
PTSD & addiction: an integrated treatment approach
Co-occurring substance use disorder (SUD) and post-traumatic stress disorder (PTSD) can be difficult to treat as patients in standard SUD treatment tend to experience poorer outcomes. Novel approaches tailored to this comorbidity are needed to give patients the best prognosis.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
This randomized controlled trial (RCT) evaluated the efficacy of integrated cognitive-behavioral therapy (ICBT) for co-occurring substance use and PTSD in a real-world outpatient clinical setting. This RCT builds on a feasibility trial (n = 11) and a pilot trial (n = 53) conducted in well controlled settings. This larger RCT determining the effectiveness of ICBT in a real world setting will increase the broader applicability of this treatment.
HOW WAS THIS STUDY CONDUCTED?
The current study (N = 221) compared three different treatment conditions: 1. standard care (SC) alone; 2. standard care (SC) plus integrated cognitive-behavioral therapy (ICBT); and 3. standard care (SC) plus individual addiction counseling (IAC). ICBT is a manualized therapy that includes patient education, mindful relaxation (techniques to handle negative affect and cravings), and flexible thinking (cognitive restructuring that focuses on the interplay between cognitions, emotions, and behaviors). Individual addiction counseling (IAC) is a manualized therapy that focuses solely on substance use recovery and combines individual drug counseling and twelve-step facilitation, two evidence-based treatments tested in prior large-scale randomized trials.
Both integrated cognitive-behavioral therapy (ICBT) and IAC consisted of 45 minute individual sessions delivered weekly for 8-12 weeks. SC refers to intensive outpatient services for 9-12 hours per week including 2-4 days of group and individual therapy sessions. SC is delivered over the course of 6-8 weeks followed by 12 weeks of once-weekly continuing care group sessions. Patients meeting diagnostic criteria for both PTSD and substance use disorder (SUD) were randomized to ICBT + SC (n = 73), IAC + SC (n = 75), SC only (n = 73). The groups will hereafter be referred to as ICBT, IAC, and SC, respectively.
The study planned for assessments at baseline, 3-months, and 6-months, with 3-months acting as the end of treatment assessment and 6-months serving as a follow-up assessment. However, about 80% of participants did not complete ICBT or IAC by 3 months requiring the authors to use the 6-month assessment as the measure of post-treatment effects. At 6 months, follow-up rates were 80%, 81%, and 73% for ICBT, IAC, and SC, respectively.
WHAT DID THIS STUDY FIND?
When comparing integrated cognitive-behavioral therapy (ICBT) to individual addiction counseling (IAC) at the two time points, the differences in toxicology results were significantly different by group. For ICBT versus standard care (SC), groups differed significantly for both toxicology and self-reported drug use as ICBT patients experienced greater reductions in days of drug use. Additionally, ICBT patients had significantly better therapy attendance than IAC patients.
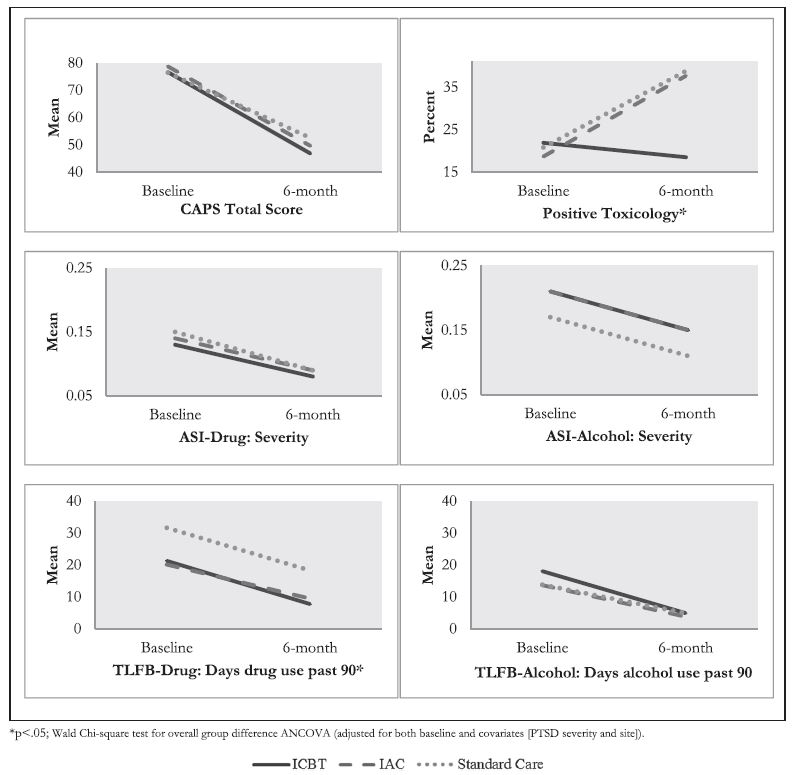
Surprisingly, ICBT, the intervention including PTSD-focused CBT which is consistently shown to be an effective therapy for PTSD (see here for a meta-analysis), did not improve PTSD severity in comparison to the substance use disorder (SUD)-only focused treatments, IAC and standard care (SC) .
