How do depression and anxiety change during treatment for alcohol use disorder?
Symptoms of depression and anxiety are commonly experienced by people with alcohol use disorder. While, in general, these symptoms usually decrease substantially in the first month of treatment, this is not the case for everyone. This study identified different subgroups of people in early abstinence receiving treatment in a community substance use treatment program based on their changes in anxiety and depression.
Compared to the general population, people who have alcohol use disorder are also more likely to experience symptoms of depression and anxiety. This is in part because people who are experiencing anxiety and depression may use alcohol to alleviate symptoms or to experience the euphoric effects of alcohol, providing brief periods of relief or reward that may be absent when anxious or depressed. Alternatively, alcohol use disorder may lead to conflicts with family and friends, job loss, or may interfere with other ways that may increase life stress that can lead to symptoms of depression or anxiety.
Alcohol also affects parts of the brain responsible for anxiety management, and heavy alcohol use over time makes it more difficult to manage anxiety. As a result, a significant proportion of people attempting to stop their alcohol use report elevated levels of anxiety and depression, symptoms which may be exacerbated by factors often present in initial recovery. These include acute and post-acute withdrawal, associated with brain changes (neuroadaptations) that can lead to loss of pleasure experiences (anhedonia). These factors may also include reductions in the amount, and nature of, social support, during the interim period when people shift from substance using peer networks to recovery-oriented peer networks. Such symptoms may increase risk fora return to alcohol use. Although some studies show that symptoms of anxiety and depression reduce significantly over the first month, these studies report average change across a large number of people and do not account for the potential presence of different patterns among different people. For some people, anxiety or depression may stay at high levels throughout early abstinence, potentially requiring additional attention and treatment; for others, anxiety and depression may reduce rapidly alongside alcohol abstinence in the first few weeks. These different patterns are important to characterize because they may be associated with different treatment needs and remission outcomes. This study identified different subgroups of changes in anxiety and depression among people who are in early abstinence receiving treatment in a community substance use treatment program.
HOW WAS THIS STUDY CONDUCTED?
The study was conducted using a retrospective cohort study design. The researchers extracted longitudinal electric health record data for 1,005 patients receiving treatment at a large “community treatment” program. The researchers used data from all people receiving treatment for alcohol use disorder who were admitted for treatment between January 1, 2020, and December 30, 2020.
Patients in treatment at the facility completed weekly measures of depression and anxiety. Data on symptoms of posttraumatic stress disorder were also collected at a single time point, most typically during the first week of treatment. The researchers were also able to extract certain data from the electronic health record, including age, self-reported gender, and race. Clinicians conducted a clinical interview to determine presence or absence of current co-occuring mental health and substance use disorders, broadly defined, at the time of the interview. The researchers primarily wanted to characterize the change in anxiety and depression symptoms over the first 6 weeks of treatment, and then see if distinct patterns of change emerged across the sample. To do this, the authors used a complex statistical approach that examines whether anxiety and depression change differently for different groups of people. After the researchers determined the number of different change trajectories, they then looked to see if people in each group differed from other groups in symptoms of posttraumatic stress disorder, gender, race, age, and the presence of co-occurring disorders.
The sample was 68.2% male and 31.8% female; 90.1% were White, 5.3% were Black, 1.7% were Hispanic, and 2.9% were categorized as “Other”. In addition to primary alcohol use disorder, based on unstructured clinical program assessment interviews, 33.9% were diagnosed with current depressive disorder, 25.9% with anxiety disorder, 6.2% with posttraumatic stress disorder, 3.9% with bipolar disorder, and 3.6% with attention deficit/hyperactivity disorder. Further, 2.3% were diagnosed with an amphetamine use disorder, 14.5% with cannabis use disorder, 7.6% with opioid use disorder, 5.1% with sedative use disorder, 1.6% with stimulant use disorder, and 4.5% with tobacco use disorder. Due to the low number of cases with co-occurring substance use disorders (in addition to alcohol use disorder), the researchers only examined subgroup differences for cannabis use disorder and opioid use disorder.
WHAT DID THIS STUDY FIND?
