The addiction field has continued to struggle to produce a testable operational definition of addiction “recovery” that can be used to estimate objective recovery rates that are distinct from rates of diagnostic remission alone or that can be used in social and legal decision making (e.g., child custody). The National Institute on Alcohol Abuse and Alcoholism (NIAAA) recently published a testable operational definition. This study was the first to examine its clinical and public health utility.
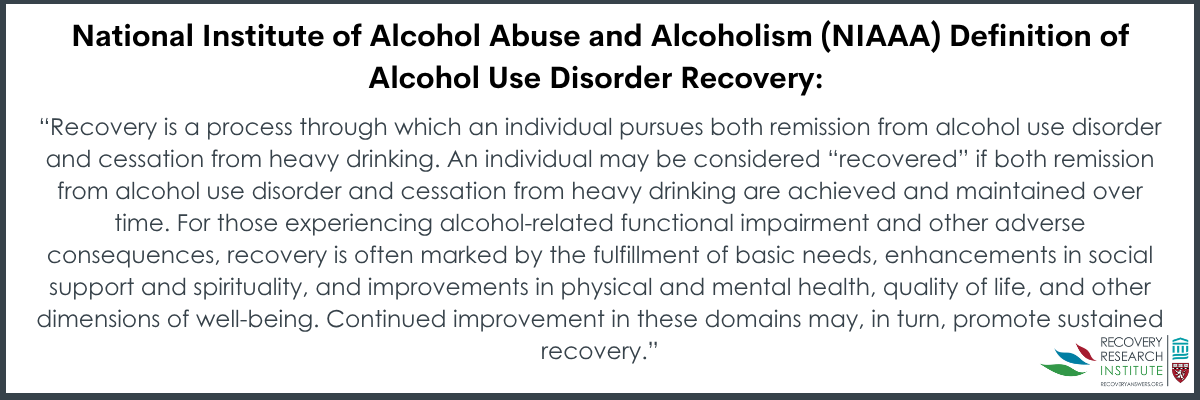
Many definitions of recovery have been suggested, but consensus has remained difficult to achieve given its multifaceted nature. Also, the field has struggled to come up with specific criteria so that objective prevalence rates can be obtained beyond self-defined subjective estimates of “recovery” or rates of diagnostic remission alone. In 2022, a workgroup at the National Institute of Alcohol Abuse and Alcoholism (best known by its acronym, NIAAA) developed an operational definition that includes both cessation from heavy drinking (defined as a maximum of 3 drinks per day and 7 per week for females, or 4 per day and 14 per week for males) and the absence of alcohol use disorder symptoms (with the exception of cravings), called “remission”. Their definition is as follows:
While this definition has begun to be adopted, it continues to be debated. Questions remain about its utility. including what clinical factors predict meeting this particular definition of recovery how stable it remains over time, how it compares to other forms of alcohol use disorder resolution, and the psychosocial benefits related to these different operational definitions of “recovery”.
This study assessed the prevalence of NIAAA-defined recovery, and individual factors associated with achieving it, while comparing it with alternative outcomes like alcohol use disorder remission with continued heavy drinking. It also examined the benefits of these different types of recovery designations.
HOW WAS THIS STUDY CONDUCTED?
This was a longitudinal, observational study of 442 participants in the first year of a current alcohol use disorder recovery attempt who were assessed each quarter over a year – at baseline as well as 3-month, 6-month, and 12-month follow-ups.
Participants were enrolled at two North American sites—Hamilton, Ontario (Canada) and Boston, Massachusetts (USA). Eligibility criteria included being 21 to 65 years old, having alcohol as one’s primary substance, and having a current Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) diagnosis of alcohol use disorder with high-risk drinking in the 30 days before starting the recovery attempt (i.e., greater than 7 drinks/week for females, and greater than 14/week for males). Additionally, participants must have initiated a formal treatment or informal (i.e., unassisted) recovery attempt in the past 90 days before enrollment, or had a plan to begin within 14 days.
At each assessment the researchers measured: 1) Alcohol use (frequency and intensity) and alcohol use disorder symptoms, 2) alcohol-related consequences, 3) alcohol and other drug self-efficacy, 4) recovery capital, 5) commitment to sobriety, 6) mental health status, 7) depression, 8) quality of life, 9) well-being, 10) happiness, and 11) self-esteem.