This finding is inconsistent with the smaller trials of integrated cognitive-behavioral therapy (ICBT) and may decrease confidence in ICBT as an integrated therapy for PTSD and substance use disorder (SUD). While the proposed theory behind this intervention was not supported, it may still be a viable treatment option for those seeking recovery as ICBT reported greater reductions in drug use (past 90 days) compared to SC, and toxicology results were greater for ICBT than both of the other conditions. Longer follow-up is needed to substantiate these findings. Additionally, the mechanism by which it may do this is unclear.

While integrated cognitive-behavioral therapy (ICBT)had no advantage over individual addiction counseling (IAC) or SC for PTSD symptom severity, it is important to keep in mind the advantage for substance use disorder (SUD) outcomes compared to the other two interventions as ICBT yielded a medium effect size when comparing toxicology results from ICBT to both IAC and SC. The most clinically relevant aspect of this study is that ICBT has the potential for widespread implementation due to ease of adherence to the protocol by therapists.
ICBT also had the highest levels of therapy attendance by patients. Since it is not possible to blind behavioral therapies in the same manner as medication trials, participants are aware of the therapy they are receiving. One possibility is that patients not randomized to receive the integrated PTSD treatment may be disappointed with their treatment assignment and therefore are less motivated to continue attending sessions.
WHY IS THIS STUDY IMPORTANT?
PTSD and substance use disorder (SUD) are strongly linked. The prevalence of PTSD is three times higher among SUD patients than the general population ranging from 25% to 49% (see here). Since PTSD is characterized by the experience of stress and anxiety, individuals are at higher risk to use alcohol or other drugs to cope. Furthermore, treatment outcomes are poorer for patients with co-occurring PTSD, warranting the need for an integrated approach.
Since the safety, acceptability, feasibility and benefit of integrated cognitive-behavioral therapy (ICBT) on PTSD and substance use outcomes has been previously demonstrated, a larger stage III trial, such as the one conducted here, was needed to confirm effectiveness by comparing it to the current available treatments—individual addiction counseling (IAC) and standard care (SC)—in a real world clinical setting.
- LIMITATIONS
-
- This study planned on collecting data on participants at 3 months (proposed end of treatment) and 6 months (post-treatment follow-up). Since the treatment took longer than anticipated with a majority of patients still in active treatment by month 3, 6 month data was used for both purposes, resulting in lack of adequate follow-up data.
NEXT STEPS
Since individual addiction counseling (IAC) and standard care (SC) focused solely on substance use disorder (SUD) treatment, it was hypothesized that integrated cognitive-behavioral therapy (ICBT) would result in superior PTSD outcomes and there would be no difference in SUD outcomes. Surprisingly, results were the opposite. Future studies into the mechanisms behind this finding are needed to improve ICBT or inform development of new integrated treatment approaches.
Outcomes should also be evaluated in the context of ongoing continuing care and implementation of this treatment over longer periods (e.g., using monthly booster sessions/check-ups) as these conditions are susceptible to relapse.
Lastly, comparative effectiveness trials with other therapies for co-occurring PTSD and SUD (e.g., Seeking Safety) are needed.
BOTTOM LINE
- For individuals & families seeking recovery: While all three interventions reduced PTSD symptom severity, integrated cognitive-behavioral therapy (ICBT)resulted in better substance use disorder (SUD) outcomes than both IAC and SC and may be a better treatment option if you are experiencing these co-occurring disorders.
- For scientists: Results of this study were different than previous smaller trials. More research is needed into the mechanisms of how ICBT works and why these difference occurred.
- For policy makers: Co-occurring disorders are common in patients with SUDs. Continued funding for research investigating approaches to enhance treatment response for PTSD symptoms in the context of SUD is warranted.
- For treatment professionals and treatment systems: ICBT is a potential treatment option for patients with co-occurring PTSD and SUD as it performed better than IAC and SC in regards to SUD outcomes and therapy attendance. It also appears to be feasible and adoptable in real world clinical settings.
CITATIONS
McGovern, M. P., Lambert-Harris, C., Xie, H., Meier, A., McLeman, B., & Saunders, E. (2015). A randomized controlled trial of treatments for co-occurring substance use disorders and post-traumatic stress disorder. Addiction, 110(7), 1194-1204. doi: 10.1111/add.12943