Anxiety and depression decreased overall, but different patterns of change emerged
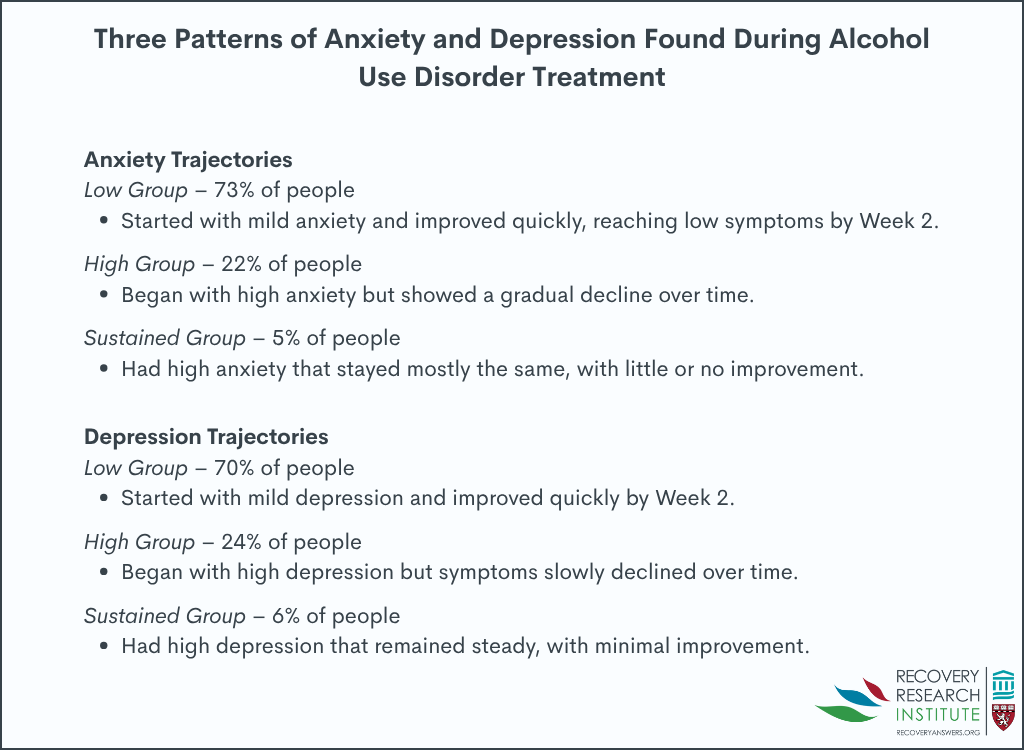
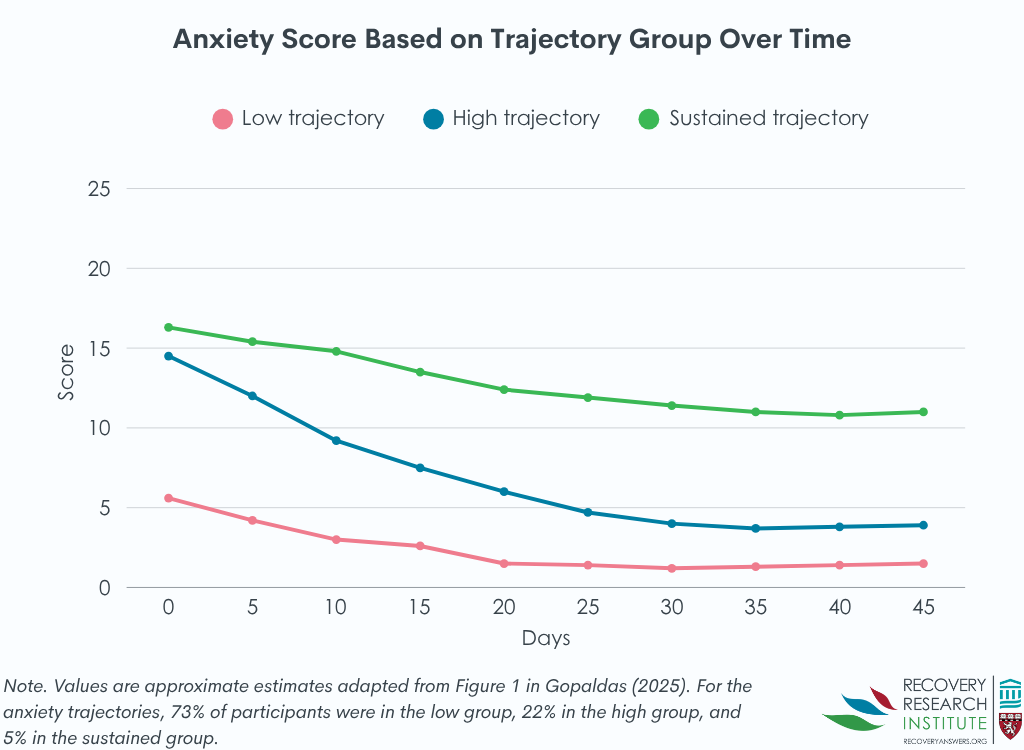
Overall, symptoms of anxiety and depression decreased by week 2 and remained low for the remainder of the 6 weeks. As described in the graphic below, 3 subgroups of change in anxiety symptoms emerged. In the largest group that accounted for 73% of the sample (the “low” group), anxiety started low, decreased slightly over the first three weeks, and then remained low during the remainder of treatment. In the second group which included 22% of the sample (the “high decreasing” group), anxiety symptoms started above the clinical cutoff but decreased quickly over the first three weeks, leveling out around week 4. In the third group which included 5% of the sample (the “sustained” group), anxiety symptoms started above the clinical cutoff, reducing slightly over the first 5 weeks but remaining on average above the clinical cutoff.