The team classified participants into four groups based on remission status and drinking pattern at each follow-up: 1) Remission with abstinence, 2) remission with low-risk drinking (with groups 1 and 2 meeting NIAAA’s ‘recovery’ definition), 3) remission with higher-risk drinking, and 4) no remission. They tracked transitions among these groups over the 1-year study period.
Around 60% of participants were female, the majority were White (80%), and most identified as heterosexual (77%). Slightly more than half had less than a bachelor’s degree, and about 45% reported not having enough income to meet their needs comfortably. At baseline, the mean alcohol use disorder severity level was severe (6+ symptoms out of 11), and most participants reported drinking heavily on most days in the 3-month period before initiating their new alcohol use disorder recovery attempt and enrolling in the study.
WHAT DID THIS STUDY FIND?
A third of participants achieved NIAAA-defined recovery
Approximately 35% of participants achieved NIAAA-defined recovery at some point during the year following their initiation of a recovery attempt (i.e., remission plus abstinence or low-risk drinking). Of those achieving NIAAA-defined recovery, about two-thirds (67%) were completely abstinent (i.e., no drinking whatsoever) while one-third achieved remission but reported some low-level alcohol use. Of those not demonstrating NIAAA-defined recovery, 16% achieved alcohol use disorder remission but continued drinking at high risk levels, while half (50%) never achieved remission during the 1-year study period.
Participants with NIAAA-defined recovery had the greatest recovery stability over time
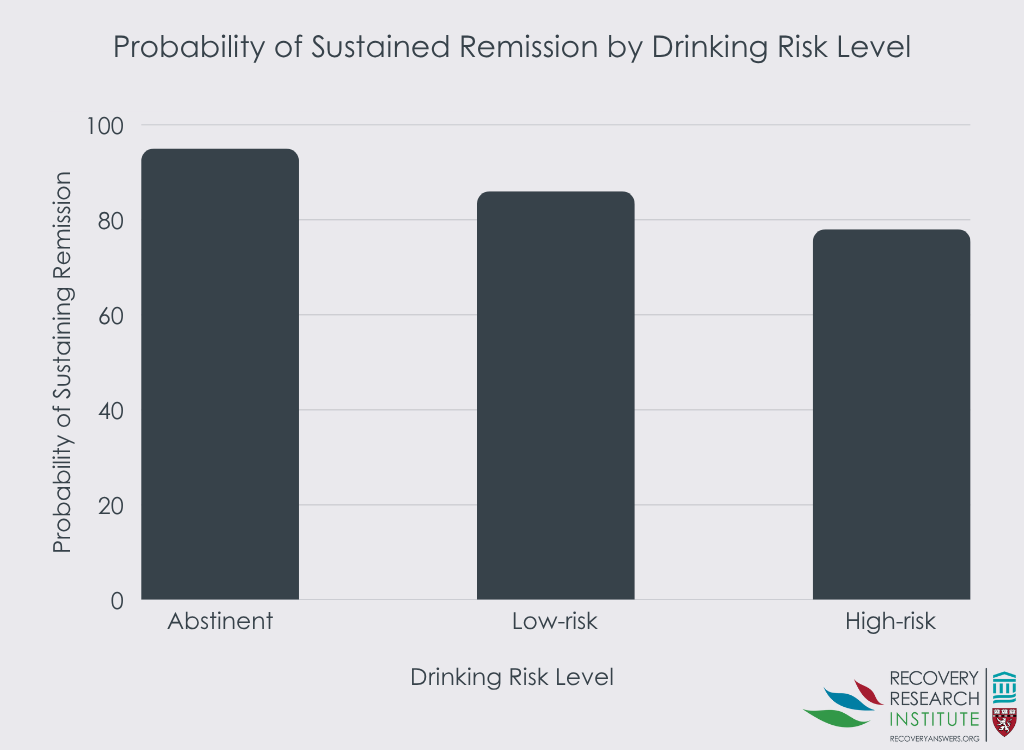
There were notable differences in drinking and alcohol-related problem stability across recovery groups. The abstinent remission group showed the greatest stability (95% probability of remaining in remission), followed by the remission with low-risk drinking group (86% probability), and the higher-risk drinking remission group (78% probability) – see graph below. Over time, both drinking remission groups showed a tendency toward greater alcohol use and alcohol use disorder relapse, with the higher-risk drinking group being particularly unstable in the final quarter of follow-up and 20% of these participants moving to the non-remission group.
