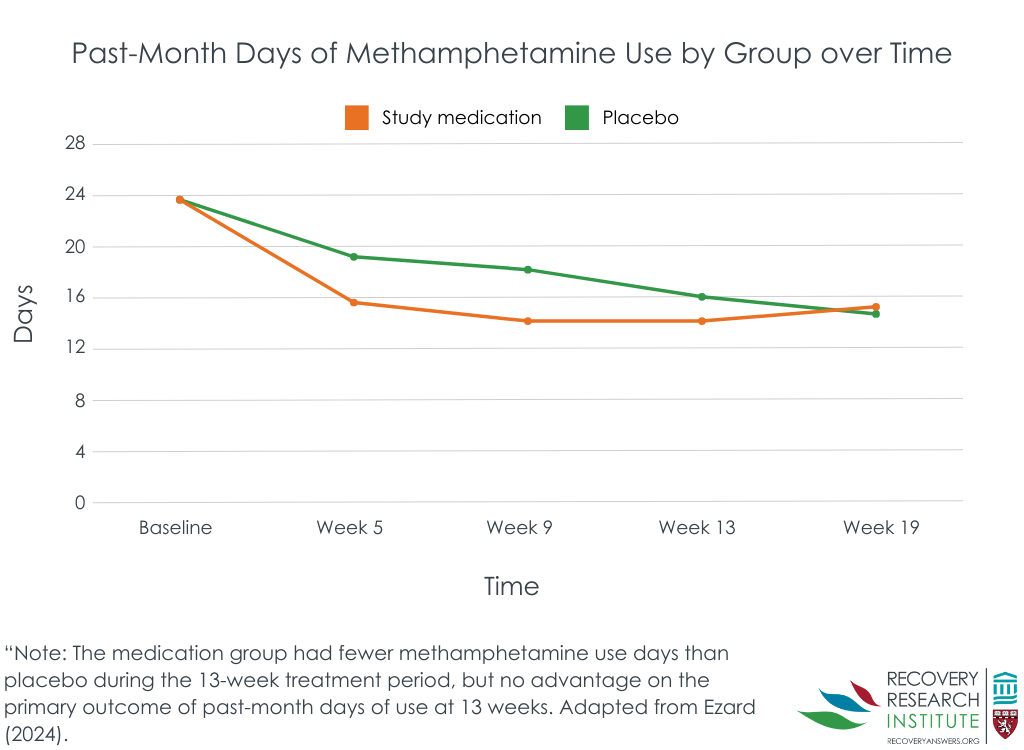
A total of 100 participants (50 placebo, 50 lisdexamfetamine) completed data collection at the Week 13 time-point, an attrition rate of 39.0%. At the 13 week follow up, those in the placebo condition reported 16 days, on average, of methamphetamine use in the past 28 days, whereas those in the lisdexamfetamine group reported 14 days of methamphetamine use (see Figure below), a non-significant difference. During the full 12-week medication period, however, the medication group had 44 days of methamphetamine use, significantly fewer than the 53 days in the placebo condition (see Figure below). There were no differences between the medication and placebo groups on longest period of abstinence over the study period, percentage achieving 21 consecutive days of abstinence, proportion of negative urine screens (over 12 or the final 4 weeks), participant retainment (at week 5, 9, or 13), craving, amphetamine withdrawal, methamphetamine use severity, or injection use.
Treatment adherence, satisfaction were largely similar, though some additional side effect risk present in medication group
The results suggested higher global satisfaction for the lisdexamfetamine group compared to the placebo. There were no differences in adherence across groups. Participants were more likely to report higher drug liking scores for lisdexamfetamine compared to placebo. Although 73% of participants in the lisdexamfetamine group and 75% of participants in the placebo group experienced adverse events, only 8 were deemed serious adverse events: 5 in the lisdexamfetamine group and 3 in the placebo group. One notable adverse event: the medication group had higher diastolic blood pressure (i.e., when the heart is at rest) at weeks 5 and 8 – though systolic (i.e., when the heart beats) is the blood pressure metric most highly correlated with cardiovascular risk. The most common adverse events were headaches and nausea.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results from this clinical trial found that, over the course of the medication period, those taking lisdexamfetamine used methamphetamine less days compared to those who took placebo, but the groups were not different at the main end-point – the end of the 12-week medication period. One important limitation is that only 60% of the sample made it to the primary outcome analysis. Though the number of participants who dropped out was similar in the 2 groups and the study examined different scenarios finding largely similar results, the study did not check to see if there were any factors that predicted dropout in one group but not the other. It could have been, for example, that those with side effects in the medication group were more likely to drop out of the study than those with side effects in the placebo group. Given that the medication and placebo had largely similar outcome profiles, this type of unbalanced dropout is less of a concern than it would have been if the medication was shown to be helpful with a possibility that dropout – not medication effects – accounted for the observed benefit.