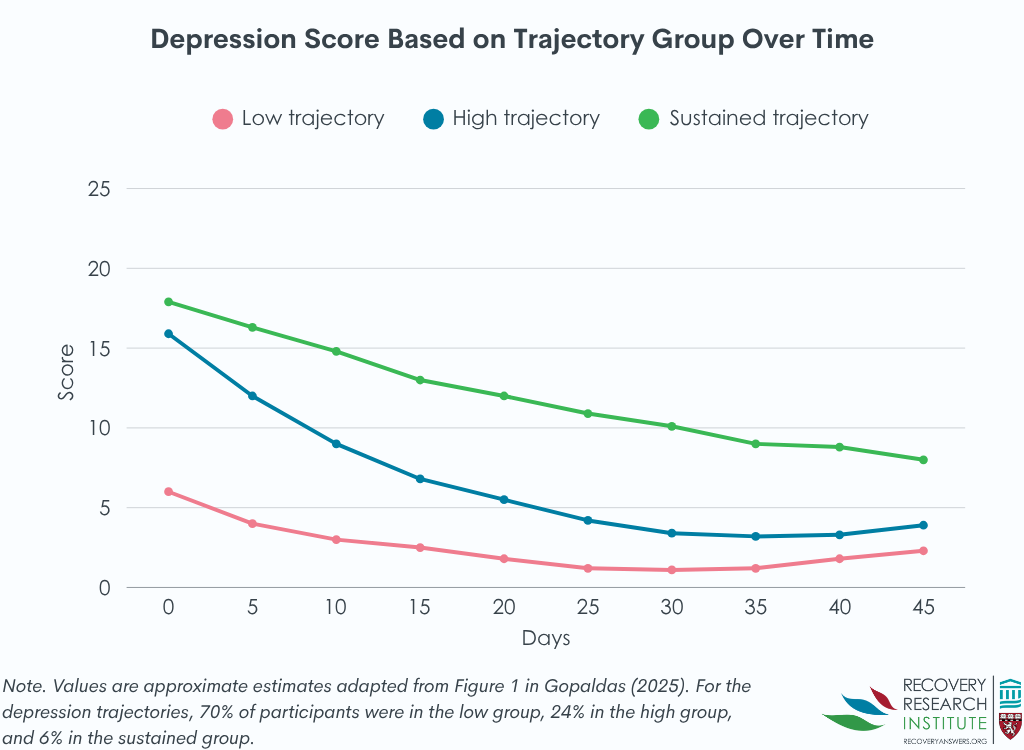
Also as described in the graphic below, 3 subgroups for depression trajectories also emerged. In the largest group accounting for 70% of the sample, depression started low, decreased slightly over the first three weeks, and then remained low during the remainder of treatment. In the second group accounting for 24% of the sample, depression symptoms started above the clinical cutoff but decreased quickly over the first three weeks, leveling out around week 4. In the third group which included 5% of the sample, depression symptoms started above the clinical cutoff but reduced consistently across the study period, resulting in scores below the clinical cutoff on average.
As is commonly observed clinically, there was a high degree of overlap between depression and anxiety group membership. Of those in the low anxiety group, 87% were also in the low depression group. Similarly, 60% of those in the high decreasing anxiety subgroup were also in the high decreasing depression subgroup, and 53% of those in the sustained trajectory anxiety group were also in the sustained trajectory depression group.
Subgroups of anxiety and depression trajectories had differing demographic and clinical profiles
Important demographic and clinical demographics emerged across anxiety change subgroups. Those in the high decreasing group were older on average than those in the sustained high group, but younger than those in the low group. Those in the low group had the lowest depression and PTSD scores, followed by the high decreasing group and the sustained group (see graph below). Co-occurring cannabis use disorder was highest in the sustained group, followed by the high decreasing group and the low group. There were no differences in sex or racial makeup, or rates of opioid use disorder, across the three different groups.
There were also important demographic and clinical demographics that emerged across depression change subgroups. There were a greater proportion of males in the low group relative to the high decreasing and sustained groups. Those in the high decreasing group were older on average than those in the sustained high group, but younger than those in the low group. Those in the low group had the lowest anxiety and PTSD scores, followed by the high decreasing group and the sustained group (see graph below). Co-occurring cannabis use disorder and opioid use disorder was highest in the sustained group, followed by the high decreasing group and the low group. There were no differences in race across the three different depression change groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Anxiety and depression decreased across the first month of treatment, highlighting significant relief during a critical period of risk for return to use. However, the results highlight that some of the sample started with elevated anxiety that remained above clinical thresholds across the period. This group tended to be younger and had higher rates of co-occuring mental health and substance use disorders. These data suggest a profile of people that broadly demonstrate greater complexity and may need more comprehensive and expansive treatment and/or access to additional resources. Although people in this group did experience some alleviation of anxiety symptoms, the stable elevation of these symptoms above clinical thresholds suggests that individuals in this profile are still experiencing significant discomfort or suffering after 6 weeks. It is unclear why this group sustained high levels of anxiety. One possibility is that the anxiety symptoms preceded the alcohol use disorder and is independent of alcohol use. So, reducing alcohol use, while providing some symptom relief related to alcohol, does not fully alleviate the existing anxiety symptomatology, which may need additional independent focus in treatment. On the other hand, the majority of the sample had low rates of anxiety symptoms that declined even further over the first 6 weeks, and approximately one quarter of the sample experienced significant reductions in anxiety symptoms, despite starting with symptom levels that were similar to the highest, sustained anxiety group. Anxiety symptoms in this group may have emerged primarily from their alcohol use disorder, and as a result abstinence is associated with rapidly declining rates symptoms of anxiety. The therapeutic environment itself provided by treatment also can help alleviate and reduce anxiety and boost self-efficacy and agency reducing symptoms further. More research is needed to determine the mechanisms behind these different group memberships, which may help improve tailored treatment approaches.
The analyses also revealed a low and high decreasing group for depressive symptoms that were similar to the low and high decreasing anxiety symptom groups. However, the most severe group demonstrated greater sustained change over the 6 week period, with the average depressive symptoms at the end of 6 weeks dipping below the clinical threshold. As such, the sustained group and the high decreasing group both started and ended at similar levels of depressive symptoms and were primarily distinguished by the pattern of change, with the high decreasing group rapidly reducing in the first few weeks and leveling out, and the sustained group experiencing stable declines over the entire period. While encouraging that the sustained group did see big declines over the 6 week period, the few weeks of additional elevated depressive symptoms may make the difference between successful sustained abstinence and return to use during this critical period.