Those achieving abstinent recovery were more likely to start with greater problem severity
There were distinct baseline profiles among recovery groups. The abstinent remission group, despite achieving the most stable recovery, actually exhibited more severe clinical characteristics at baseline—similar to the non-remission group—including higher alcohol use disorder symptom counts, more drinks per drinking day, greater alcohol-related consequences, and higher likelihood of prior treatment. In contrast, both drinking remission groups (i.e., low-risk and higher-risk) showed less severe baseline profiles with fewer alcohol use disorder symptoms, lower drinking intensity, fewer consequences and lower likelihood of prior treatment. Key predictors of achieving NIAAA-defined recovery included having sufficient household income, greater commitment to sobriety, greater abstinence self-efficacy, and lower baseline alcohol use disorder severity indicators.
Those achieving NIAAA-defined recovery showed the greatest improvements in psychological well-being and quality of life
Those achieving NIAAA-defined recovery (both abstinent and remitted but low-risk drinking groups) experienced substantial improvements in psychological well-being and quality of life between baseline and the last follow-up at which they experienced remission compared to participants who did not achieve remission or who maintained remission but engaged in heavier drinking. For all 3 remission groups, effect sizes for improvements were often moderate to large across domains including anxiety, depression, and quality of life. However, a notable exception was found in measures of happiness and self-esteem, where the higher-risk drinking remission group showed little improvement, similar to the non-remission group. With regards to recovery capital (the resources necessary to begin and maintain recovery from substance use disorder), all the remission groups showed improvements, while the non-remission group did not. With the exception of depression, the non-remission group did not see improvements in psychosocial and well-being outcomes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The NIAAA operational definition of recovery examined in this study appears to capture meaningful improvements in well-being and functioning, not just remission of alcohol use disorder symptoms. The researchers’ findings suggest this definition has practical utility and that achieving either abstinence or low-risk drinking while in remission leads to substantial psychosocial benefits, and that abstinent remission is the most stable form of recovery.
The researchers also identified some important differences between subgroups. Their results suggest that people who achieve remission with either abstinence or with low-risk drinking may represent different alcohol use disorder subtypes or stages of change. Specifically, those achieving abstinent remission tended to have more severe baseline characteristics, while low-risk drinkers showed less initial baseline severity and struggled to maintain remission over time. This is consistent with previous studies that have shown that abstainers are more likely to remain in remission than low-risk drinkers.
Achieving NIAAA-defined recovery (either with abstinence or low-risk drinking) was also associated with a greater improvement in psychosocial well-being and quality of life. This finding is consistent with previous research showing people who have resolved an alcohol or other drug problem tend to show the most gains in recovery when they are abstinent or drinking/using substances at lower-risk levels.
Conversely, continuing to drink at high-risk thresholds, even while maintaining diagnostic remission, appears to pose a significant risk for both psychological well-being and recovery stability. The researchers’ findings indicate that heavier drinking during remission is associated with less improvement in happiness and self-esteem and may produce a greater “gravitational tendency” toward full alcohol use disorder recurrence. As study authors note, for many in this group, alcohol exposure at higher levels may perpetuate cravings and alcohol use over time, in turn destabilizing remission.
The findings highlight the importance of addressing both symptom remission and alcohol use patterns in treatment planning. And while achieving any form of remission brings substantial benefits, the greater stability of abstinent remission suggests that abstinence may be the optimal long-term goal for many individuals with severe alcohol use disorder histories. At the same time, the study also validates that some individuals can benefit from achieving remission while maintaining high-risk drinking patterns, at least in the short term, though to a lesser degree than those with low-risk or no alcohol use. The challenge for the remitted but drinking groups is how to prevent deterioration and susceptibility toward increased symptomatic use and related consequences that also appear to diminish quality of life and functioning.
The sample was primarily White, and findings may not generalize to other populations or geographic regions outside culturally similar urban areas in Canada and the United States.
Bioassay confirmation, originally planned for the study design, became infeasible due to COVID-19 restrictions and a move to remote assessments. Data relied entirely on participant self-report rather than biochemical confirmation of abstinence or alcohol use levels. Though self-report is a valid way to assess substance use, confirmation with bioassays increases confidence.
The statistical ability to detect effect was low in some of the researchers’ analyses due to relatively small sample sizes in certain groups, warranting confirmation in larger samples.