Also, as in many studies comparing a psychoactive medication to placebo, individuals were more likely to correctly guess they were receiving the study medication (i.e., a stimulant medication) than the placebo – potentially accentuating any bias by increasing positive expectancy effects in the medication group and decreasing them in the placebo group once they realized they were not getting the active medication. The advantage of lisdexamfetamine during the 12-week trial therefore should be clarified in further research.
The study only recruited people who used methamphetamine at least half the days in the past month. Although this is an important population with specialized needs, it is unclear if lisdexamfetamine might demonstrate greater efficacy in a sample of people with less severe patterns of use.
As noted above, the attrition rate was notable – only 60% completed the study. While there was no evidence that this dropout impacted interpretation of primary study findings – it might reduce the degree to which the results generalize to individuals with methamphetamine use disorder more generally.
BOTTOM LINE
Lisdexamfetamine, the medication marketed as Vyvanse for ADHD, generally had similar outcomes compared to placebo, with some small advantages for the medication, however when examining total number of methamphetamine use days across the entire trial. Given what appear to be minor side effects of lisdexamfetamine, particularly in context of many unsuccessful efforts to develop and discover useful medications for this disorder, the single positive finding may warrant more rigorous research in a larger sample. Further research may do well also to examine particular subgroups of patients who may respond particularly well to this medication.
For individuals and families seeking recovery: If you or a family member are seeking help for methamphetamine use disorder, more research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer some benefit for methamphetamine use. Other psychosocial treatments, such as contingency management, have been shown to be helpful at increasing abstinence in dozens of studies. It is also important to mention that scientists continue to explore other medication options, with some emerging as potential therapeutics that will be tested in further clinical trials.
For treatment professionals and treatment systems: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer some benefit for patients with methamphetamine use disorder. Other approaches, like contingency management, have demonstrated efficacy while greater overall engagement with treatment and recovery has shown to improve outcomes.
For scientists: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer benefit for patients with methamphetamine use disorder. A larger sample may allow for sub-group analyses including in people with less frequent methamphetamine use and those with co-occurring substance use disorders. Whether medication may be useful in combination with other treatment modalities (such as contingency management) or recovery support services (such as recovery coaches) may also prove fruitful to investigate in future research.
For policy makers: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer benefit for patients with methamphetamine use disorder. Only one positive finding out of many outcomes suggest more rigorous research may be warranted, particularly given what appear to be minor side effects of lisdexamfetamine in context of many unsuccessful efforts to develop and discover useful medications for this disorder. Policies that increase funding to continue investigating lisdexamfetamine, or funding for trials testing lisdexamfetamine in addition to psychosocial treatments, such as contingency management, may also be useful.
Methamphetamine is classified as a Schedule II drug indicating some acceptable medical utility. However, methamphetamine also has significant addictive potential and can lead to substantial toxicity in the brain and body, facilitating the breakdown of skeletal muscle, and inducing seizures and bleeding in the brain at high doses and with chronic use. The past decade has seen a rise in prevalence of methamphetamine use and overdoses involving methamphetamine, particularly in conjunction with opioids.
Psychosocial treatments such as contingency management, a collection of approaches that systematically use incentives to positively reinforce stimulant abstinence (e.g., by providing monetary vouchers to patients for testing negative for stimulant use via urinalysis), are empirically supported for those with methamphetamine use disorder. Additionally, cognitive behavioral therapy (CBT) strategies appear to improve treatment retention.
However, studies have shown that psychosocial treatments are less effective among people with higher levels of methamphetamine use – those using more than half the days in a month, for example. There is a pressing need to identify additional treatment alternatives to enhance treatment efficacy for people who use methamphetamine. Despite decades of medication trials and the public health impact of methamphetamine use, there are no medications approved by the Food and Drug Administration for treating methamphetamine use disorder.