An important limitation of the current study was that it did not include data about return to use or substance use during the treatment episode, so it is unclear whether substance use might interfere with these depression and anxiety trajectories, or whether change trajectories might highlight differences in abstinence rates across the first 6 weeks. However, past research suggests that greater anxiety/depression symptom severity is associated with worse outcomes, which suggests that the sustained high groups may be more likely to return to use during this early phase or over the ensuing months. More research will be needed to see how these profiles are related to substance use among alcohol use disorder patients with these types of characteristics.
The researchers did not report data about alcohol or other substance use, so it is unclear whether trajectories might differ in part based on the patients use over time.
The sample was predominantly White and male, and trajectories may differ in samples with higher proportion of women or people with a minoritized identity.
The sample was derived from a private “community program”. It is unclear whether participants were recruited from outpatient settings, inpatient settings, or both.
BOTTOM LINE
As found in prior research, although anxiety and depression can be a significant barrier to sustained abstinence in the first month of treatment for many, these symptoms may decline rapidly alongside alcohol abstinence, providing much needed relief. However, there are different patterns of change, and some have levels of depressive or anxiety symptoms that remain high. Those whose symptoms remain high over the course of the first month of abstinence are more likely to be younger and have co-occurring mental health or substance use disorders. From a stress and coping theory perspective, such individuals may be at higher risk for return to use and may require more comprehensive services to address independent anxiety/depression disorders.
For individuals and families seeking recovery: Many people experience anxiety or depression in the early days of a recovery journey. If you are experiencing this, these findings suggest that you are likely to experience some relief in the first 6 weeks while stopping alcohol use. However, if you have elevated symptoms, and also meet criteria for posttraumatic stress disorder or another substance use disorder, you may be less likely to see as large reductions, or at least as rapidly over the first few weeks of initial abstinence. People with this pattern may wish to consider additional treatment that can address these other challenges.
For treatment professionals and treatment systems: If you treat patients with alcohol use disorder who wish to cease alcohol use, significant anxiety or depressive symptoms may impede achievement of that goal during the initial recovery phases. It is important to asses for anxiety and depression in order to better understand the needs of the patient. Further, those with comorbidities such as co-occuring posttraumatic stress disorder or other substance use disorders may be more likely to have sustained symptoms of depression or anxiety during the initial treatment episode, which may require more additional treatment focused specifically on addressing these other challenges.
For scientists: These data suggest that there are distinct profiles of change in anxiety and depression over the first 6 weeks of initial abstinence in a treatment setting. Future research may consider examining associations between change profiles and substance use outcomes, or even substance use severity at the start of treatment. Further, although a substantive portion of people initiating recovery return to use in the first month, the risk remains elevated particularly across the first year. Future studies that examine trajectories over a full year may reveal alternative patterns of change that can further individualize treatment approaches. Finally, the data from this study are unable to reveal the mechanisms underlying these profiles. Future research may attempt to uncover why people fall into each of the anxiety and depression subgroups.
For policy makers: These data highlight the significant barriers people with alcohol use disorder face as they attempt to make changes to their alcohol use. Policies that increase access to treatment or recovery support services is likely to alleviate symptoms and increase remission success. Further, funding for research in the intersection between anxiety and depression and alcohol use disorder may provide more targeted approaches for managing these commonly co-occurring conditions.
Compared to the general population, people who have alcohol use disorder are also more likely to experience symptoms of depression and anxiety. This is in part because people who are experiencing anxiety and depression may use alcohol to alleviate symptoms or to experience the euphoric effects of alcohol, providing brief periods of relief or reward that may be absent when anxious or depressed. Alternatively, alcohol use disorder may lead to conflicts with family and friends, job loss, or may interfere with other ways that may increase life stress that can lead to symptoms of depression or anxiety.
Alcohol also affects parts of the brain responsible for anxiety management, and heavy alcohol use over time makes it more difficult to manage anxiety. As a result, a significant proportion of people attempting to stop their alcohol use report elevated levels of anxiety and depression, symptoms which may be exacerbated by factors often present in initial recovery. These include acute and post-acute withdrawal, associated with brain changes (neuroadaptations) that can lead to loss of pleasure experiences (anhedonia). These factors may also include reductions in the amount, and nature of, social support, during the interim period when people shift from substance using peer networks to recovery-oriented peer networks. Such symptoms may increase risk fora return to alcohol use. Although some studies show that symptoms of anxiety and depression reduce significantly over the first month, these studies report average change across a large number of people and do not account for the potential presence of different patterns among different people. For some people, anxiety or depression may stay at high levels throughout early abstinence, potentially requiring additional attention and treatment; for others, anxiety and depression may reduce rapidly alongside alcohol abstinence in the first few weeks. These different patterns are important to characterize because they may be associated with different treatment needs and remission outcomes. This study identified different subgroups of changes in anxiety and depression among people who are in early abstinence receiving treatment in a community substance use treatment program.
HOW WAS THIS STUDY CONDUCTED?
The study was conducted using a retrospective cohort study design. The researchers extracted longitudinal electric health record data for 1,005 patients receiving treatment at a large “community treatment” program. The researchers used data from all people receiving treatment for alcohol use disorder who were admitted for treatment between January 1, 2020, and December 30, 2020.