BOTTOM LINE
The NIAAA’s operational definition of ‘recovery’ (remission plus no heavy drinking) appears to be clinically meaningful, and attainable for a significant subset of people making new recovery attempts and is associated with real improvements in quality of life and well-being. Those who achieved remission but continued heavy drinking fared better than those who didn’t remit, but on the whole they did more poorly that those who remitted with abstinence or low-risk drinking. Those in abstinent remission had the most stable form of recovery compared to those in remission but drinking at low- or high-risk levels.
For individuals and families seeking recovery: Achieving remission from alcohol use disorder—whether with full abstinence or with low-risk drinking—can bring substantial improvements in quality of life and well-being. Heavier drinking during remission may reduce these benefits and increase the risk of alcohol use disorder relapse. Continued alcohol use when in remission may destabilize and reduce gains in quality of life and functioning over time as there is tendency to gravitate toward symptomatic use.
For treatment professionals and treatment systems: Clear and measurable definitions of recovery help in creating objective estimates of recovery prevalence and in tracking progress and predicting long-term outcomes. Supporting clients to achieve and maintain abstinence or low-risk drinking, and regularly monitoring symptoms and functioning, will likely improve recovery stability.
For scientists: The NIAAA’s operational definition of recovery appears to be useful for research and clinical benchmarking. However, future studies should explore these patterns in more diverse and representative samples and continue to refine the understanding of recovery trajectories.
For policy makers: Standardized, objective, definitions of recovery can help inform policy, funding, and program design, including by producing the ability to provide objective prevalence rates of “recovery” that are distinct from diagnostic remission alone. The NIAAA definition links clinical improvement to measurable public health impact beyond just remission.
Many definitions of recovery have been suggested, but consensus has remained difficult to achieve given its multifaceted nature. Also, the field has struggled to come up with specific criteria so that objective prevalence rates can be obtained beyond self-defined subjective estimates of “recovery” or rates of diagnostic remission alone. In 2022, a workgroup at the National Institute of Alcohol Abuse and Alcoholism (best known by its acronym, NIAAA) developed an operational definition that includes both cessation from heavy drinking (defined as a maximum of 3 drinks per day and 7 per week for females, or 4 per day and 14 per week for males) and the absence of alcohol use disorder symptoms (with the exception of cravings), called “remission”. Their definition is as follows:
While this definition has begun to be adopted, it continues to be debated. Questions remain about its utility. including what clinical factors predict meeting this particular definition of recovery how stable it remains over time, how it compares to other forms of alcohol use disorder resolution, and the psychosocial benefits related to these different operational definitions of “recovery”.
This study assessed the prevalence of NIAAA-defined recovery, and individual factors associated with achieving it, while comparing it with alternative outcomes like alcohol use disorder remission with continued heavy drinking. It also examined the benefits of these different types of recovery designations.
HOW WAS THIS STUDY CONDUCTED?
This was a longitudinal, observational study of 442 participants in the first year of a current alcohol use disorder recovery attempt who were assessed each quarter over a year – at baseline as well as 3-month, 6-month, and 12-month follow-ups.
Participants were enrolled at two North American sites—Hamilton, Ontario (Canada) and Boston, Massachusetts (USA). Eligibility criteria included being 21 to 65 years old, having alcohol as one’s primary substance, and having a current Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) diagnosis of alcohol use disorder with high-risk drinking in the 30 days before starting the recovery attempt (i.e., greater than 7 drinks/week for females, and greater than 14/week for males). Additionally, participants must have initiated a formal treatment or informal (i.e., unassisted) recovery attempt in the past 90 days before enrollment, or had a plan to begin within 14 days.
At each assessment the researchers measured: 1) Alcohol use (frequency and intensity) and alcohol use disorder symptoms, 2) alcohol-related consequences, 3) alcohol and other drug self-efficacy, 4) recovery capital, 5) commitment to sobriety, 6) mental health status, 7) depression, 8) quality of life, 9) well-being, 10) happiness, and 11) self-esteem.
The team classified participants into four groups based on remission status and drinking pattern at each follow-up: 1) Remission with abstinence, 2) remission with low-risk drinking (with groups 1 and 2 meeting NIAAA’s ‘recovery’ definition), 3) remission with higher-risk drinking, and 4) no remission. They tracked transitions among these groups over the 1-year study period.
Around 60% of participants were female, the majority were White (80%), and most identified as heterosexual (77%). Slightly more than half had less than a bachelor’s degree, and about 45% reported not having enough income to meet their needs comfortably. At baseline, the mean alcohol use disorder severity level was severe (6+ symptoms out of 11), and most participants reported drinking heavily on most days in the 3-month period before initiating their new alcohol use disorder recovery attempt and enrolling in the study.