Lisdexamfetamine, an agonist-like stimulant medication also known and marketed by the brand name Vyvanse, is currently FDA-approved to treat attention-deficit hyperactivity disorder (ADHD) and binge-eating disorder. Agonist medications have become increasingly investigated as medications for substance use disorders, in part due to their success in treatment of opioid use disorder over the past few decades. Like other agonist medications, lisdexamfetamine operates similarly to methamphetamine pharmacologically but has a slower onset, longer duration of action, and must be metabolized in the stomach to produce its effects (i.e., it is a ”prodrug” of the medication’s active ingredient) which is thought to reduce the medication’s potential for addiction and other non-medical use. This randomized controlled trial tested the initial efficacy and safety of lisdexamfetamine in reducing methamphetamine use for people with more severe methamphetamine use profiles.
HOW WAS THIS STUDY CONDUCTED?
This study used a randomized double-blind trial to test oral lisdexamfetamine (250 mg daily) in 75 individuals or an identical matched placebo for 80 individuals, all of whom were using methamphetamine at least 14 out of the last 28 days. Participants, who were recruited from 6 Australian treatment clinics specializing in the treatment of stimulant use disorder, underwent a 1-week induction of medication followed by 12 weeks of the medication trial and a 2-week taper. They completed follow-ups at weeks 5, 9, 13, and 19 the latter of which occurred 4 weeks after discontinuing the medication or placebo. In addition to medications, all participants were offered 4 sessions of CBT for methamphetamine use by trained and supervised therapists as consistent with standard care. The primary outcome was the number of days of self-reported methamphetamine use in the past 28 days at the end of the 12-week active medication period (week 13). Secondary outcomes included number of days of self-reported methamphetamine use across the entire 12-week treatment period (possible range = 0–84 days), maximum consecutive abstinence days during treatment period, percentage 21+ consecutive abstinence days at any point during the medication period, percentage of methamphetamine-negative urine tests over 12 weeks and in the last 4 weeks (one a week, with missing tests considered positive), craving, withdrawal, methamphetamine use severity, insomnia, depression, anxiety, stress, quality of life, treatment retention, criminal behavior, and treatment satisfaction.
Participants were eligible for the study: 1) If they met criteria for methamphetamine dependence based on the ICD-10 (consistent with DSM-5 moderate or severe) as determined by an addiction medicine specialist; 2) if they used methamphetamine during more than half of the past 28 days; and 3) if they were not ruled out by any exclusion criteria including, but not limited to, currently taking opioid agonist medication, concurrent severe psychiatric or other medical disorder, other substance use disorder which might interfere with participation in the study, or use of another prescribed stimulant (such as methylphenidate). Although 164 were initially recruited for the study, the study excluded 9 individuals (4 in the placebo group, and 5 in the lisdexamfetamine group) who did not start study medication following randomization.
Participants were, on average, 39.4 years of age. And 61% identified as male. Of the full sample, 46% did not complete high school equivalent, whereas 40% had at least trade or vocational school education or higher, with 19% having obtained a university degree. Participants reported an average of 24 days of methamphetamine use in the past 28 days.
WHAT DID THIS STUDY FIND?
The medication reduced methamphetamine use, but only slightly
A total of 100 participants (50 placebo, 50 lisdexamfetamine) completed data collection at the Week 13 time-point, an attrition rate of 39.0%. At the 13 week follow up, those in the placebo condition reported 16 days, on average, of methamphetamine use in the past 28 days, whereas those in the lisdexamfetamine group reported 14 days of methamphetamine use (see Figure below), a non-significant difference. During the full 12-week medication period, however, the medication group had 44 days of methamphetamine use, significantly fewer than the 53 days in the placebo condition (see Figure below). There were no differences between the medication and placebo groups on longest period of abstinence over the study period, percentage achieving 21 consecutive days of abstinence, proportion of negative urine screens (over 12 or the final 4 weeks), participant retainment (at week 5, 9, or 13), craving, amphetamine withdrawal, methamphetamine use severity, or injection use.