Patients in treatment at the facility completed weekly measures of depression and anxiety. Data on symptoms of posttraumatic stress disorder were also collected at a single time point, most typically during the first week of treatment. The researchers were also able to extract certain data from the electronic health record, including age, self-reported gender, and race. Clinicians conducted a clinical interview to determine presence or absence of current co-occuring mental health and substance use disorders, broadly defined, at the time of the interview. The researchers primarily wanted to characterize the change in anxiety and depression symptoms over the first 6 weeks of treatment, and then see if distinct patterns of change emerged across the sample. To do this, the authors used a complex statistical approach that examines whether anxiety and depression change differently for different groups of people. After the researchers determined the number of different change trajectories, they then looked to see if people in each group differed from other groups in symptoms of posttraumatic stress disorder, gender, race, age, and the presence of co-occurring disorders.
The sample was 68.2% male and 31.8% female; 90.1% were White, 5.3% were Black, 1.7% were Hispanic, and 2.9% were categorized as “Other”. In addition to primary alcohol use disorder, based on unstructured clinical program assessment interviews, 33.9% were diagnosed with current depressive disorder, 25.9% with anxiety disorder, 6.2% with posttraumatic stress disorder, 3.9% with bipolar disorder, and 3.6% with attention deficit/hyperactivity disorder. Further, 2.3% were diagnosed with an amphetamine use disorder, 14.5% with cannabis use disorder, 7.6% with opioid use disorder, 5.1% with sedative use disorder, 1.6% with stimulant use disorder, and 4.5% with tobacco use disorder. Due to the low number of cases with co-occurring substance use disorders (in addition to alcohol use disorder), the researchers only examined subgroup differences for cannabis use disorder and opioid use disorder.
WHAT DID THIS STUDY FIND?
Anxiety and depression decreased overall, but different patterns of change emerged
Overall, symptoms of anxiety and depression decreased by week 2 and remained low for the remainder of the 6 weeks. As described in the graphic below, 3 subgroups of change in anxiety symptoms emerged. In the largest group that accounted for 73% of the sample (the “low” group), anxiety started low, decreased slightly over the first three weeks, and then remained low during the remainder of treatment. In the second group which included 22% of the sample (the “high decreasing” group), anxiety symptoms started above the clinical cutoff but decreased quickly over the first three weeks, leveling out around week 4. In the third group which included 5% of the sample (the “sustained” group), anxiety symptoms started above the clinical cutoff, reducing slightly over the first 5 weeks but remaining on average above the clinical cutoff.
Also as described in the graphic below, 3 subgroups for depression trajectories also emerged. In the largest group accounting for 70% of the sample, depression started low, decreased slightly over the first three weeks, and then remained low during the remainder of treatment. In the second group accounting for 24% of the sample, depression symptoms started above the clinical cutoff but decreased quickly over the first three weeks, leveling out around week 4. In the third group which included 5% of the sample, depression symptoms started above the clinical cutoff but reduced consistently across the study period, resulting in scores below the clinical cutoff on average.
As is commonly observed clinically, there was a high degree of overlap between depression and anxiety group membership. Of those in the low anxiety group, 87% were also in the low depression group. Similarly, 60% of those in the high decreasing anxiety subgroup were also in the high decreasing depression subgroup, and 53% of those in the sustained trajectory anxiety group were also in the sustained trajectory depression group.
Subgroups of anxiety and depression trajectories had differing demographic and clinical profiles
Important demographic and clinical demographics emerged across anxiety change subgroups. Those in the high decreasing group were older on average than those in the sustained high group, but younger than those in the low group. Those in the low group had the lowest depression and PTSD scores, followed by the high decreasing group and the sustained group (see graph below). Co-occurring cannabis use disorder was highest in the sustained group, followed by the high decreasing group and the low group. There were no differences in sex or racial makeup, or rates of opioid use disorder, across the three different groups.
There were also important demographic and clinical demographics that emerged across depression change subgroups. There were a greater proportion of males in the low group relative to the high decreasing and sustained groups. Those in the high decreasing group were older on average than those in the sustained high group, but younger than those in the low group. Those in the low group had the lowest anxiety and PTSD scores, followed by the high decreasing group and the sustained group (see graph below). Co-occurring cannabis use disorder and opioid use disorder was highest in the sustained group, followed by the high decreasing group and the low group. There were no differences in race across the three different depression change groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Anxiety and depression decreased across the first month of treatment, highlighting significant relief during a critical period of risk for return to use. However, the results highlight that some of the sample started with elevated anxiety that remained above clinical thresholds across the period. This group tended to be younger and had higher rates of co-occuring mental health and substance use disorders. These data suggest a profile of people that broadly demonstrate greater complexity and may need more comprehensive and expansive treatment and/or access to additional resources. Although people in this group did experience some alleviation of anxiety symptoms, the stable elevation of these symptoms above clinical thresholds suggests that individuals in this profile are still experiencing significant discomfort or suffering after 6 weeks. It is unclear why this group sustained high levels of anxiety. One possibility is that the anxiety symptoms preceded the alcohol use disorder and is independent of alcohol use. So, reducing alcohol use, while providing some symptom relief related to alcohol, does not fully alleviate the existing anxiety symptomatology, which may need additional independent focus in treatment. On the other hand, the majority of the sample had low rates of anxiety symptoms that declined even further over the first 6 weeks, and approximately one quarter of the sample experienced significant reductions in anxiety symptoms, despite starting with symptom levels that were similar to the highest, sustained anxiety group. Anxiety symptoms in this group may have emerged primarily from their alcohol use disorder, and as a result abstinence is associated with rapidly declining rates symptoms of anxiety. The therapeutic environment itself provided by treatment also can help alleviate and reduce anxiety and boost self-efficacy and agency reducing symptoms further. More research is needed to determine the mechanisms behind these different group memberships, which may help improve tailored treatment approaches.
