
Substance Use Disorder & Schizophrenia: Is Cognitive Enhancement Therapy a Viable Option for Treating Comorbidity?
People diagnosed with schizophrenia often experience comorbid substance use issues with more than 50% of patients misusing alcohol and other drugs.
Both health issues can cause executive and problem-solving impairments which in turn inhibit the patient’s ability to recover.
Despite the need for effective treatments to address both issues concurrently, patients with substance use disorders are often excluded from randomized controlled trials (RCTs) evaluating the efficacy of schizophrenia therapies, and those with psychotic disorders are often excluded from substance use disorder (SUD) outcome studies.
Cognitive enhancement therapy (CET), a treatment previously evaluated in non-substance misusing schizophrenia patients, works to rehabilitate social cognitive and neurocognitive deficits and provides benefits for social and vocational functioning.
To see if these benefits hold among substance misusing schizophrenic patients, Eack and colleagues conducted a pilot randomized controlled trial (RCT) to test the feasibility of cognitive enhancement therapy (CET) in a population that is difficult to engage and retain in care.
Thirty one patients with schizophrenia (n = 17) and schizoaffective disorder (n = 14) were enrolled in an 18 month randomized feasibility trial evaluating the efficacy of cognitive enhancement therapy (CET) versus treatment as usual (TAU). Adults meeting DSM-IV criteria for schizophrenia or schizoaffective disorder with moderate or higher severity for cannabis or alcohol use (≥4 on the Addiction Severity Index) and not misusing other illicit substances were deemed eligible for randomization.
The inclusion criteria focused on cannabis and alcohol, the two most commonly misused substances among schizophrenic patients in the U.S. Over 18 months, cognitive enhancement therapy (CET) consisted of 60 hours of computer-based training in attention, memory, and problem-solving. It also included social-cognitive groups with psychoeducational lectures and homework assignments as well as neurocognitive training taking place in pairs.
The content focused on both schizophrenia and substance use disorders to reflect the needs of the study population. TAU included mental health and social services such as psychiatry services, case management, and individual support therapy. Patients were assessed on cognitive and behavioral measures and frequency of substance use every six months.
Participants were 38 years old on average, 71% male, and about half White. All but two met DSM-IV criteria for substance abuse or dependence. Over two thirds were actively using cannabis or alcohol at the start of the study. There were no significant differences in baseline demographic or clinical characteristics between groups. Of the 31 patients completing baseline assessments, 28 received treatment with 19 randomized to CET and 9 to TAU. More patients were randomized to CET in order to facilitate the creation of social-cognitive groups. Individuals completing the study had lower pre-treatment drug addiction severity scores.
The authors used composite indexes of cognition and behavior to compare the effects of CET versus TAU. The effects on neurocognitive and social-cognitive functioning favored CET. While not achieving statistical significance, the largest improvements for neurocognitive change were in processing speed and verbal learning with large effect sizes (d = 0.92 and 0.90, respectively).
Cognitive enhancement therapy (CET) patients showed significantly greater improvements on understanding emotions (d = 1.17) and managing emotions (d = 0.97) compared to treatment as usual (TAU) patients. Significant improvements favoring CET were also seen in social adjustment, specifically in major role functioning (d = 1.85) and global assessment of functioning (d = 1.02). There were no significant differences between groups for symptom improvement.
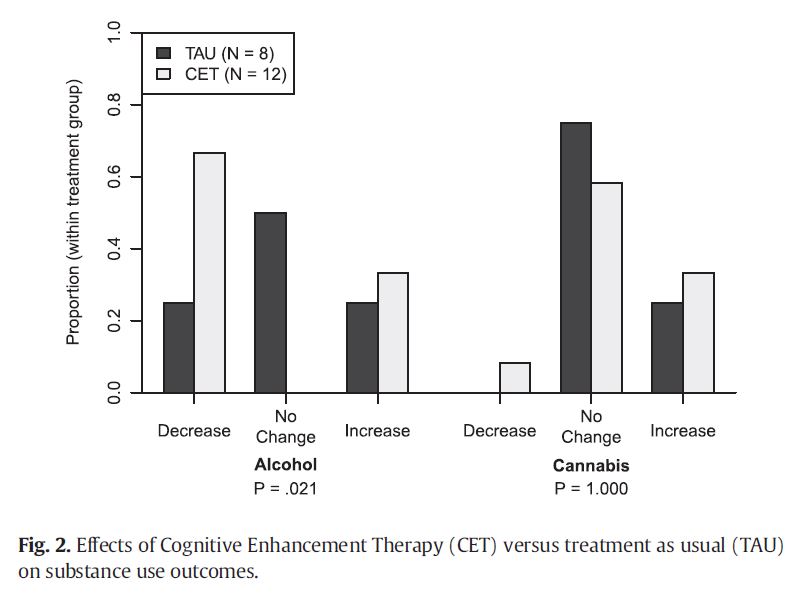
While there was not a significant difference between groups for the number of abstinent participants by the end of the study, the cognitive enhancement therapy (CET) group had a significantly greater proportion of patients reporting reduced number of days using alcohol in the previous month with 67% decreasing use versus 25% in the treatment as usual (TAU) group.
Source: (Eack et al. 2015)
IN CONTEXT
In the U.S., the lifetime prevalence of substance use disorder among people with schizophrenia ranges between 50 and 59%, compared to 16% in the general population.
This study adds important information to what is known on treatment for people suffering from these co-occurring disorders, a field where information is limited.
- LIMITATIONS
-
- The authors noted that it was difficult to recruit and retain patients for this study. Due to the nature of the health condition, many researchers exclude patients with comorbid schizophrenia and substance use issues from randomized controlled trials (RCT) for this very reason despite the need for more research on best treatment practices for this patient population.
- This feasibility trial demonstrated that once such patients are retained in treatment, there are benefits conferred by cognitive enhancement therapy (CET) over TAU for both cognitive functioning and alcohol consumption. However, these results may not be generalizable since the study population was very specific; it is unknown if CET would be as useful in schizophrenia patients misusing substances other than alcohol and marijuana or with more severe addiction since those completing the trial had lower levels of addiction severity.
NEXT STEPS
Since this is a difficult population to engage in care, adequately powered larger trials will need to have innovative recruitment plans and methods to reduce attrition.
BOTTOM LINE
- For individuals & families seeking recovery: Cognitive enhancement therapy (CET) appears to be worth the time investment and is unlikely to hurt.
- For scientists: There is a lack of RCTs evaluating treatments for patients with co-occurring schizophrenia and substance use disorders or other hazardous use. While difficult to engage in care, it is important that therapies are evaluated in this population in order to improve current practices.
- For policy makers: Since substance misuse is a common problem among patients with schizophrenia, improvements need to be made to better serve this population.
- For treatment professionals and treatment systems: Since patients with co-occurring psychotic spectrum and substance use disorders can be difficult to engage and retain in treatment, more outreach efforts may be needed to deliver the best care.
CITATIONS
Eack, S. M., Hogarty, S. S., Greenwald, D. P., Litschge, M. Y., McKnight, S. A., Bangalore, S. S., . . . Cornelius, J. R. (2015). Cognitive Enhancement Therapy in substance misusing schizophrenia: results of an 18-month feasibility trial. Schizophr Res, 161(2-3), 478-483. doi: 10.1016/j.schres.2014.11.017