Treatment adherence, satisfaction were largely similar, though some additional side effect risk present in medication group
The results suggested higher global satisfaction for the lisdexamfetamine group compared to the placebo. There were no differences in adherence across groups. Participants were more likely to report higher drug liking scores for lisdexamfetamine compared to placebo. Although 73% of participants in the lisdexamfetamine group and 75% of participants in the placebo group experienced adverse events, only 8 were deemed serious adverse events: 5 in the lisdexamfetamine group and 3 in the placebo group. One notable adverse event: the medication group had higher diastolic blood pressure (i.e., when the heart is at rest) at weeks 5 and 8 – though systolic (i.e., when the heart beats) is the blood pressure metric most highly correlated with cardiovascular risk. The most common adverse events were headaches and nausea.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results from this clinical trial found that, over the course of the medication period, those taking lisdexamfetamine used methamphetamine less days compared to those who took placebo, but the groups were not different at the main end-point – the end of the 12-week medication period. One important limitation is that only 60% of the sample made it to the primary outcome analysis. Though the number of participants who dropped out was similar in the 2 groups and the study examined different scenarios finding largely similar results, the study did not check to see if there were any factors that predicted dropout in one group but not the other. It could have been, for example, that those with side effects in the medication group were more likely to drop out of the study than those with side effects in the placebo group. Given that the medication and placebo had largely similar outcome profiles, this type of unbalanced dropout is less of a concern than it would have been if the medication was shown to be helpful with a possibility that dropout – not medication effects – accounted for the observed benefit.
Also, as in many studies comparing a psychoactive medication to placebo, individuals were more likely to correctly guess they were receiving the study medication (i.e., a stimulant medication) than the placebo – potentially accentuating any bias by increasing positive expectancy effects in the medication group and decreasing them in the placebo group once they realized they were not getting the active medication. The advantage of lisdexamfetamine during the 12-week trial therefore should be clarified in further research.
The study only recruited people who used methamphetamine at least half the days in the past month. Although this is an important population with specialized needs, it is unclear if lisdexamfetamine might demonstrate greater efficacy in a sample of people with less severe patterns of use.
As noted above, the attrition rate was notable – only 60% completed the study. While there was no evidence that this dropout impacted interpretation of primary study findings – it might reduce the degree to which the results generalize to individuals with methamphetamine use disorder more generally.
BOTTOM LINE
Lisdexamfetamine, the medication marketed as Vyvanse for ADHD, generally had similar outcomes compared to placebo, with some small advantages for the medication, however when examining total number of methamphetamine use days across the entire trial. Given what appear to be minor side effects of lisdexamfetamine, particularly in context of many unsuccessful efforts to develop and discover useful medications for this disorder, the single positive finding may warrant more rigorous research in a larger sample. Further research may do well also to examine particular subgroups of patients who may respond particularly well to this medication.
For individuals and families seeking recovery: If you or a family member are seeking help for methamphetamine use disorder, more research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer some benefit for methamphetamine use. Other psychosocial treatments, such as contingency management, have been shown to be helpful at increasing abstinence in dozens of studies. It is also important to mention that scientists continue to explore other medication options, with some emerging as potential therapeutics that will be tested in further clinical trials.
For treatment professionals and treatment systems: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer some benefit for patients with methamphetamine use disorder. Other approaches, like contingency management, have demonstrated efficacy while greater overall engagement with treatment and recovery has shown to improve outcomes.
For scientists: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer benefit for patients with methamphetamine use disorder. A larger sample may allow for sub-group analyses including in people with less frequent methamphetamine use and those with co-occurring substance use disorders. Whether medication may be useful in combination with other treatment modalities (such as contingency management) or recovery support services (such as recovery coaches) may also prove fruitful to investigate in future research.
For policy makers: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer benefit for patients with methamphetamine use disorder. Only one positive finding out of many outcomes suggest more rigorous research may be warranted, particularly given what appear to be minor side effects of lisdexamfetamine in context of many unsuccessful efforts to develop and discover useful medications for this disorder. Policies that increase funding to continue investigating lisdexamfetamine, or funding for trials testing lisdexamfetamine in addition to psychosocial treatments, such as contingency management, may also be useful.
Methamphetamine is classified as a Schedule II drug indicating some acceptable medical utility. However, methamphetamine also has significant addictive potential and can lead to substantial toxicity in the brain and body, facilitating the breakdown of skeletal muscle, and inducing seizures and bleeding in the brain at high doses and with chronic use. The past decade has seen a rise in prevalence of methamphetamine use and overdoses involving methamphetamine, particularly in conjunction with opioids.
Psychosocial treatments such as contingency management, a collection of approaches that systematically use incentives to positively reinforce stimulant abstinence (e.g., by providing monetary vouchers to patients for testing negative for stimulant use via urinalysis), are empirically supported for those with methamphetamine use disorder. Additionally, cognitive behavioral therapy (CBT) strategies appear to improve treatment retention.