The analyses also revealed a low and high decreasing group for depressive symptoms that were similar to the low and high decreasing anxiety symptom groups. However, the most severe group demonstrated greater sustained change over the 6 week period, with the average depressive symptoms at the end of 6 weeks dipping below the clinical threshold. As such, the sustained group and the high decreasing group both started and ended at similar levels of depressive symptoms and were primarily distinguished by the pattern of change, with the high decreasing group rapidly reducing in the first few weeks and leveling out, and the sustained group experiencing stable declines over the entire period. While encouraging that the sustained group did see big declines over the 6 week period, the few weeks of additional elevated depressive symptoms may make the difference between successful sustained abstinence and return to use during this critical period.
An important limitation of the current study was that it did not include data about return to use or substance use during the treatment episode, so it is unclear whether substance use might interfere with these depression and anxiety trajectories, or whether change trajectories might highlight differences in abstinence rates across the first 6 weeks. However, past research suggests that greater anxiety/depression symptom severity is associated with worse outcomes, which suggests that the sustained high groups may be more likely to return to use during this early phase or over the ensuing months. More research will be needed to see how these profiles are related to substance use among alcohol use disorder patients with these types of characteristics.
The researchers did not report data about alcohol or other substance use, so it is unclear whether trajectories might differ in part based on the patients use over time.
The sample was predominantly White and male, and trajectories may differ in samples with higher proportion of women or people with a minoritized identity.
The sample was derived from a private “community program”. It is unclear whether participants were recruited from outpatient settings, inpatient settings, or both.
BOTTOM LINE
As found in prior research, although anxiety and depression can be a significant barrier to sustained abstinence in the first month of treatment for many, these symptoms may decline rapidly alongside alcohol abstinence, providing much needed relief. However, there are different patterns of change, and some have levels of depressive or anxiety symptoms that remain high. Those whose symptoms remain high over the course of the first month of abstinence are more likely to be younger and have co-occurring mental health or substance use disorders. From a stress and coping theory perspective, such individuals may be at higher risk for return to use and may require more comprehensive services to address independent anxiety/depression disorders.
For individuals and families seeking recovery: Many people experience anxiety or depression in the early days of a recovery journey. If you are experiencing this, these findings suggest that you are likely to experience some relief in the first 6 weeks while stopping alcohol use. However, if you have elevated symptoms, and also meet criteria for posttraumatic stress disorder or another substance use disorder, you may be less likely to see as large reductions, or at least as rapidly over the first few weeks of initial abstinence. People with this pattern may wish to consider additional treatment that can address these other challenges.
For treatment professionals and treatment systems: If you treat patients with alcohol use disorder who wish to cease alcohol use, significant anxiety or depressive symptoms may impede achievement of that goal during the initial recovery phases. It is important to asses for anxiety and depression in order to better understand the needs of the patient. Further, those with comorbidities such as co-occuring posttraumatic stress disorder or other substance use disorders may be more likely to have sustained symptoms of depression or anxiety during the initial treatment episode, which may require more additional treatment focused specifically on addressing these other challenges.
For scientists: These data suggest that there are distinct profiles of change in anxiety and depression over the first 6 weeks of initial abstinence in a treatment setting. Future research may consider examining associations between change profiles and substance use outcomes, or even substance use severity at the start of treatment. Further, although a substantive portion of people initiating recovery return to use in the first month, the risk remains elevated particularly across the first year. Future studies that examine trajectories over a full year may reveal alternative patterns of change that can further individualize treatment approaches. Finally, the data from this study are unable to reveal the mechanisms underlying these profiles. Future research may attempt to uncover why people fall into each of the anxiety and depression subgroups.
For policy makers: These data highlight the significant barriers people with alcohol use disorder face as they attempt to make changes to their alcohol use. Policies that increase access to treatment or recovery support services is likely to alleviate symptoms and increase remission success. Further, funding for research in the intersection between anxiety and depression and alcohol use disorder may provide more targeted approaches for managing these commonly co-occurring conditions.
Compared to the general population, people who have alcohol use disorder are also more likely to experience symptoms of depression and anxiety. This is in part because people who are experiencing anxiety and depression may use alcohol to alleviate symptoms or to experience the euphoric effects of alcohol, providing brief periods of relief or reward that may be absent when anxious or depressed. Alternatively, alcohol use disorder may lead to conflicts with family and friends, job loss, or may interfere with other ways that may increase life stress that can lead to symptoms of depression or anxiety.
