
Characteristics of Swedish Workers Receiving Opioid Medications
Since unemployment is common among individuals who use substances, employment status is seen as a marker of stability among people in recovery.th.
For individuals with an opiate use disorder on medication assisted treatments (MAT), rejoining the workforce or maintaining current employment represents a return to normal social functioning and is seen as an important goal to work towards.
Nilsson and colleagues used data from the national Swedish Social Services register to examine the association between various factors and working while on medication assisted treatments (MAT)(prescribed by a physician) for a year or more. The data was collected between 2002 and 2008 and includes information on 2638 people residing in Sweden who used heroin or other opiates for three or more days per week for at least one year. A comparison of this dataset to Swedish Census data showed that the data is mainly representative of the Swedish population with slight over-representation of urban populations.
Using the Andersen model of health service utilization as a theoretical framework, the authors grouped participant factors into the following categories: predisposing factors (demographic and individual characteristics, e.g. age and gender), enabling factors (social resources that facilitate or impede the likelihood of a patient using health care services, e.g. work history and housing status), and need factors (characteristics influencing a patient’s perception of need for care, e.g. treatment history and criminal activity).
Over 70% of participants were male, and the average age was 34 years. Ten percent of participants reported currently working. The average number of years worked was 1.9. Regarding work history over the past three years, 40% were unemployed, 27% worked full time, and 9% worked part time. The average number of years taking prescribed methadone and buprenorphine was 2.5 and 1.7, respectively. About 6% reported working for more than a year while on MAT.
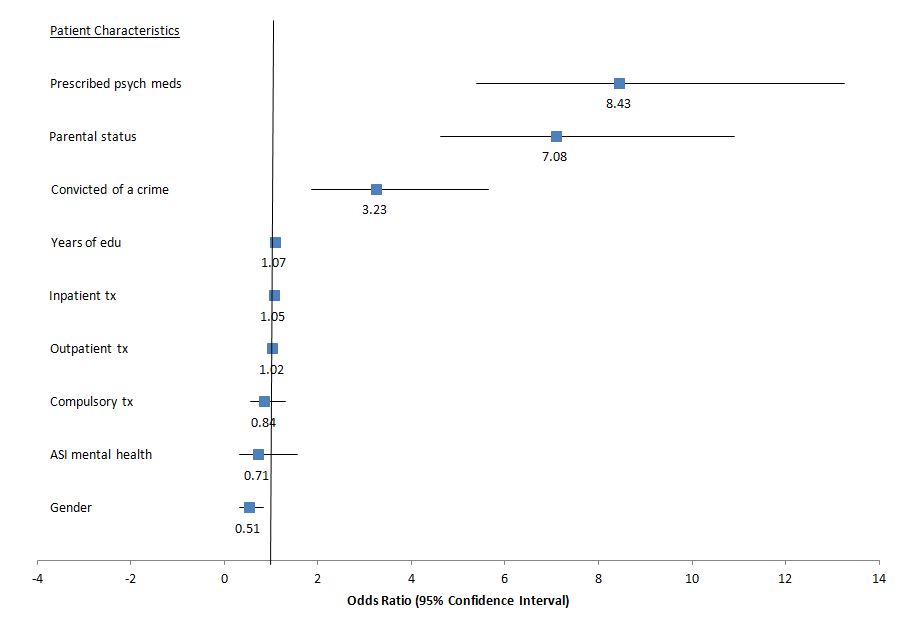
In the bivariate analysis of the predisposing factors, males, people with more years of education, and people with children were more likely to be working while on MAT compared to those who were not working or were not on MAT. No enabling factors were significantly associated with the outcome.
Of the need factors, previous outpatient treatment attendance and previous inpatient treatment attendance were significantly associated with working while on MAT, while those in compulsory treatment were significantly less likely to be working while on MAT (vs. not working or not on MAT). Participants who had ever been prescribed psychiatric medications, those with less severe mental health issues, and those with a criminal record were more likely to be working while on MAT
The authors then used logistic regression to examine the association between the outcome and the significant variables from the bivariate analysis.
IN CONTEXT
Examining factors related to working & recieving medication assisted treatment (MAT) provides insight into the characteristics of a patient that might make them a good candidate for this method of treatment.
Two of the more interesting findings from this study are that patients with children and patients prescribed psychiatric medication had the greatest likelihoods of working while on MAT. Those who take psychiatric medications may be generally more willing to take medication for behavioral or emotional difficulties, and thus are accepting of medication-based treatments for opioid use disorder. Children, and their need for a supportive, stable environment, may act as a motivator for parents to comply with MAT treatment regimens and to return to the workforce.
- LIMITATIONS
-
- Since data were derived from a national registry, important clinical variables such as readiness and motivation to change were not available. The observed relationship between the factors in this study and the outcome of working while on medication assisted treatment (MAT) may actually be explained by these variables or other unmeasured factors.
- In the analysis, the choice of comparison group made results difficult to interpret. Rather than comparing those working while on medication assisted treatment (MAT) to people who are either not working or working but not on MAT (defined as one group), a comparison should be made to those who are not working while on MAT. This would provide clearer insight into what factors influence the ability to work while on these medications.
- to work while on these medications.In order to start maintenance treatment in Sweden between 2002 and 2008, patients had to be 20 or older, have a history of trying and failing non-medication treatment, have at least four years of registered intravenous opiate misuse, and show proof of no polydrug use. Since participation in this study, the eligibility criteria for maintenance treatment has become less stringent, requiring patients to be 20 or older, have two years of documented opiate addiction, and have the capability to understand and give consent for treatment. If the study were repeated after this change, the findings may be different as the study population may include people with less severe opiate use disorder due to the less specific criteria for maintenance treatment.
NEXT STEPS
To draw firmer conclusions on the social and economic benefit of maintenance treatment, future longitudinal research should focus on studying if maintenance therapy helps people with opiate use disorders return to and stay in the workforce.
BOTTOM LINE
- For individuals & families seeking recovery: Proper use of maintenance therapy may help one remain in recovery.
- For scientists: A direct comparison between patients on opioid agonist treatment who do and do not find stable work is needed to better understand this issue. Longitudinal studies are needed to assess the impact of methadone and buprenorphine on the workforce more broadly. Economic studies should evaluate the potential benefit of these treatments and their ability to alleviate the economic burden of opioid dependence.
- For policy makers: Since maintenance therapy is an evidence-based treatment method for opiate use disorder, it is important that employers do not discriminate against people who are prescribed these medications.
- For treatment professionals and treatment systems: Discuss maintenance therapy with your patient to see if it is a good option for them. Concurrently addressing factors that may increase their motivation for change will also help them progress in other domains of their life in addition to achievements directly related to their opioid use.
CITATIONS
Blom, N. M., Chassler, D., & Lundgren, L. M. (2014). Factors associated with work and taking prescribed methadone or buprenorphine among Swedish opiate addicts. Evaluation and program planning.