However, studies have shown that psychosocial treatments are less effective among people with higher levels of methamphetamine use – those using more than half the days in a month, for example. There is a pressing need to identify additional treatment alternatives to enhance treatment efficacy for people who use methamphetamine. Despite decades of medication trials and the public health impact of methamphetamine use, there are no medications approved by the Food and Drug Administration for treating methamphetamine use disorder.
Lisdexamfetamine, an agonist-like stimulant medication also known and marketed by the brand name Vyvanse, is currently FDA-approved to treat attention-deficit hyperactivity disorder (ADHD) and binge-eating disorder. Agonist medications have become increasingly investigated as medications for substance use disorders, in part due to their success in treatment of opioid use disorder over the past few decades. Like other agonist medications, lisdexamfetamine operates similarly to methamphetamine pharmacologically but has a slower onset, longer duration of action, and must be metabolized in the stomach to produce its effects (i.e., it is a ”prodrug” of the medication’s active ingredient) which is thought to reduce the medication’s potential for addiction and other non-medical use. This randomized controlled trial tested the initial efficacy and safety of lisdexamfetamine in reducing methamphetamine use for people with more severe methamphetamine use profiles.
HOW WAS THIS STUDY CONDUCTED?
This study used a randomized double-blind trial to test oral lisdexamfetamine (250 mg daily) in 75 individuals or an identical matched placebo for 80 individuals, all of whom were using methamphetamine at least 14 out of the last 28 days. Participants, who were recruited from 6 Australian treatment clinics specializing in the treatment of stimulant use disorder, underwent a 1-week induction of medication followed by 12 weeks of the medication trial and a 2-week taper. They completed follow-ups at weeks 5, 9, 13, and 19 the latter of which occurred 4 weeks after discontinuing the medication or placebo. In addition to medications, all participants were offered 4 sessions of CBT for methamphetamine use by trained and supervised therapists as consistent with standard care. The primary outcome was the number of days of self-reported methamphetamine use in the past 28 days at the end of the 12-week active medication period (week 13). Secondary outcomes included number of days of self-reported methamphetamine use across the entire 12-week treatment period (possible range = 0–84 days), maximum consecutive abstinence days during treatment period, percentage 21+ consecutive abstinence days at any point during the medication period, percentage of methamphetamine-negative urine tests over 12 weeks and in the last 4 weeks (one a week, with missing tests considered positive), craving, withdrawal, methamphetamine use severity, insomnia, depression, anxiety, stress, quality of life, treatment retention, criminal behavior, and treatment satisfaction.
Participants were eligible for the study: 1) If they met criteria for methamphetamine dependence based on the ICD-10 (consistent with DSM-5 moderate or severe) as determined by an addiction medicine specialist; 2) if they used methamphetamine during more than half of the past 28 days; and 3) if they were not ruled out by any exclusion criteria including, but not limited to, currently taking opioid agonist medication, concurrent severe psychiatric or other medical disorder, other substance use disorder which might interfere with participation in the study, or use of another prescribed stimulant (such as methylphenidate). Although 164 were initially recruited for the study, the study excluded 9 individuals (4 in the placebo group, and 5 in the lisdexamfetamine group) who did not start study medication following randomization.
Participants were, on average, 39.4 years of age. And 61% identified as male. Of the full sample, 46% did not complete high school equivalent, whereas 40% had at least trade or vocational school education or higher, with 19% having obtained a university degree. Participants reported an average of 24 days of methamphetamine use in the past 28 days.
WHAT DID THIS STUDY FIND?
The medication reduced methamphetamine use, but only slightly
A total of 100 participants (50 placebo, 50 lisdexamfetamine) completed data collection at the Week 13 time-point, an attrition rate of 39.0%. At the 13 week follow up, those in the placebo condition reported 16 days, on average, of methamphetamine use in the past 28 days, whereas those in the lisdexamfetamine group reported 14 days of methamphetamine use (see Figure below), a non-significant difference. During the full 12-week medication period, however, the medication group had 44 days of methamphetamine use, significantly fewer than the 53 days in the placebo condition (see Figure below). There were no differences between the medication and placebo groups on longest period of abstinence over the study period, percentage achieving 21 consecutive days of abstinence, proportion of negative urine screens (over 12 or the final 4 weeks), participant retainment (at week 5, 9, or 13), craving, amphetamine withdrawal, methamphetamine use severity, or injection use.