Alcohol also affects parts of the brain responsible for anxiety management, and heavy alcohol use over time makes it more difficult to manage anxiety. As a result, a significant proportion of people attempting to stop their alcohol use report elevated levels of anxiety and depression, symptoms which may be exacerbated by factors often present in initial recovery. These include acute and post-acute withdrawal, associated with brain changes (neuroadaptations) that can lead to loss of pleasure experiences (anhedonia). These factors may also include reductions in the amount, and nature of, social support, during the interim period when people shift from substance using peer networks to recovery-oriented peer networks. Such symptoms may increase risk fora return to alcohol use. Although some studies show that symptoms of anxiety and depression reduce significantly over the first month, these studies report average change across a large number of people and do not account for the potential presence of different patterns among different people. For some people, anxiety or depression may stay at high levels throughout early abstinence, potentially requiring additional attention and treatment; for others, anxiety and depression may reduce rapidly alongside alcohol abstinence in the first few weeks. These different patterns are important to characterize because they may be associated with different treatment needs and remission outcomes. This study identified different subgroups of changes in anxiety and depression among people who are in early abstinence receiving treatment in a community substance use treatment program.
HOW WAS THIS STUDY CONDUCTED?
The study was conducted using a retrospective cohort study design. The researchers extracted longitudinal electric health record data for 1,005 patients receiving treatment at a large “community treatment” program. The researchers used data from all people receiving treatment for alcohol use disorder who were admitted for treatment between January 1, 2020, and December 30, 2020.
Patients in treatment at the facility completed weekly measures of depression and anxiety. Data on symptoms of posttraumatic stress disorder were also collected at a single time point, most typically during the first week of treatment. The researchers were also able to extract certain data from the electronic health record, including age, self-reported gender, and race. Clinicians conducted a clinical interview to determine presence or absence of current co-occuring mental health and substance use disorders, broadly defined, at the time of the interview. The researchers primarily wanted to characterize the change in anxiety and depression symptoms over the first 6 weeks of treatment, and then see if distinct patterns of change emerged across the sample. To do this, the authors used a complex statistical approach that examines whether anxiety and depression change differently for different groups of people. After the researchers determined the number of different change trajectories, they then looked to see if people in each group differed from other groups in symptoms of posttraumatic stress disorder, gender, race, age, and the presence of co-occurring disorders.
The sample was 68.2% male and 31.8% female; 90.1% were White, 5.3% were Black, 1.7% were Hispanic, and 2.9% were categorized as “Other”. In addition to primary alcohol use disorder, based on unstructured clinical program assessment interviews, 33.9% were diagnosed with current depressive disorder, 25.9% with anxiety disorder, 6.2% with posttraumatic stress disorder, 3.9% with bipolar disorder, and 3.6% with attention deficit/hyperactivity disorder. Further, 2.3% were diagnosed with an amphetamine use disorder, 14.5% with cannabis use disorder, 7.6% with opioid use disorder, 5.1% with sedative use disorder, 1.6% with stimulant use disorder, and 4.5% with tobacco use disorder. Due to the low number of cases with co-occurring substance use disorders (in addition to alcohol use disorder), the researchers only examined subgroup differences for cannabis use disorder and opioid use disorder.
WHAT DID THIS STUDY FIND?
Anxiety and depression decreased overall, but different patterns of change emerged
Overall, symptoms of anxiety and depression decreased by week 2 and remained low for the remainder of the 6 weeks. As described in the graphic below, 3 subgroups of change in anxiety symptoms emerged. In the largest group that accounted for 73% of the sample (the “low” group), anxiety started low, decreased slightly over the first three weeks, and then remained low during the remainder of treatment. In the second group which included 22% of the sample (the “high decreasing” group), anxiety symptoms started above the clinical cutoff but decreased quickly over the first three weeks, leveling out around week 4. In the third group which included 5% of the sample (the “sustained” group), anxiety symptoms started above the clinical cutoff, reducing slightly over the first 5 weeks but remaining on average above the clinical cutoff.
Also as described in the graphic below, 3 subgroups for depression trajectories also emerged. In the largest group accounting for 70% of the sample, depression started low, decreased slightly over the first three weeks, and then remained low during the remainder of treatment. In the second group accounting for 24% of the sample, depression symptoms started above the clinical cutoff but decreased quickly over the first three weeks, leveling out around week 4. In the third group which included 5% of the sample, depression symptoms started above the clinical cutoff but reduced consistently across the study period, resulting in scores below the clinical cutoff on average.
As is commonly observed clinically, there was a high degree of overlap between depression and anxiety group membership. Of those in the low anxiety group, 87% were also in the low depression group. Similarly, 60% of those in the high decreasing anxiety subgroup were also in the high decreasing depression subgroup, and 53% of those in the sustained trajectory anxiety group were also in the sustained trajectory depression group.
Subgroups of anxiety and depression trajectories had differing demographic and clinical profiles
Important demographic and clinical demographics emerged across anxiety change subgroups. Those in the high decreasing group were older on average than those in the sustained high group, but younger than those in the low group. Those in the low group had the lowest depression and PTSD scores, followed by the high decreasing group and the sustained group (see graph below). Co-occurring cannabis use disorder was highest in the sustained group, followed by the high decreasing group and the low group. There were no differences in sex or racial makeup, or rates of opioid use disorder, across the three different groups.