WHAT DID THIS STUDY FIND?
A third of participants achieved NIAAA-defined recovery
Approximately 35% of participants achieved NIAAA-defined recovery at some point during the year following their initiation of a recovery attempt (i.e., remission plus abstinence or low-risk drinking). Of those achieving NIAAA-defined recovery, about two-thirds (67%) were completely abstinent (i.e., no drinking whatsoever) while one-third achieved remission but reported some low-level alcohol use. Of those not demonstrating NIAAA-defined recovery, 16% achieved alcohol use disorder remission but continued drinking at high risk levels, while half (50%) never achieved remission during the 1-year study period.
Participants with NIAAA-defined recovery had the greatest recovery stability over time
There were notable differences in drinking and alcohol-related problem stability across recovery groups. The abstinent remission group showed the greatest stability (95% probability of remaining in remission), followed by the remission with low-risk drinking group (86% probability), and the higher-risk drinking remission group (78% probability) – see graph below. Over time, both drinking remission groups showed a tendency toward greater alcohol use and alcohol use disorder relapse, with the higher-risk drinking group being particularly unstable in the final quarter of follow-up and 20% of these participants moving to the non-remission group.
Those achieving abstinent recovery were more likely to start with greater problem severity
There were distinct baseline profiles among recovery groups. The abstinent remission group, despite achieving the most stable recovery, actually exhibited more severe clinical characteristics at baseline—similar to the non-remission group—including higher alcohol use disorder symptom counts, more drinks per drinking day, greater alcohol-related consequences, and higher likelihood of prior treatment. In contrast, both drinking remission groups (i.e., low-risk and higher-risk) showed less severe baseline profiles with fewer alcohol use disorder symptoms, lower drinking intensity, fewer consequences and lower likelihood of prior treatment. Key predictors of achieving NIAAA-defined recovery included having sufficient household income, greater commitment to sobriety, greater abstinence self-efficacy, and lower baseline alcohol use disorder severity indicators.
Those achieving NIAAA-defined recovery showed the greatest improvements in psychological well-being and quality of life
Those achieving NIAAA-defined recovery (both abstinent and remitted but low-risk drinking groups) experienced substantial improvements in psychological well-being and quality of life between baseline and the last follow-up at which they experienced remission compared to participants who did not achieve remission or who maintained remission but engaged in heavier drinking. For all 3 remission groups, effect sizes for improvements were often moderate to large across domains including anxiety, depression, and quality of life. However, a notable exception was found in measures of happiness and self-esteem, where the higher-risk drinking remission group showed little improvement, similar to the non-remission group. With regards to recovery capital (the resources necessary to begin and maintain recovery from substance use disorder), all the remission groups showed improvements, while the non-remission group did not. With the exception of depression, the non-remission group did not see improvements in psychosocial and well-being outcomes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The NIAAA operational definition of recovery examined in this study appears to capture meaningful improvements in well-being and functioning, not just remission of alcohol use disorder symptoms. The researchers’ findings suggest this definition has practical utility and that achieving either abstinence or low-risk drinking while in remission leads to substantial psychosocial benefits, and that abstinent remission is the most stable form of recovery.
The researchers also identified some important differences between subgroups. Their results suggest that people who achieve remission with either abstinence or with low-risk drinking may represent different alcohol use disorder subtypes or stages of change. Specifically, those achieving abstinent remission tended to have more severe baseline characteristics, while low-risk drinkers showed less initial baseline severity and struggled to maintain remission over time. This is consistent with previous studies that have shown that abstainers are more likely to remain in remission than low-risk drinkers.
Achieving NIAAA-defined recovery (either with abstinence or low-risk drinking) was also associated with a greater improvement in psychosocial well-being and quality of life. This finding is consistent with previous research showing people who have resolved an alcohol or other drug problem tend to show the most gains in recovery when they are abstinent or drinking/using substances at lower-risk levels.
Conversely, continuing to drink at high-risk thresholds, even while maintaining diagnostic remission, appears to pose a significant risk for both psychological well-being and recovery stability. The researchers’ findings indicate that heavier drinking during remission is associated with less improvement in happiness and self-esteem and may produce a greater “gravitational tendency” toward full alcohol use disorder recurrence. As study authors note, for many in this group, alcohol exposure at higher levels may perpetuate cravings and alcohol use over time, in turn destabilizing remission.