Treatment adherence, satisfaction were largely similar, though some additional side effect risk present in medication group
The results suggested higher global satisfaction for the lisdexamfetamine group compared to the placebo. There were no differences in adherence across groups. Participants were more likely to report higher drug liking scores for lisdexamfetamine compared to placebo. Although 73% of participants in the lisdexamfetamine group and 75% of participants in the placebo group experienced adverse events, only 8 were deemed serious adverse events: 5 in the lisdexamfetamine group and 3 in the placebo group. One notable adverse event: the medication group had higher diastolic blood pressure (i.e., when the heart is at rest) at weeks 5 and 8 – though systolic (i.e., when the heart beats) is the blood pressure metric most highly correlated with cardiovascular risk. The most common adverse events were headaches and nausea.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results from this clinical trial found that, over the course of the medication period, those taking lisdexamfetamine used methamphetamine less days compared to those who took placebo, but the groups were not different at the main end-point – the end of the 12-week medication period. One important limitation is that only 60% of the sample made it to the primary outcome analysis. Though the number of participants who dropped out was similar in the 2 groups and the study examined different scenarios finding largely similar results, the study did not check to see if there were any factors that predicted dropout in one group but not the other. It could have been, for example, that those with side effects in the medication group were more likely to drop out of the study than those with side effects in the placebo group. Given that the medication and placebo had largely similar outcome profiles, this type of unbalanced dropout is less of a concern than it would have been if the medication was shown to be helpful with a possibility that dropout – not medication effects – accounted for the observed benefit.
Also, as in many studies comparing a psychoactive medication to placebo, individuals were more likely to correctly guess they were receiving the study medication (i.e., a stimulant medication) than the placebo – potentially accentuating any bias by increasing positive expectancy effects in the medication group and decreasing them in the placebo group once they realized they were not getting the active medication. The advantage of lisdexamfetamine during the 12-week trial therefore should be clarified in further research.
The study only recruited people who used methamphetamine at least half the days in the past month. Although this is an important population with specialized needs, it is unclear if lisdexamfetamine might demonstrate greater efficacy in a sample of people with less severe patterns of use.
As noted above, the attrition rate was notable – only 60% completed the study. While there was no evidence that this dropout impacted interpretation of primary study findings – it might reduce the degree to which the results generalize to individuals with methamphetamine use disorder more generally.
BOTTOM LINE
Lisdexamfetamine, the medication marketed as Vyvanse for ADHD, generally had similar outcomes compared to placebo, with some small advantages for the medication, however when examining total number of methamphetamine use days across the entire trial. Given what appear to be minor side effects of lisdexamfetamine, particularly in context of many unsuccessful efforts to develop and discover useful medications for this disorder, the single positive finding may warrant more rigorous research in a larger sample. Further research may do well also to examine particular subgroups of patients who may respond particularly well to this medication.
For individuals and families seeking recovery: If you or a family member are seeking help for methamphetamine use disorder, more research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer some benefit for methamphetamine use. Other psychosocial treatments, such as contingency management, have been shown to be helpful at increasing abstinence in dozens of studies. It is also important to mention that scientists continue to explore other medication options, with some emerging as potential therapeutics that will be tested in further clinical trials.
For treatment professionals and treatment systems: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer some benefit for patients with methamphetamine use disorder. Other approaches, like contingency management, have demonstrated efficacy while greater overall engagement with treatment and recovery has shown to improve outcomes.
For scientists: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer benefit for patients with methamphetamine use disorder. A larger sample may allow for sub-group analyses including in people with less frequent methamphetamine use and those with co-occurring substance use disorders. Whether medication may be useful in combination with other treatment modalities (such as contingency management) or recovery support services (such as recovery coaches) may also prove fruitful to investigate in future research.
For policy makers: More research is needed to determine whether lisdexamfetamine, the medication marketed as Vyvanse for ADHD, may offer benefit for patients with methamphetamine use disorder. Only one positive finding out of many outcomes suggest more rigorous research may be warranted, particularly given what appear to be minor side effects of lisdexamfetamine in context of many unsuccessful efforts to develop and discover useful medications for this disorder. Policies that increase funding to continue investigating lisdexamfetamine, or funding for trials testing lisdexamfetamine in addition to psychosocial treatments, such as contingency management, may also be useful.