There were also important demographic and clinical demographics that emerged across depression change subgroups. There were a greater proportion of males in the low group relative to the high decreasing and sustained groups. Those in the high decreasing group were older on average than those in the sustained high group, but younger than those in the low group. Those in the low group had the lowest anxiety and PTSD scores, followed by the high decreasing group and the sustained group (see graph below). Co-occurring cannabis use disorder and opioid use disorder was highest in the sustained group, followed by the high decreasing group and the low group. There were no differences in race across the three different depression change groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Anxiety and depression decreased across the first month of treatment, highlighting significant relief during a critical period of risk for return to use. However, the results highlight that some of the sample started with elevated anxiety that remained above clinical thresholds across the period. This group tended to be younger and had higher rates of co-occuring mental health and substance use disorders. These data suggest a profile of people that broadly demonstrate greater complexity and may need more comprehensive and expansive treatment and/or access to additional resources. Although people in this group did experience some alleviation of anxiety symptoms, the stable elevation of these symptoms above clinical thresholds suggests that individuals in this profile are still experiencing significant discomfort or suffering after 6 weeks. It is unclear why this group sustained high levels of anxiety. One possibility is that the anxiety symptoms preceded the alcohol use disorder and is independent of alcohol use. So, reducing alcohol use, while providing some symptom relief related to alcohol, does not fully alleviate the existing anxiety symptomatology, which may need additional independent focus in treatment. On the other hand, the majority of the sample had low rates of anxiety symptoms that declined even further over the first 6 weeks, and approximately one quarter of the sample experienced significant reductions in anxiety symptoms, despite starting with symptom levels that were similar to the highest, sustained anxiety group. Anxiety symptoms in this group may have emerged primarily from their alcohol use disorder, and as a result abstinence is associated with rapidly declining rates symptoms of anxiety. The therapeutic environment itself provided by treatment also can help alleviate and reduce anxiety and boost self-efficacy and agency reducing symptoms further. More research is needed to determine the mechanisms behind these different group memberships, which may help improve tailored treatment approaches.
The analyses also revealed a low and high decreasing group for depressive symptoms that were similar to the low and high decreasing anxiety symptom groups. However, the most severe group demonstrated greater sustained change over the 6 week period, with the average depressive symptoms at the end of 6 weeks dipping below the clinical threshold. As such, the sustained group and the high decreasing group both started and ended at similar levels of depressive symptoms and were primarily distinguished by the pattern of change, with the high decreasing group rapidly reducing in the first few weeks and leveling out, and the sustained group experiencing stable declines over the entire period. While encouraging that the sustained group did see big declines over the 6 week period, the few weeks of additional elevated depressive symptoms may make the difference between successful sustained abstinence and return to use during this critical period.
An important limitation of the current study was that it did not include data about return to use or substance use during the treatment episode, so it is unclear whether substance use might interfere with these depression and anxiety trajectories, or whether change trajectories might highlight differences in abstinence rates across the first 6 weeks. However, past research suggests that greater anxiety/depression symptom severity is associated with worse outcomes, which suggests that the sustained high groups may be more likely to return to use during this early phase or over the ensuing months. More research will be needed to see how these profiles are related to substance use among alcohol use disorder patients with these types of characteristics.
The researchers did not report data about alcohol or other substance use, so it is unclear whether trajectories might differ in part based on the patients use over time.
The sample was predominantly White and male, and trajectories may differ in samples with higher proportion of women or people with a minoritized identity.
The sample was derived from a private “community program”. It is unclear whether participants were recruited from outpatient settings, inpatient settings, or both.
BOTTOM LINE
As found in prior research, although anxiety and depression can be a significant barrier to sustained abstinence in the first month of treatment for many, these symptoms may decline rapidly alongside alcohol abstinence, providing much needed relief. However, there are different patterns of change, and some have levels of depressive or anxiety symptoms that remain high. Those whose symptoms remain high over the course of the first month of abstinence are more likely to be younger and have co-occurring mental health or substance use disorders. From a stress and coping theory perspective, such individuals may be at higher risk for return to use and may require more comprehensive services to address independent anxiety/depression disorders.
For individuals and families seeking recovery: Many people experience anxiety or depression in the early days of a recovery journey. If you are experiencing this, these findings suggest that you are likely to experience some relief in the first 6 weeks while stopping alcohol use. However, if you have elevated symptoms, and also meet criteria for posttraumatic stress disorder or another substance use disorder, you may be less likely to see as large reductions, or at least as rapidly over the first few weeks of initial abstinence. People with this pattern may wish to consider additional treatment that can address these other challenges.
For treatment professionals and treatment systems: If you treat patients with alcohol use disorder who wish to cease alcohol use, significant anxiety or depressive symptoms may impede achievement of that goal during the initial recovery phases. It is important to asses for anxiety and depression in order to better understand the needs of the patient. Further, those with comorbidities such as co-occuring posttraumatic stress disorder or other substance use disorders may be more likely to have sustained symptoms of depression or anxiety during the initial treatment episode, which may require more additional treatment focused specifically on addressing these other challenges.
For scientists: These data suggest that there are distinct profiles of change in anxiety and depression over the first 6 weeks of initial abstinence in a treatment setting. Future research may consider examining associations between change profiles and substance use outcomes, or even substance use severity at the start of treatment. Further, although a substantive portion of people initiating recovery return to use in the first month, the risk remains elevated particularly across the first year. Future studies that examine trajectories over a full year may reveal alternative patterns of change that can further individualize treatment approaches. Finally, the data from this study are unable to reveal the mechanisms underlying these profiles. Future research may attempt to uncover why people fall into each of the anxiety and depression subgroups.
For policy makers: These data highlight the significant barriers people with alcohol use disorder face as they attempt to make changes to their alcohol use. Policies that increase access to treatment or recovery support services is likely to alleviate symptoms and increase remission success. Further, funding for research in the intersection between anxiety and depression and alcohol use disorder may provide more targeted approaches for managing these commonly co-occurring conditions.