The findings highlight the importance of addressing both symptom remission and alcohol use patterns in treatment planning. And while achieving any form of remission brings substantial benefits, the greater stability of abstinent remission suggests that abstinence may be the optimal long-term goal for many individuals with severe alcohol use disorder histories. At the same time, the study also validates that some individuals can benefit from achieving remission while maintaining high-risk drinking patterns, at least in the short term, though to a lesser degree than those with low-risk or no alcohol use. The challenge for the remitted but drinking groups is how to prevent deterioration and susceptibility toward increased symptomatic use and related consequences that also appear to diminish quality of life and functioning.
The sample was primarily White, and findings may not generalize to other populations or geographic regions outside culturally similar urban areas in Canada and the United States.
Bioassay confirmation, originally planned for the study design, became infeasible due to COVID-19 restrictions and a move to remote assessments. Data relied entirely on participant self-report rather than biochemical confirmation of abstinence or alcohol use levels. Though self-report is a valid way to assess substance use, confirmation with bioassays increases confidence.
The statistical ability to detect effect was low in some of the researchers’ analyses due to relatively small sample sizes in certain groups, warranting confirmation in larger samples.
BOTTOM LINE
The NIAAA’s operational definition of ‘recovery’ (remission plus no heavy drinking) appears to be clinically meaningful, and attainable for a significant subset of people making new recovery attempts and is associated with real improvements in quality of life and well-being. Those who achieved remission but continued heavy drinking fared better than those who didn’t remit, but on the whole they did more poorly that those who remitted with abstinence or low-risk drinking. Those in abstinent remission had the most stable form of recovery compared to those in remission but drinking at low- or high-risk levels.
For individuals and families seeking recovery: Achieving remission from alcohol use disorder—whether with full abstinence or with low-risk drinking—can bring substantial improvements in quality of life and well-being. Heavier drinking during remission may reduce these benefits and increase the risk of alcohol use disorder relapse. Continued alcohol use when in remission may destabilize and reduce gains in quality of life and functioning over time as there is tendency to gravitate toward symptomatic use.
For treatment professionals and treatment systems: Clear and measurable definitions of recovery help in creating objective estimates of recovery prevalence and in tracking progress and predicting long-term outcomes. Supporting clients to achieve and maintain abstinence or low-risk drinking, and regularly monitoring symptoms and functioning, will likely improve recovery stability.
For scientists: The NIAAA’s operational definition of recovery appears to be useful for research and clinical benchmarking. However, future studies should explore these patterns in more diverse and representative samples and continue to refine the understanding of recovery trajectories.
For policy makers: Standardized, objective, definitions of recovery can help inform policy, funding, and program design, including by producing the ability to provide objective prevalence rates of “recovery” that are distinct from diagnostic remission alone. The NIAAA definition links clinical improvement to measurable public health impact beyond just remission.
Many definitions of recovery have been suggested, but consensus has remained difficult to achieve given its multifaceted nature. Also, the field has struggled to come up with specific criteria so that objective prevalence rates can be obtained beyond self-defined subjective estimates of “recovery” or rates of diagnostic remission alone. In 2022, a workgroup at the National Institute of Alcohol Abuse and Alcoholism (best known by its acronym, NIAAA) developed an operational definition that includes both cessation from heavy drinking (defined as a maximum of 3 drinks per day and 7 per week for females, or 4 per day and 14 per week for males) and the absence of alcohol use disorder symptoms (with the exception of cravings), called “remission”. Their definition is as follows:
While this definition has begun to be adopted, it continues to be debated. Questions remain about its utility. including what clinical factors predict meeting this particular definition of recovery how stable it remains over time, how it compares to other forms of alcohol use disorder resolution, and the psychosocial benefits related to these different operational definitions of “recovery”.
This study assessed the prevalence of NIAAA-defined recovery, and individual factors associated with achieving it, while comparing it with alternative outcomes like alcohol use disorder remission with continued heavy drinking. It also examined the benefits of these different types of recovery designations.
HOW WAS THIS STUDY CONDUCTED?
This was a longitudinal, observational study of 442 participants in the first year of a current alcohol use disorder recovery attempt who were assessed each quarter over a year – at baseline as well as 3-month, 6-month, and 12-month follow-ups.
Participants were enrolled at two North American sites—Hamilton, Ontario (Canada) and Boston, Massachusetts (USA). Eligibility criteria included being 21 to 65 years old, having alcohol as one’s primary substance, and having a current Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) diagnosis of alcohol use disorder with high-risk drinking in the 30 days before starting the recovery attempt (i.e., greater than 7 drinks/week for females, and greater than 14/week for males). Additionally, participants must have initiated a formal treatment or informal (i.e., unassisted) recovery attempt in the past 90 days before enrollment, or had a plan to begin within 14 days.
At each assessment the researchers measured: 1) Alcohol use (frequency and intensity) and alcohol use disorder symptoms, 2) alcohol-related consequences, 3) alcohol and other drug self-efficacy, 4) recovery capital, 5) commitment to sobriety, 6) mental health status, 7) depression, 8) quality of life, 9) well-being, 10) happiness, and 11) self-esteem.
The team classified participants into four groups based on remission status and drinking pattern at each follow-up: 1) Remission with abstinence, 2) remission with low-risk drinking (with groups 1 and 2 meeting NIAAA’s ‘recovery’ definition), 3) remission with higher-risk drinking, and 4) no remission. They tracked transitions among these groups over the 1-year study period.
Around 60% of participants were female, the majority were White (80%), and most identified as heterosexual (77%). Slightly more than half had less than a bachelor’s degree, and about 45% reported not having enough income to meet their needs comfortably. At baseline, the mean alcohol use disorder severity level was severe (6+ symptoms out of 11), and most participants reported drinking heavily on most days in the 3-month period before initiating their new alcohol use disorder recovery attempt and enrolling in the study.
WHAT DID THIS STUDY FIND?
A third of participants achieved NIAAA-defined recovery
Approximately 35% of participants achieved NIAAA-defined recovery at some point during the year following their initiation of a recovery attempt (i.e., remission plus abstinence or low-risk drinking). Of those achieving NIAAA-defined recovery, about two-thirds (67%) were completely abstinent (i.e., no drinking whatsoever) while one-third achieved remission but reported some low-level alcohol use. Of those not demonstrating NIAAA-defined recovery, 16% achieved alcohol use disorder remission but continued drinking at high risk levels, while half (50%) never achieved remission during the 1-year study period.
Participants with NIAAA-defined recovery had the greatest recovery stability over time
There were notable differences in drinking and alcohol-related problem stability across recovery groups. The abstinent remission group showed the greatest stability (95% probability of remaining in remission), followed by the remission with low-risk drinking group (86% probability), and the higher-risk drinking remission group (78% probability) – see graph below. Over time, both drinking remission groups showed a tendency toward greater alcohol use and alcohol use disorder relapse, with the higher-risk drinking group being particularly unstable in the final quarter of follow-up and 20% of these participants moving to the non-remission group.
Those achieving abstinent recovery were more likely to start with greater problem severity
There were distinct baseline profiles among recovery groups. The abstinent remission group, despite achieving the most stable recovery, actually exhibited more severe clinical characteristics at baseline—similar to the non-remission group—including higher alcohol use disorder symptom counts, more drinks per drinking day, greater alcohol-related consequences, and higher likelihood of prior treatment. In contrast, both drinking remission groups (i.e., low-risk and higher-risk) showed less severe baseline profiles with fewer alcohol use disorder symptoms, lower drinking intensity, fewer consequences and lower likelihood of prior treatment. Key predictors of achieving NIAAA-defined recovery included having sufficient household income, greater commitment to sobriety, greater abstinence self-efficacy, and lower baseline alcohol use disorder severity indicators.
Those achieving NIAAA-defined recovery showed the greatest improvements in psychological well-being and quality of life
Those achieving NIAAA-defined recovery (both abstinent and remitted but low-risk drinking groups) experienced substantial improvements in psychological well-being and quality of life between baseline and the last follow-up at which they experienced remission compared to participants who did not achieve remission or who maintained remission but engaged in heavier drinking. For all 3 remission groups, effect sizes for improvements were often moderate to large across domains including anxiety, depression, and quality of life. However, a notable exception was found in measures of happiness and self-esteem, where the higher-risk drinking remission group showed little improvement, similar to the non-remission group. With regards to recovery capital (the resources necessary to begin and maintain recovery from substance use disorder), all the remission groups showed improvements, while the non-remission group did not. With the exception of depression, the non-remission group did not see improvements in psychosocial and well-being outcomes.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The NIAAA operational definition of recovery examined in this study appears to capture meaningful improvements in well-being and functioning, not just remission of alcohol use disorder symptoms. The researchers’ findings suggest this definition has practical utility and that achieving either abstinence or low-risk drinking while in remission leads to substantial psychosocial benefits, and that abstinent remission is the most stable form of recovery.
The researchers also identified some important differences between subgroups. Their results suggest that people who achieve remission with either abstinence or with low-risk drinking may represent different alcohol use disorder subtypes or stages of change. Specifically, those achieving abstinent remission tended to have more severe baseline characteristics, while low-risk drinkers showed less initial baseline severity and struggled to maintain remission over time. This is consistent with previous studies that have shown that abstainers are more likely to remain in remission than low-risk drinkers.
Achieving NIAAA-defined recovery (either with abstinence or low-risk drinking) was also associated with a greater improvement in psychosocial well-being and quality of life. This finding is consistent with previous research showing people who have resolved an alcohol or other drug problem tend to show the most gains in recovery when they are abstinent or drinking/using substances at lower-risk levels.
Conversely, continuing to drink at high-risk thresholds, even while maintaining diagnostic remission, appears to pose a significant risk for both psychological well-being and recovery stability. The researchers’ findings indicate that heavier drinking during remission is associated with less improvement in happiness and self-esteem and may produce a greater “gravitational tendency” toward full alcohol use disorder recurrence. As study authors note, for many in this group, alcohol exposure at higher levels may perpetuate cravings and alcohol use over time, in turn destabilizing remission.
The findings highlight the importance of addressing both symptom remission and alcohol use patterns in treatment planning. And while achieving any form of remission brings substantial benefits, the greater stability of abstinent remission suggests that abstinence may be the optimal long-term goal for many individuals with severe alcohol use disorder histories. At the same time, the study also validates that some individuals can benefit from achieving remission while maintaining high-risk drinking patterns, at least in the short term, though to a lesser degree than those with low-risk or no alcohol use. The challenge for the remitted but drinking groups is how to prevent deterioration and susceptibility toward increased symptomatic use and related consequences that also appear to diminish quality of life and functioning.
The sample was primarily White, and findings may not generalize to other populations or geographic regions outside culturally similar urban areas in Canada and the United States.
Bioassay confirmation, originally planned for the study design, became infeasible due to COVID-19 restrictions and a move to remote assessments. Data relied entirely on participant self-report rather than biochemical confirmation of abstinence or alcohol use levels. Though self-report is a valid way to assess substance use, confirmation with bioassays increases confidence.
The statistical ability to detect effect was low in some of the researchers’ analyses due to relatively small sample sizes in certain groups, warranting confirmation in larger samples.
BOTTOM LINE
The NIAAA’s operational definition of ‘recovery’ (remission plus no heavy drinking) appears to be clinically meaningful, and attainable for a significant subset of people making new recovery attempts and is associated with real improvements in quality of life and well-being. Those who achieved remission but continued heavy drinking fared better than those who didn’t remit, but on the whole they did more poorly that those who remitted with abstinence or low-risk drinking. Those in abstinent remission had the most stable form of recovery compared to those in remission but drinking at low- or high-risk levels.
For individuals and families seeking recovery: Achieving remission from alcohol use disorder—whether with full abstinence or with low-risk drinking—can bring substantial improvements in quality of life and well-being. Heavier drinking during remission may reduce these benefits and increase the risk of alcohol use disorder relapse. Continued alcohol use when in remission may destabilize and reduce gains in quality of life and functioning over time as there is tendency to gravitate toward symptomatic use.
For treatment professionals and treatment systems: Clear and measurable definitions of recovery help in creating objective estimates of recovery prevalence and in tracking progress and predicting long-term outcomes. Supporting clients to achieve and maintain abstinence or low-risk drinking, and regularly monitoring symptoms and functioning, will likely improve recovery stability.
For scientists: The NIAAA’s operational definition of recovery appears to be useful for research and clinical benchmarking. However, future studies should explore these patterns in more diverse and representative samples and continue to refine the understanding of recovery trajectories.
For policy makers: Standardized, objective, definitions of recovery can help inform policy, funding, and program design, including by producing the ability to provide objective prevalence rates of “recovery” that are distinct from diagnostic remission alone. The NIAAA definition links clinical improvement to measurable public health impact beyond just remission.